
Article Figures & Data
Figures
- Figure 1.
The structure of the Australian health care system and its flow of funds. *The tax rebate is not an expense of the Australian Government Department of Health and Ageing, but is a tax expenditure of the Australian Government. Source: Australian Institute of Health and Welfare 2007. Health expenditure Australia 2005–06. Health and Welfare Expenditure series no. 30. Cat. No. HWE 37. Canberra: AIHW.
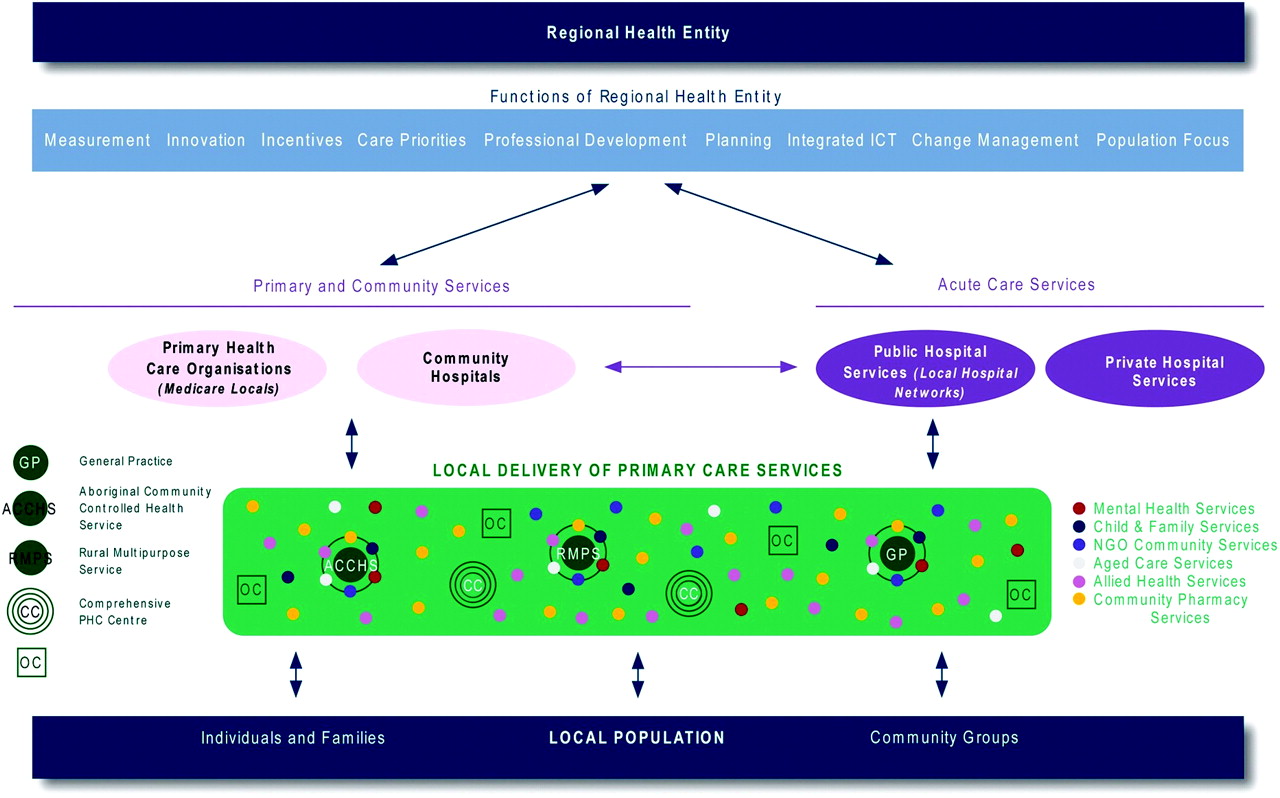
- Figure 2.
Functions of regional health entities. ICT, information communication technology; NGO, nongovernment organization.

Tables
Characteristic National Primary Care Strategy (Australia) (6) Primary Health Care Strategy (New Zealand) (11) Patient Centered Medical Home (USA) (12) Royal College of General Practice (England) (13) Clinical care Population health–based focus Voluntary patient enrolment Enrolled populations Enrolled populations Identifies and aims to reduces health inequalities ✓ ✓ ✓ Delivers uniformly accessible, patient-centered, continuity of care Better access to primary health care services
There are key issues in relation to relocation of hospital service modelsOffer access to comprehensive services to improve, maintain, and restore people's health Enhanced access is available through systems, eg, open scheduling, expanded hours, and new options for communication Provide access including urgent care
Major after-hours problems
ResponsivenessClinical care well integrated and coordinated with secondary care Explicit statements on integration of primary/secondary services to improve coordination, continuity, and collaboration Coordinate care across service areas
Low level coordination and integration to dateCare is coordinated and/or integrated across all elements of health care
Personal physician
Whole-person orientationPractices collaborating and working together Must have a primary care workforce appropriate to local conditions and need GP led most appropriate and accessible blend of multidisciplinary team care Develop the primary health care workforce Physician-directed medical practice, ie, the physician leads a team of individuals who collectively provide care GP-led, integrated, and expanded multidisciplinary teams Provides high-quality, safe, evidence-based care Integrated quality and safety tools Continuously improve quality using good information Quality and safety are hallmarks of the medical home Culture of quality and safety of care Education and training Appropriately resourced and vertically integrated professional development and training Commitment across PHC teams to training and education Limited commitment to training and education Culture of education, teaching, and training ICT Has ICT systems that integrate information effectively across the health care system Improved ICT to support continuity of care via personally controlled EHR Not included ICT infrastructure to support care Governance Has an appropriate governance model with local engagement, responsibility, and appropriate decision-making capacity, accepting of and managing local diversity and complexity Meso-level primary care organizations to facilitate: Local engagement, patient and community participation; and provider representation
Linkage between micro- and macrosectors of the system divisions (n = 111 in 2010); transitioning to larger “Medicare locals” in 2011Meso-level primary health care organizations (n = 32 in 2011) who have shared governance with clinicians, community, and Maori groups
There is limited ability to accept responsibility for complex decision makingAn expectation of accountable care organizations but untested, which currently limits population focus and inequality reduction Meso-level Primary Care Trusts (n = 152 in 2010) are transitioning to smaller GP consortia led and championed by local clinicians Uses a funding model that encourages maximal management of complex disease in the community, an outcomes focus, and health promotion/disease prevention Non–fee-for-service physician payment (capitation)
Correct funding signals and incentives across the system to maintain care within the community
Variety of funding models to fit local circumstance and prioritiesMixed funding model with government funding applied by variation of capitation
Patients pay fees for services
Some limited quality and performance paymentsPayment reform recognizing the added value provided to patients who have a patient-centered medical home Commissioning, resource management, and coordination of care EHR, electronic health record; GP, general practitioner; ICT, information communication technology; PHC, primary health care.
Function Activity Clinical care Population health focus • Population health activities • Community engagement • Patient enrolment Reduce health inequalities • Local initiatives, eg, Closing the Gap (Australia) Improve access • After-hours care • Contracting with providers Integrated care • Disease management • Coordinated and integrated service delivery Multidisciplinary workforce • Access to GP-led expanded PHC teams Quality and safety • Clinical and practice support • Monitoring quality and accreditation Integrated education and training Vertically integrated professional development • Multidisciplinary continuous professional development Integrated communications technology Enhance clinical data sharing • Electronic discharge summary and referrals; personally controlled electronic health record Integrated governance Improve linkage • Act as link between macro- and microlevels of the system • Link between primary and secondary sectors • Link between “horizontal” components of the system, eg, housing and employment Allocation of regional budgets • Commissioning services Local/regional decision making • Run by independent boards GP, general practitioner; PHC, primary health care.




{kind=link}
{kind=link}