
Article Figures & Data
Figures
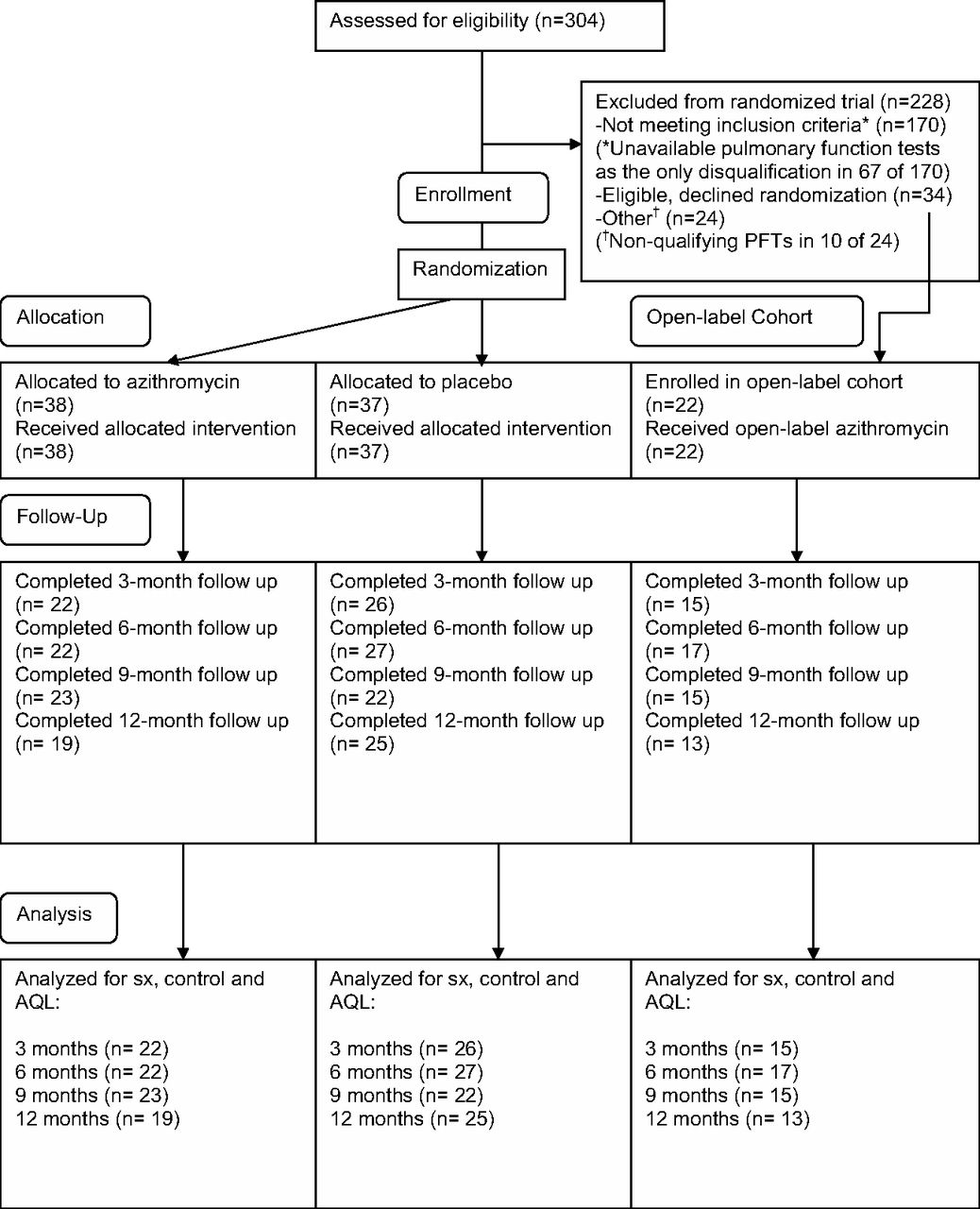
- Figure 1.
CONSORT diagram. *Unavailable pulmonary function tests (PFTs) as the only disqualification of 67 of 170. †Nonqualifying PFTs in 10 of 24.
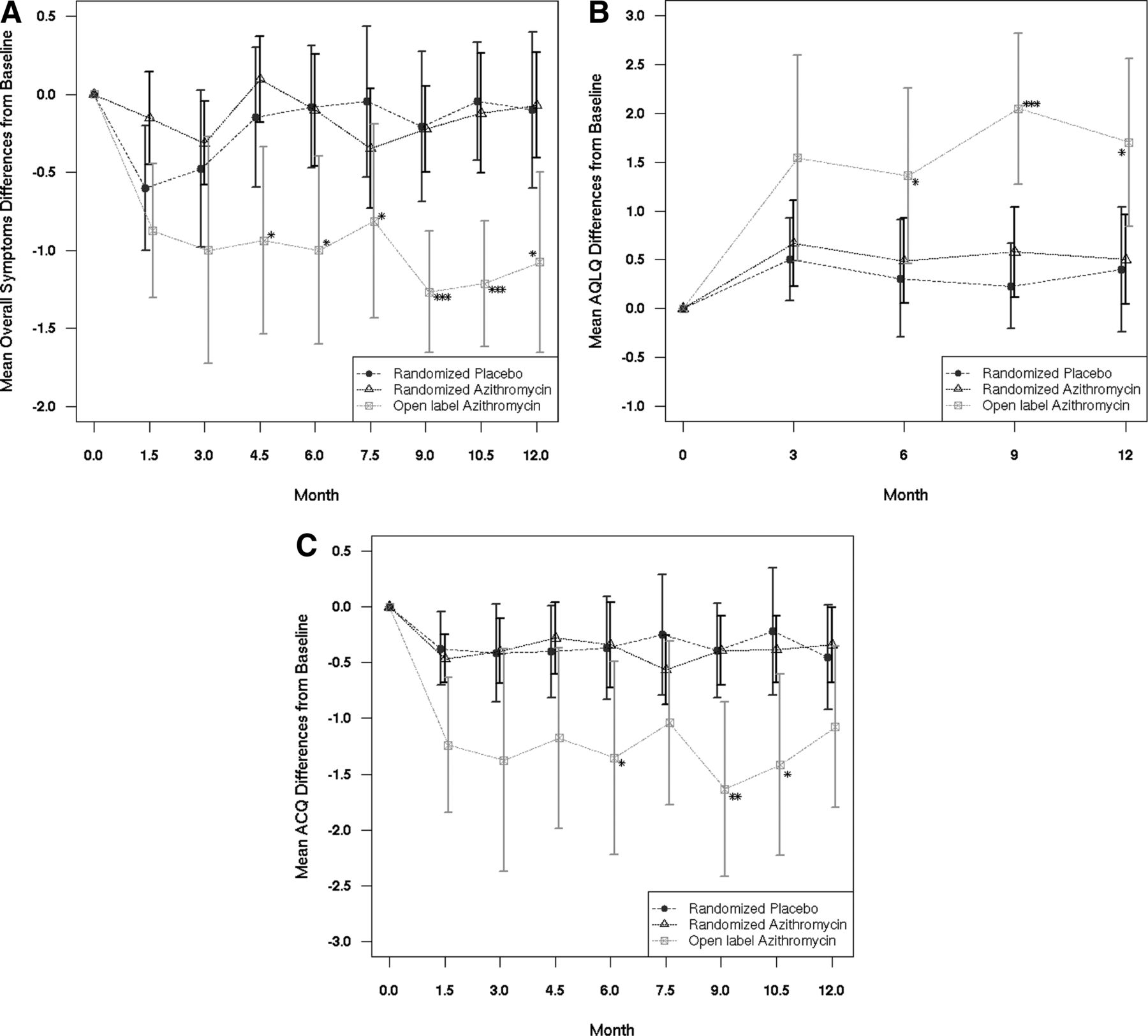
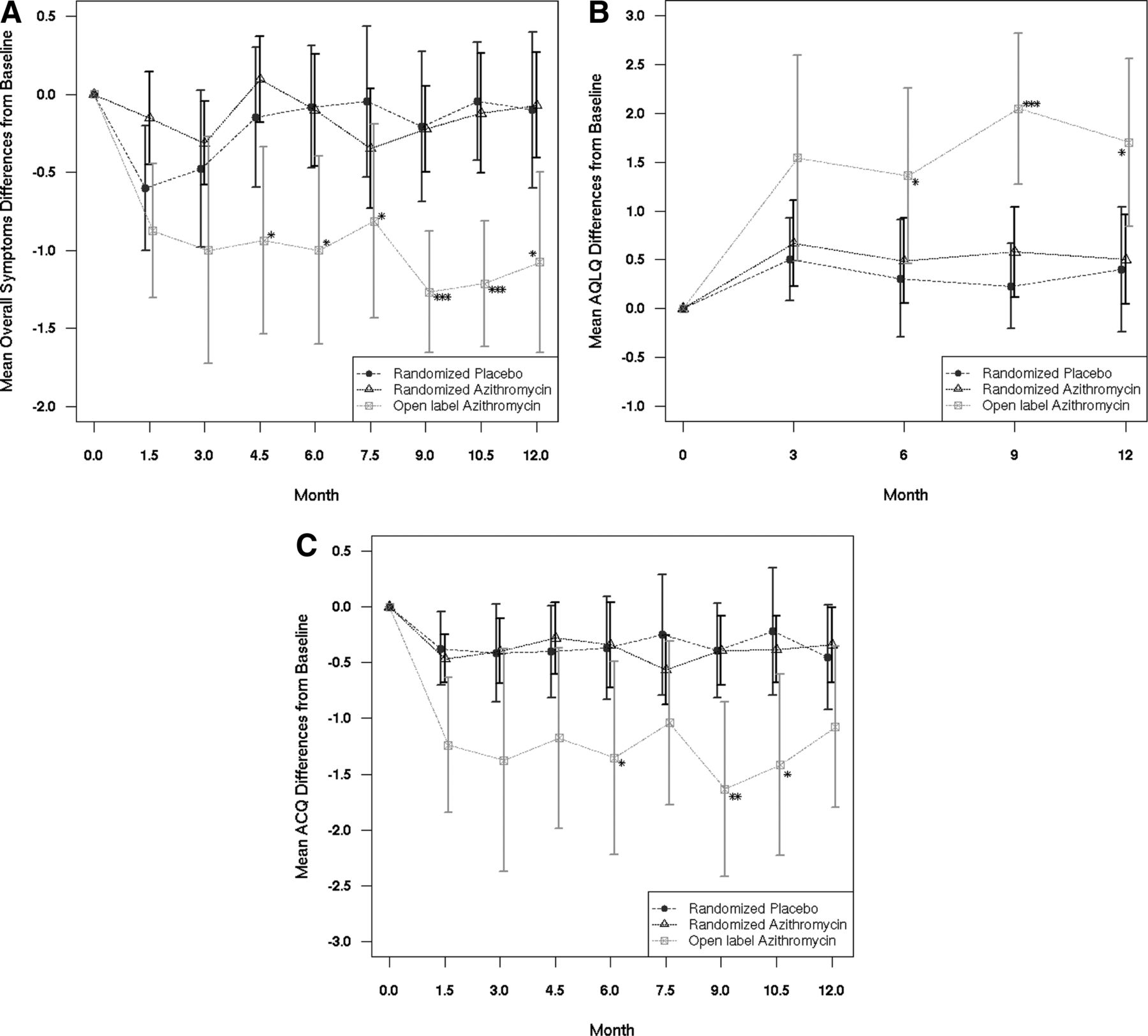
- Figure 2.
Differences from baseline for asthma symptoms, quality of life, and control. A: Symptoms—rating of overall asthma symptoms for the past 24 hours (negative numbers indicate decreased symptoms and hence improvement). B: Quality of life— Juniper Asthma Quality of Life Questionnaire (AQLQ); positive numbers indicate higher quality of life scores and hence improvement). C: Control—Juniper Mini-Asthma Control Questionnaire (ACQ; negative numbers indicate better control and hence improvement). See Methods for details. Symbols represent the mean paired differences from baseline. Bars represent 95% confidence intervals. *P < 0·05, **P < 0·01, ***P < 0·001 (t tests, placebo versus open label).
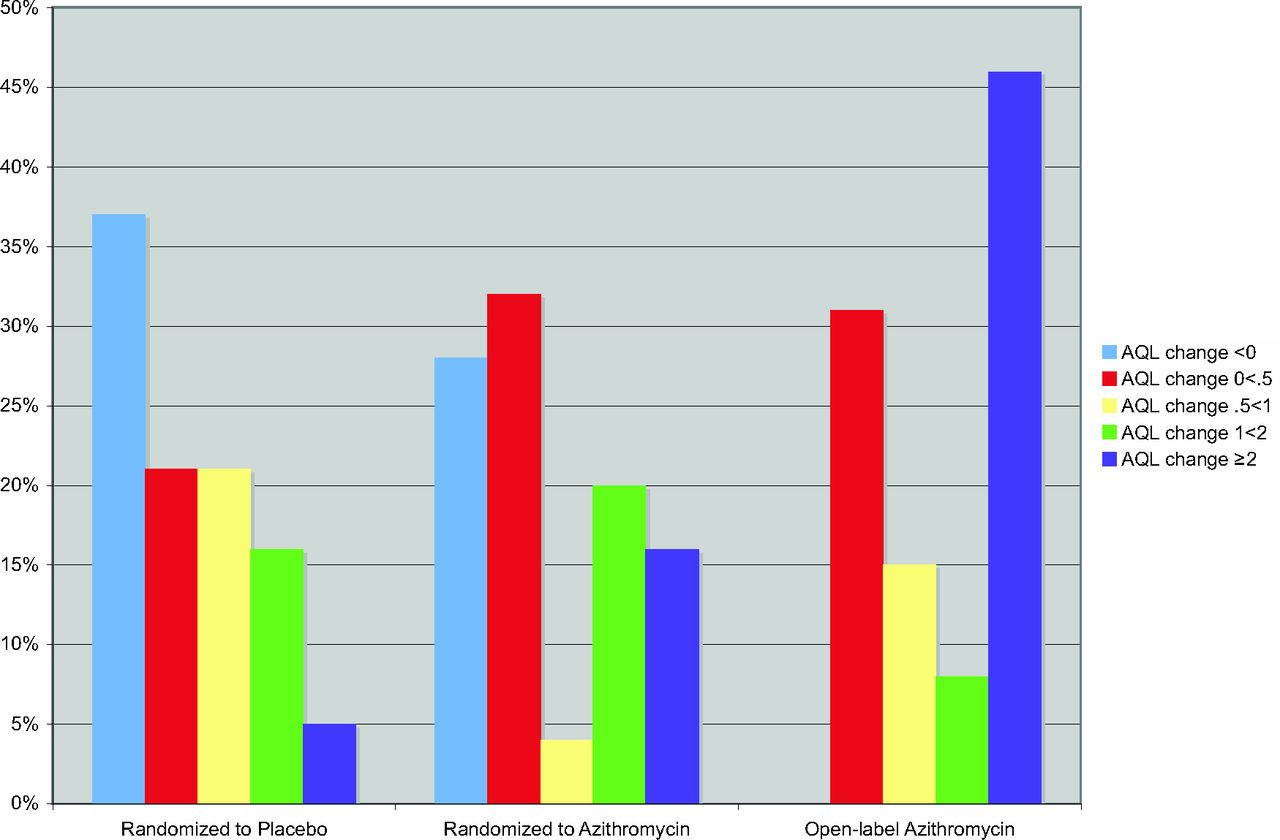
- Figure 3.
Improvement in asthma quality of life (AQL) after azithromycin treatment may be “all or none.” AQL change scores from baseline to 12 months after enrollment (9 months after treatment completion) are defined as follows: “AQL change <0” = AQL change worse than baseline; “AQL change 0 < .5” = change between 0 to <.5 units; “AQL change 0.5 < 1” = change between 0.5 to <1 (change of 0.5 unit is considered the minimum clinically important change); “AQL change 1 < 2” = change between 1 and 2 (change >1.5 units represents a large change); “AQL change ≥2” = change of 2 units or more. The contrasting patterns between placebo and open-label azithromycin were statistically significant, as noted in the text. The differences between randomized azithromycin and placebo were not statistically significant, as noted in the text.

Tables
Criteria Inclusions Adults ≥18 years of age with physician-diagnosed asthma (symptomatic ≥2 days per week and/or ≥2 nights per month or in exacerbation)
Objective evidence for reversible airway obstruction (≥12% and ≥200 mL change in FEV18 and/or a 25% and 60 L/min change in PEFR9) either spontaneously or after treatment
Asthma for at least 6 months before enrollment
Exclusions Not English literate or has no email address or Internet access
Macrolide allergy
Pregnant or lactating
≥4 weeks of continuous use of macrolides, tetracyclines, or quinolones within 6 months of randomization
Asthma symptoms less than 6 months' duration
Unstable asthma requiring immediate emergency care
Comorbidities likely to interfere with study assessments or follow-up (eg, cystic fibrosis, obstructive sleep apnea requiring CPAP, cardiomyopathy, congestive heart failure, terminal cancer, alcohol or other drug abuse, or any other serious medical condition that, in the opinion of the study physician, would seriously interfere with or preclude assessment of study outcomes or completion of study assessments)
Medical conditions for which macrolide administration may possibly be hazardous (eg, acute or chronic hepatitis, cirrhosis, or other liver disease; chronic kidney disease; or history of prolonged cardiac repolarization and QT interval or torsades de pointes).
Specified medications for which close monitoring has been recommended in the setting of macrolide administration (digoxin, theophylline, warfarin, ergotamine or dihydroergotamine, triazolam, carbamazepine, cyclosporine, hexobarbital, or phenytoin)
Outcomes Asthma symptom scores (0 = none, 1 = mild, 2 = moderate, 3 = severe, 4 = worst ever) within the past 24 hours; every 1.5 months
AQL (Juniper AQL questionnaire)10 within the past 2 weeks; every 3 months
Asthma control (mini-Juniper Asthma Control Questionnaire, without pulmonary function)11,12 within the past week; every 3 months
Exacerbations (a steroid burst, an unscheduled or emergency visit and/or a hospitalizations for asthma) within the past 1.5 months; every 1.5 months
Other respiratory illnesses within the past 1.5 months; every 1.5 months
Off-study antibiotic use within the past 1.5 months; every 1.5 months
Adverse events within the past 1.5 months; every 1.5 months
Use of asthma-controller medications (oral or inhaled steroids, LABAs, or antileukotriene agents) within the past 3 months; every 3 months
Self-reported improvement in asthma (compared with baseline) within the past 3 months; every 3 months
AQL, asthma quality of life; CPAP, continuous positive airway pressure; FEV1, forced expiratory volume in 1 second; LABA, long-acting bronchodilators; PEFR, peak expiratory flow rate.
Characteristic Randomized Placebo (n=37) Randomized Azithromycin (n=38) Open-Label Azithromycin (n=22) P* Age(years), mean(SD) 47.4 (14.2) 45.7 (15.5) 45.4 (15.2) .621/.745 At asthma diagnosis 24 (<1–59) 24 (<1–58) 28 (11–59) .603/.104 Diagnosis at age ≥18 years 21 (57) 24 (63) 19 (86) .641/.023 Male sex 13 (35) 11 (29) 12 (55) .626/.078 Smoking status .187/.028 Never 13 (35) 20 (53) 16 (73) Former 19 (51) 12 (32) 6 (27) Current 5 (14) 6 (16) 0 (0) White race 33 (89) 36 (95) 18 (82) .430/.227 Education, median years (range) 15 (10–20) 14 (12–22) 17 (12–25) .550/<.001 ≥High school graduate 35 (95) 38 (100) 21 (100) .240/1.000 Chronic sinusitis 11 (30) 14 (37) 17 (77) .626/<.001 Atopy Allergy tested 18 (53) 18 (49) 19 (86) .814/.003 Negative 2 (11) 1 (6) 6 (32) .759/.003 Positive for 1–3 positive 4 (22) 3 (17) 8 (42) Positive for ≥4 12 (67) 14 (78) 5 (26) Infectious asthma† 6 (16) 17 (46) 13 (59) .011/.024 Exacerbations (previous 2 years), n (%) 24 (65) 26 (68) 14 (64) .809/.802 Hospitalized 0 (0) 2 (5) 4 (18) .493/.023 Emergency visit 14 (38) 19 (50) 9 (41) .355/1.000 Steroid burst 22 (59) 24 (63) 13 (59) .815/1.000 Baseline asthma severity, n (%) Day symptom frequency‡ .675/.009 Mild to moderate 35 (95) 34 (89) 15 (68) Severe 2 (5) 4 (11) 7 (32) Night symptom frequency‡ 1.000/.046 Mild to moderate 33 (89) 33 (87) 15 (68) Severe 4 (11) 5 (13) 7 (32) Coexisting COPD 8 (22) 5 (13) 2 (9) .375/.509 Lung function, mean (SD) FEV1, L (n) 18 19 7 Low§ 2.24 (1.25) 2.33 (1.05) 2.48 (1.19) .812/.688 % Change‖ 42 (47.4) 26 (25.9) 33 (26.8) .214/.969 PEFR, L/min (n with value) 25 25 18 Low§ 258 (110) 276 (110) 300 (105) .566/.281 % Change‖ 62 (56) 63 (49) 85 (63) .927/.140 Any controller medication 33 (89) 25 (66) 19 (86) .026/.549 Inhaled corticosteroid 30 (81) 24 (63) 18 (82) Long-acting bronchodilator¶ 26 (70) 14 (37) 15 (68) Leukotriene inhibitor 8 (22) 9 (24) 6 (27) Oral prednisone 4 (11) 2 (5) 1 (5) Baseline asthma measures, mean (SD)** Overall asthma symptoms 1.48 (0.94) 1.42 (0.77) 2.06 (0.73) .744/.005 Asthma quality of life 4.97 (1.28) 4.98 (1.27) 4.12 (1.29) .988/.023 Asthma control 1.56 (1.02) 1.75 (0.93) 2.26 (1.35) .424/.090 Values provided as n (%) unless otherwise indicated.
↵* P values comparing randomized placebo versus randomized azithromycin/randomized cohort versus open-label cohort.
↵† History showed first asthma symptoms began after an acute respiratory illness.
↵‡ Day: mild = ≥2 days/week to less than daily; moderate = ≥1 per day to less than continuous; severe = continuous. Night: mild = ≥2 per month to ≤1 per week; moderate = >1 per week to ≤1 per night; severe = >1 per night.
↵§ Before bronchodilator use or lowest spontaneous value.
↵‖ Based on data after bronchodilator use or highest spontaneous value. Some subjects had either FEV1 or PEFR values, not both.
↵¶ All subjects using a long-acting bronchodilator also were using an inhaled corticosteroid.
↵** See Methods for definitions.
COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; PEFR, peak expiratory flow rate.
Randomized Placebo Randomized Azithromycin Open-label Azithromycin P, Placebo vs Randomized Azithromycin P, Placebo vs Open-Label Change in overall asthma symptoms, from baseline Week 6 −0.60 (1.07) (n=30) −0.15 (0.83) (n=33) −0.88 (0.81) (n=16) .071/.071† .333/.428† Week 12 −0.48 (1.16) (n=23) −0.31 ((0.74) (n=32) −1.0 (1.37) (n=16) .551/.580† .223/.723† Week 18 −0.15 (1.13) (n=27) 0.10 (0.75) (n=31) −0.94 (1.12) (n=16) .344/.178† .034/.161† Week 24 −0.08 (0.95) (n=25) −0.10 (0.96) (n=30) −1.0 (1.17) (n=17) .939/.599† .012/.013† Week 30 −0.05 (1.09) (n=22) −0.34 (1.01) (n=29) −0.81 (1.17) (n=16) .322/.280† .048/.870† Week 36 −0.21 (1.14) (n=24) −0.22 (0.70) (n=27) −1.27 (0.70) (n=15) .959/.942† .001/.017† Week 42 −0.04 (0.88) (n=23) −0.12 (0.93) (n=25) −1.21 (0.70) (n=14) .770/.858† <.001/.001† Week 48 −0.10 (1.07) (n=20) −0.07 (0.88) (n=29) −1.07 (0.95) (n=13) .916/.758† .011/.067† Change in AQL, from baseline Week 12 0.50 (0.95) (n=22) 0.67 (1.10) (n=26) 1.54 (1.91) (n=15) .584/.682† .067/.180† Week 24 0.31 (1.36) (n=22) 0.49 (1.11) (n=27) 1.36 (1.75) (n=17) .618/.382† .049/.151† Week 36 0.23 (1.02) (n=23) 0.58 (1.04) (n=22) 2.05 (1.40) (n=15) .261/.342† <.001/.001† Week 48 0.40 (1.33) (n=19) 0.50 (1.10) (n=25) 1.70 (1.42) (n=13) .784/.929† .015/.068† Change in asthma control, from baseline Week 6 −0.37 (0.88) (n=30) −0.46 (0.60) (n=33) −1.24 (1.14) (n=16) .634/.654† .014/.009† Week 12 −0.41 (1.01) (n=23) −0.40 (0.80) (n=32) −1.38 (1.87) (n=16) .946/.998† .075/.324† Week 18 −0.40 (1.05) (n=27) −0.28 (0.88) (n=31) −1.18 (1.53) (n=16) .637/.573† .085/.179† Week 24 −0.37 (1.12) (n=25) −0.34 (1.03) (n=30) −1.35 (1.69) (n=17) .925/.536† .045/.034† Week 30 −0.25 (1.22) (n=22) −0.56 (0.81) (n=29) −1.04 (1.38) (n=16) .307/.281† .078/.163† Week 36 −0.39 (1.00) (n=24) −0.39 (0.79) (n=27) −1.63 (1.41) (n=15) 1.000/.852† .007/.015† Week 42 −0.22 (1.32) (n=23) −0.38 (0.72) (n=25) −1.42 (1.41) (n=14) .604/.817† .016/.068† Week 48 −0.45 (1.00) (n=20) −0.34 (0.88) (n=29) −1.08 (1.20) (n=13) .692/.525† .132/.379† AQL improved ≥1 unit, n/N (%) Week 12 5/22 (23) 11/26 (42) 9/15 (60) .221/.136‡ .038/.098‡ Week 24 6/22 (27) 8/27 (30) 11/17 (65) 1.000/.745‡ .026/.048‡ Week 36 5/23 (22) 6/22 (27) 12/15 (80) .738/.738‡ .001/.003‡ Week 48 4/19 (21) 9/25 (36) 7/13 (54) .335/.386‡ .072/.116‡ Asthma control improved ≥1 unit, n/N (%) Week 6 6/30 (20) 4/33 (12) 9/16 (56) .498 /.421‡ .021/.010‡ Week 12 7/23 (30) 7/32 (22) 11/16 (69) .539/.531‡ .025/.045‡ Week 18 7/27 (26) 4/31 (13) 9/16 (56) .315/.437‡ .059/.054‡ Week 24 6/25 (24) 10/30 (33) 10/17 (59) .556/.144‡ .029/.017‡ Week 30 5/22 (23) 9/29 (31) 8/16 (50) .546/.502‡ .098/.105‡ Week 36 5/24 (21) 6/27 (22) 10/15 (67) 1.000/.875‡ .007/.009‡ Week 42 6/23 (26) 7/25 (28) 8/14 (57) 1.000/.862‡ .085/.152‡ Week 48 5/20 (25) 8/29 (28) 5/13 (38) 1.000/.980‡ .461/.998‡ All values are mean (SD) unless otherwise indicated.
↵* See Methods for definitions.
↵† Univariate (t test)/multivariate (analysis of variance); controlled for age, sex, and ever-smoking at each time point, as well as for controller medication use at weeks 12, 24, 36, and 48 (controller data is unavailable for other time points).
↵‡ Univariate (Fisher exact test)/multivariate (logistic regression); controlled for age, sex, and ever-smoking at each time point, as well as for controller medication use at weeks 12, 24, 36, and 48 (controller data is unavailable for other time points).
AQL, asthma quality of life.
Side Effects, n (%) Randomized Placebo Randomized Azithromycin Open-Label Azithromycin P† Nausea .016/.008/.458 None 31 (91) 25 (71) 12 (60) Mild to moderate 1 (3) 9 (26) 6 (30) Severe 2 (6) 1 (3) 2 (10) Vomiting 1.000/.128/.456 None 32 (94) 33 (94) 18 (90) Mild to moderate 0 (0) 1 (3) 2 (10) Severe 2 (6) 1 (3) 0 (0) Stomach pain .076/.001/.196 None 30 (88) 24 (69) 9 (45) Mild to moderate 3 (9) 10 (29) 10 (50) Severe 1 (3) 1 (3) 1 (5) Diarrhea .106/.002/.196 None 29 (85) 23 (66) 9 (45) Mild to moderate 3 (9) 10 (29) 10 (50) Severe 2 (6) 2 (6) 1 (5) Rash .743/.046/.420 None 33 (97) 33 (94) 16 (80) Mild to moderate 0 (0) 2 (6) 3 (15) Severe 1 (3) 1 (3) 1 (5) Swelling .239/.716/.128 None 32 (94) 35 (100) 18 (90) Mild to moderate 1 (3) 0 (0) 2 (10) Severe 1 (3) 0 (0) 0 (0) Hearing loss .743/1.000/.999 None 32 (94) 34 (97) 19 (95) Mild to moderate 1 (3) 1 (3) 1 (5) Severe 1 (3) 0 (0) 0 (0) Vaginal candidiasis .670/1.000/.999 None 20 (91) 21 (84) 7 (88) Mild to moderate 3 (9) 4 (16) 1 (13) Severe 0 (0) 0 (0) 0 (0) - Table 5. Randomized Trials of Second-Generation Macrolides/Azalides for Asthma: Study Designs
Reference Age Group Sampling Frame Asthma Severity Subjects (n) Design RX/Duration Observation after RX Shoji (1999)17 Adults Hospital asthma clinic Mild/moderate 14 Single site; double-blind cross-over (4-week washout) Roxithromycin, 300 mg daily or placebo/8 weeks None Aspirin-intolerant asthma Amayasu (2000)18 Adults Not stated (hospital asthma clinic[s]?) Mild/moderate 17 Single site; double-blind cross-over (4-week washout) Clarithromycin, 200 mg daily or placebo/8 weeks None Black (2001)19 18–60 years old Majority of subjects recruited from the general population; recruitment method(s) not specified Moderate/severe 232 Multinational; double-blind, parallel groups (Australia, New Zealand, Italy, Argentina) Roxithromycin, 300 mg daily or placebo/6 weeks 24 weeks Kraft (2002)20 Young adults Subjects recruited from the general population via advertising Not stated
Mean FEV1%pred = 69.3
35% were taking ICS52 Single site; double-blind parallel groups
All subjects underwent bronchoscopy before and after prescriptionClarithromycin, 1000 mg daily or placebo/6 weeks None Kostadima (2004)21 18–70 years old Not stated (referral speciality setting) Not stated, probably mild 63 Single site; double-blind, parallel groups Clarithromycin, 500 or 750 mg daily or placebo/8 weeks None Mean FEV1%pred ∼85% Subjects using albuterol >2 times weekly were excluded Hahn (2006)22 ≥18 years old Community-based healthcare settings Mostly mild/moderate 46 Multisite; double-blind, parallel groups Azithromycin, 600 mg daily for 3 days then 600 mg weekly or placebo/6 weeks 12 weeks Piacentini (2007)23 Children Inpatient setting Not stated 16 Single site; double-blind, parallel groups Azithromycin, 10 mg/kg/day for 3 of 7 days or placebo/8 weeks None Simpson (2008)24 Adults Specialty outpatient clinic Severe refractory 45 Single site; double-blind, parallel groups Clarithromycin, 1000 mg daily or placebo/8 weeks 4 weeks Stratified by high (>61%)/low induced sputum neutrophil proportion Strunk (2008)25 Children Academic asthma centers Moderate/severe 55 Multisite; double-blind, parallel groups
This was a study of macrolide as a “steroid-sparing” agent, not as an antimicrobialAzithromycin, 250–500 mg daily or montelukast 5–10 mg daily of placebo/24 weeks 6 weeks Sutherland (2010)26 18–60 years old Academic asthma centers Suboptimally controlled asthma 92 Multisite; double-blind, parallel groups
Stratified on Mpn or Cpn PCR± (bronchoscopic sampling) The study was underpowered to test PCR+ casesClarithromycin, 1000 mg daily or placebo/16 weeks None Hahn (2012), current study ≥18 years old Community-based healthcare settings Mild/moderate (randomized) 75 randomized 22 open-label Multisite; double-blind, parallel groups Azithromycin, 600 mg daily for 3 days then 600 mg weekly or placebo/12 weeks 36 weeks Severe (open-label) %pred, percent of the predicted value; Cpn, Chlamydia pneumoniae; FEV1, forced expiratory volume in 1 second; ICS, inhaled corticosteroid; Mpn, Mycoplasma pneumoniae; PCR, polymerase chain reaction.
- Table 6. Randomized Trials of Second-Generation Macrolides/Azalides for Asthma: Exclusions, Outcomes, and Results
Reference Exclusions* Outcomes Reported Results of Macrolide Treatment Shoji (1999)17 Smokers Blood eosinophils and ECP Decreased eosinophils/ECP Controller medication Sputum cell counts and ECP Decreased eosinophils/ECP (No differences in sputum neutrophils) Sulpyrine provocation test Not improved (No patient-oriented outcomes reported) Amayasu (2000)18 Smokers Blood eosinophils and ECP Decreased eosinophils/ECP Aspirin sensitivity Sputum cell counts and ECP Decreased eosinophils/ECP ARI for 6 weeks BHR Improved Any asthma controller medication Pulmonary function Not improved Overall asthma symptoms Improved Black (2001)19 FEV1 <50% predicted Pulmonary function(PEF) Improvement at end of prescription that waned after prescription C. pneumoniae IgG < 1:64 and IgA < 1:16 Pulmonary function(FEV1) Not improved Smoking ≥20 pack-years Asthma symptoms Not improved Bronchiectasis AQL Not improved Prednisone burst in previous month Respiratory illness Kraft (2002)20 Smoking >5 pack years PCR+ for Mpn or Cpn 31 of 55 were PCR+ for Mpn and/or Cpn Any cigarette within 2 years Pulmonary function Improved FEV1 in PCR+ subject subgroup Any lung comorbidity Lung inflammation Decreased inflammatory cytokines Any LRTi within 3 months (No patient-oriented outcomes reported) Kostadima (2004)21 Asthma diagnosis <1 year ago BHR Decreased BHR Not on ICS Pulmonary function Not improved Rescue inhaler >2 times weekly Serum free cortisol Not affected Any smoking history (No patient-oriented outcomes reported) Any other medication FEV1 < 50% predicted Any ARI or exacerbation within 4 weeks before or during the study Hahn (2006)22 None AQL No improvement Rescue medication use No improvement Cpn IgG and IgA antibodies Baseline IgA predicted worsening symptoms Overall asthma symptoms Improved at end of prescription and persisted after prescription Piacentini (2007)23 Oral steroids in the preceding 3 months or during the study Lung function No improvement Signs of airway infection in the preceding month or during the study BHR Improved Lung inflammation Reduced induced sputum neutrophils Simpson (2008)24 Current smoking Sputum inflammatory markers Decreased airway IL-8 and neutrophils History of smoking, >5 pack-years Pulmonary function No improvement Antihistamine medication BHR No improvement Asthma control No improvement Asthma symptoms Decreased wheezing after prescription AQL Improved (NNT = 6 for ≥0.5 units improvement) It was unclear whether the AQL was reported at the end of the prescription or after the prescription Strunk (2008)25 No controller medication Time to inadequate control after steroid step-down No improvement in asthma control (futility analysis) FEV1 < 50%pred Recruitment was discontinued early (292 screened, only 55 randomized) >3 hospitalizations in past year Sinus surgery in past year Lung comorbidities Sutherland (2010)26 Exacerbation within 6 weeks Asthma control No differences in asthma control ARI within 6 weeks Pulmonary function No improvement >2 exacerbations or ARI prior to entry Exhaled nitric oxide No improvement Smoking BHR Improved History of smoking, ≥10 pack-years Rescue medication use No improvement Lung comorbidities AQL No improvement Hahn (2012), current study None Overall asthma symptoms Randomized: no improvements in any outcome AQL Open label: improved overall asthma symptoms and AQL score at end of prescription that persisted after prescription (improvements maximal at the 9-month study point) ACQ ↵* Other than for safety and logistics.
ACQ, asthma control questionnaire; ARI, acute respiratory illness; AQL, asthma quality of life; BHR, bronchial hyperresponsiveness; Cpn, Chlamydia pneumoniae; ECP, eosinophil cationic protein; FEV1, forced expiratory volume in 1 second; ICS, inhaled corticosteroid; Ig, immunoglobulin; IL, interleukin; LRTi, lower respiratory tract illness; Mpn, Mycoplasma pneumoniae; NNT, number needed to treat; PCR, polymerase chain reaction; PEF, peak expiratory flow.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Management of severe asthma: summary of the European Respiratory Society/American Thoracic Society task force report
- British Thoracic Society guideline for the use of long-term macrolides in adults with respiratory disease
- Azithromycin as an add-on treatment for persistent uncontrolled asthma in adults: protocol of a systematic review and meta-analysis
- Management of severe asthma: a European Respiratory Society/American Thoracic Society guideline
- Does maintenance azithromycin reduce asthma exacerbations? An individual participant data meta-analysis
- The differential effects of azithromycin on the airway epithelium in vitro and in vivo
- Meta-Analysis of the Adverse Effects of Long-Term Azithromycin Use in Patients with Chronic Lung Diseases
- Asthma, Chronic Obstructive Pulmonary Disease (COPD), and the Overlap Syndrome
- Development of a Population Pharmacokinetic Model To Describe Azithromycin Whole-Blood and Plasma Concentrations over Time in Healthy Subjects
- Cardiovascular Diseases and Other Evidence for Primary Care Clinical Practice