
Abstract
Adult-onset Still disease (AOSD) is an uncommon clinical entity that predominantly affects young adults. One of the most common presentations of the disease is fever of unknown origin. Early diagnosis can be difficult because fever of unknown origin is more commonly seen with other conditions such as malignancy or infection. Ambiguity in presentation and lack of serologic markers make diagnosis difficult.
We describe here an 18-year-old African-American man who presented with fever, sore throat, and arthritis at initial admission, with serology positive for both Mycoplasma pneumonia and Epstein-Barr infection. The patient was discharged without improvement. He was then readmitted with persistence of initial symptoms and, at that stage, he fulfilled the proposed diagnostic criteria of AOSD. The purpose of this case report is to describe the triggering infections that can initially mislead diagnosis and to review the literature about AOSD from a primary care perspective.
Adult-onset Still disease (AOSD) was first described by Bywaters1 in 1971. Still disease is a systemic inflammatory disorder of unknown etiology. AOSD is uncommon, with an estimated prevalence lower than 1 case per 100, 000 people.2 Patients usually present with a high spiking fever, arthralgia or arthritis, sore throat, transient maculopapular rash, lymphadenopathy, hepatosplenomegaly, and serositis. Patients may or may not have all of the above symptoms at initial presentation.
Case Presentation
An 18-year-old African-American man presented to the emergency department with complaints of having had sore throat, joint pain, and a spiking fever for 5 days. The rest of the review of the systems was negative. He had no significant medical history, was not taking any medication, and had no significant family history. He smoked marijuana approximately 2 to 3 times a week. Vital signs at admission were a temperature of 38.8°C, heart rate of 92 beats per minute, respiratory rate of 20 breaths per minute, and blood pressure of 126/74 mm Hg. Physical examination showed shotty cervical lymphadenopathy bilaterally. Cardiovascular and respiratory systems were normal. The abdominal examination showed mild hepatosplenomegaly and the genitourinary examination was normal. A moderate left knee joint effusion was noted, and tenderness was elicited in the shoulder, knee, elbow and wrist joints. Total white blood cell count, bands, C- reactive protein level, erythrocyte sedimentation rate (ESR), and liver function test were elevated. See Table 1 for further details about the laboratory results of the patient during the initial admission.
Laboratory Values of the Patient during the Course of Treatment
Transthoracic echocardiogram revealed a small pericardial effusion, with no valve vegetation. A chest radiograph showed a left lower lobe consolidation with minimal pleural effusion. Radiographs of the left knee revealed a moderate effusion. Left knee joint fluid study was normal. Urinalysis, urine culture, and 3 sets of blood cultures were negative. Based on the chest radiograph findings and increased white blood cell count, a diagnosis of community-acquired pneumonia was made and the patient was started on ceftriaxone and azithromycin. Mycoplasma and Epstein-Barr virus serologies were obtained and found to be positive. He was discharged from the hospital on a 2-week course of azithromycin and ibuprofen with instructions to return to family medicine outpatient for follow- up.
He was readmitted after 9 days with a persistent fever that did not respond to ibuprofen or azithromycin. Physical examination did not reveal any new findings. He underwent further work-up. The list of laboratory examinations performed during the second admission are shown in Table 1. An infectious disease consultation was obtained. A septic work-up was repeated and was negative. A progress chest radiograph showed resolution of the pneumonia and pleural effusion. A repeat transesophageal echocardiogram ruled out infective endocarditis. At this stage an autoimmune disorder was considered. The patient was evaluated by a rheumatologist and was noted to fulfill the proposed diagnostic criteria of AOSD (refer to Table 2). He was discharged from the hospital on naprosyn and instructed to follow up with the rheumatologist as an outpatient.
Yamaguchi Criteria*
Our patient's symptoms did not resolve with naprosyn after discharge from the hospital. He developed a skin rash so he was started on low-dose oral prednisone, which was subsequently increased to 60 mg daily. He continued to have fevers and left wrist swelling despite treatment with the steroid. Magnetic resonance imaging of the left wrist showed synovial proliferation and erosion (Figure 1) so he was started on methotrexate. His symptoms resolved within 2 weeks of starting methotrexate and he is currently taking 15 mg of methotrexate weekly. All of his inflammatory markers have returned to normal (see Table 1).
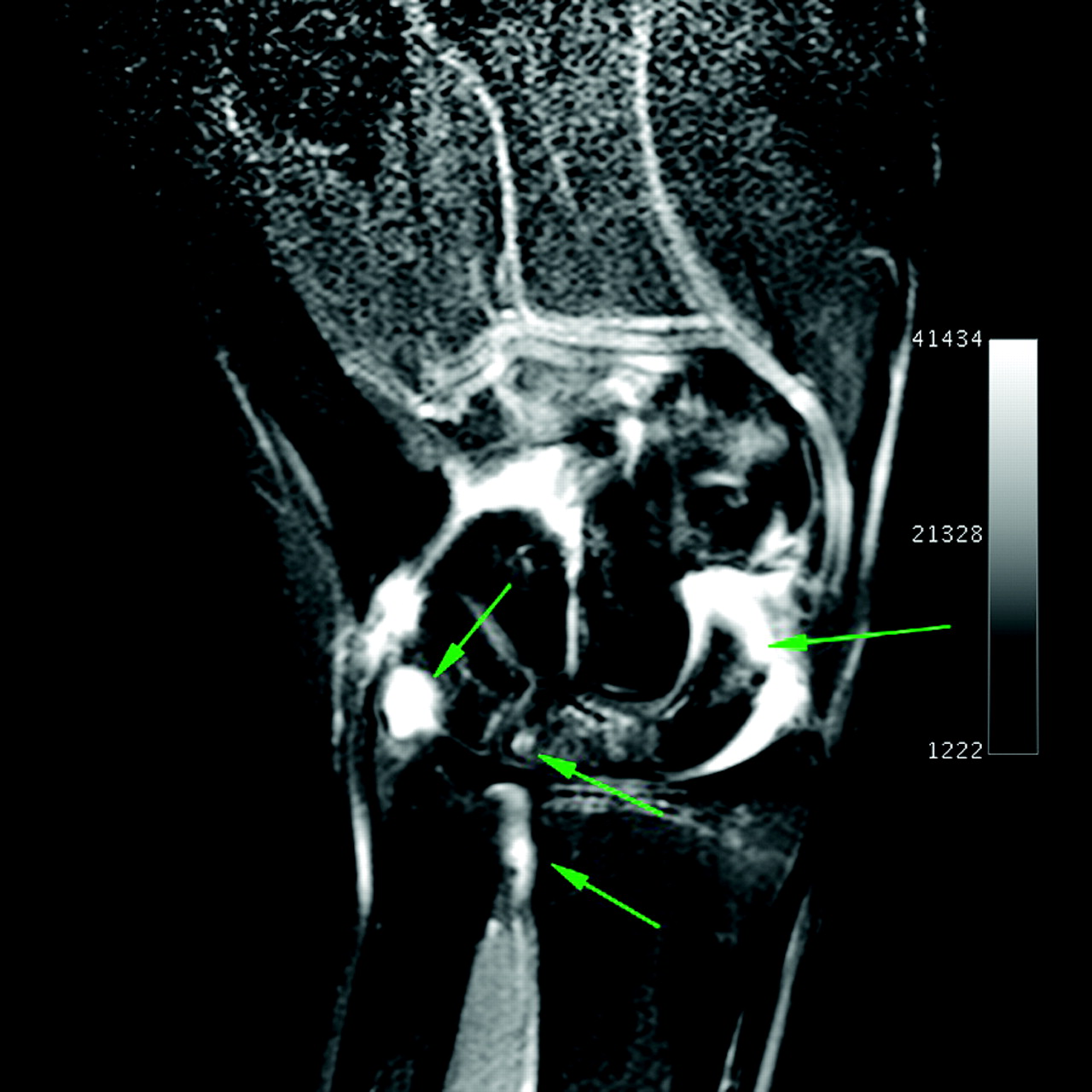
Magnetic resonance image of the left wrist. Gadolinium-enhanced, coronal, T1-weighted image demonstrates synovial proliferation and active synovitis (bright signal between and contiguous to the carpal bones and involving the radioulnar joints), as well as contiguous osseous erosions (arrows).
Discussion
AOSD is a rare inflammatory disorder that usually affects young adults,3,4 although it can also be seen among the geriatric population.5,6 There is a slight preponderance among women.4,7 The mechanisms underlying AOSD are not completely understood to date, and the possibility of a genetic association remains inconclusive.8
There are several infectious agents related to AOSD onset reported in the literature and based on concurrent elevation of serology markers. These include Epstein–Barr; parvovirus B19; cytomegalovirus; human herpes virus 6; human immunodeficiency virus; coxsackie virus; mumps; rubella; echovirus; Hepatitis A, B, and C viruses; campylobacter jejuni; chlamydia pneumonia; and Mycoplasma pneumonia. Our literature review revealed only one case of adult Still disease associated with Mycoplasma pneumonia.9 The combination of both Epstein-Barr infection and Mycoplasma pneumonia with the presentation of AOSD has not been previously reported. Distinguishing between infection-related AOSD with chronic self-perpetuating inflammation versus long-lasting infection with chronic persistence of the infectious agent can be difficult.8
Clinically, most of the patients with AOSD present with fever, sore throat, arthralgia, arthritis, and/or skin rash, but some patients may also have present with conditions such as lymphadenopathy, hepatosplenomegaly, and/or serositis. The fever, typically higher than 39°C, starts suddenly and could present as FUO alone. Joint pain occurs in two thirds of patients. The arthralgia starts concomitantly with fever, involves any joint, and may migrate at the beginning and become more stable during the course of the disease. The skin rash consists of small discrete, nonpruiritic, salmon-pink macules or maculopapules, which are transient and mainly visible during fever.
AOSD is a diagnosis of exclusion. Differential diagnoses are infections, such as endocarditis and deep-seated occult infections, or neoplastic etiology, especially lymphomas and autoimmune diseases like vasculitis and polymyositis. These conditions should be excluded before AOSD is diagnosed.8
Eight different sets of diagnostic criteria have been proposed for clinical diagnosis of AOSD3,10–16 The most widely used and validated criteria are those of Yamaguchi (refer to Table 2).10 The Yamaguchi criteria have a sensitivity of 96.2% and specificity of 92.1%. A study by Crispin et al3 showed that the Yamaguchi criteria had a positive predictive value of 70.3% and negative predictive value of 95.2% among their study population. The laboratory investigations can show an increased systemic inflammatory response, such as high white blood cell count (usually 10,000 to 15,000 with more than 80% granulocytes); thrombocytosis; anemia; ESR; elevated C-reactive protein, and significant increase in serum ferritin level. ESR level could be >100 mm in some cases. Coagulation abnormalities, abnormal liver function tests, and raised lactic dehydroginase level are also seen. A high level of ferritin seems to be characteristic of AOSD and is seen in nearly 70% of cases.7,17 Ferritin levels in AOSD are usually higher than those found in other autoimmune or inflammatory disorders. Serum ferritin levels of >3000 ng/mL have been most commonly observed among patients with AOSD; glycosylated ferritin level drops to ≤20% in patients with AOSD.17
Natural history of AOSD has been described commonly in 3 different patterns.8 Monocyclic, or self-limited, systemic pattern is usually associated with a single flare and complete remission is achieved within 2 to 4 weeks in 19% to 44% of cases. Intermittent, or polcyclic, pattern is seen in 10% to 41% of cases and it usually presents with recurrence of systemic or articular flares separated by periods of remission lasting from 2 weeks to 2 years. The chronic evolution form more frequently is articular than systemic and is seen in 35% to 67% of cases.
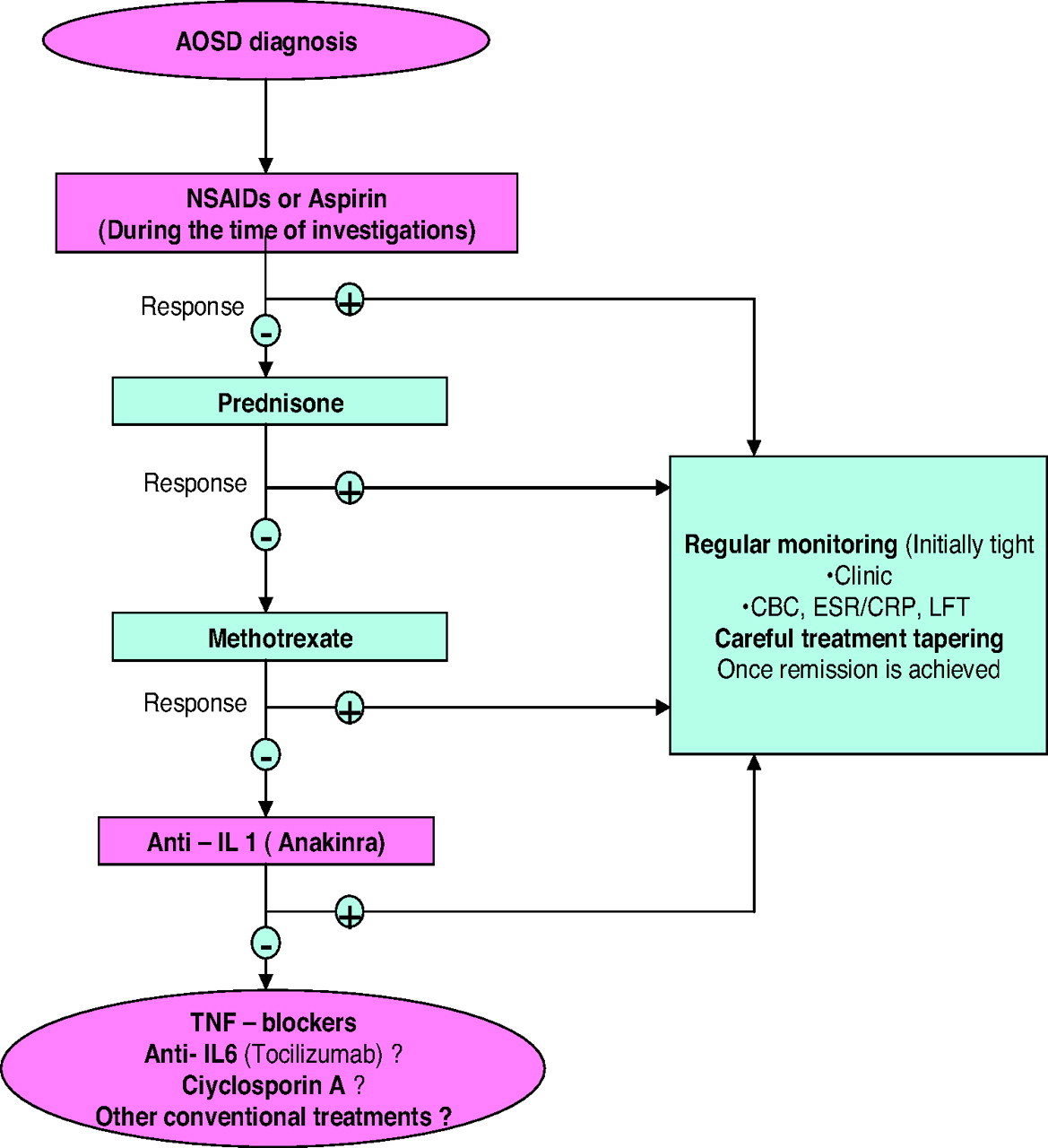
The treatment of AOSD is mainly centered on the use of nonsteroidal anti-inflammatory drugs, steroids, and disease-modifying antirheumatic drugs.1 No randomized, controlled trial has been performed to evaluate treatments for AOSD; nonsteroidal anti-inflammatory drugs and prednisone are used as first-line agents in the treatment of AOSD. After the diagnosis is established, corticosteroids are usually required for symptom control and response is often dramatic. Patients with visceral involvement may achieve a response with an intravenous infusion of high-dose methylprednisolone.5,18 Methotrexate is effective in controlling disease activity and allows for steroid dose sparing in AOSD.19 The potential efficacy of interleukin-I receptor antagonist (anakinra), tumor necrosis factor blockers, immunoglobulins, and cyclosporine has been reported. A treatment algorithm is presented in Figure 2.8

Proposed therapeutic strategies in adult-onset Still disease (AOSD). NSAIDs, nonsteroidal anti-inflammatory drugs; IL, interleukin; CBC, complete blood count; ESR/CRP, erythrocyte sedimentation rate/C-reactive protein; LFT, liver function tests; TNF, tumor necrosis factor.
Conclusion
AOSD is a rare autoimmune disorder. The most characteristic clinical presentation of this condition is fever, arthralgia or arthritis, sore throat, and skin rash. Fever of unknown origin is one of the most common presentations of AOSD. Diagnosis is based on exclusion of inflammatory and neoplastic diseases and no definite serologic marker is available at present. It is still controversial as to whether the infections found in conjunction with AOSD are merely “contemporaneous” or if they may indeed be triggering factors of AOSD.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication June 23, 2009.
- Revision received October 26, 2009.
- Accepted for publication November 2, 2009.




{kind=link}
{kind=link}