
Abstract
Introduction: Current guidelines for the diagnosis and management of asthma suggest that patients perform peak expiratory flow (PEF) measurements while standing; however, recent literature suggests this may not be necessary. The purpose of this study was to determine the impact of patient position on PEF measurements.
Methods: A randomized observational analysis of PEF measurements for 211 patients in sitting and standing positions was performed. The highest PEF measurement from tests performed with correct technique in both the sitting and standing position was compared.
Results: Overall, PEF measurements did not significantly differ between the sitting and standing positions (506 ± 2 L/min versus 508 ± 2 L/min; P = .45). No differences were seen between mean PEF measurements in the sitting or standing positions for either women or men, nor were there significant differences between mean PEF values for the sitting and standing positions in participants who reported a history of asthma.
Conclusions: PEF measurements do not significantly differ based on sitting or standing measurements among healthy participants. Based on the results of this study it may not be necessary for the patient to stand while performing PEF measurements. Further study among patients with asthma is warranted.
Asthma is a chronic inflammatory disease of the airways that affects more than 22 million Americans, including almost 7 million children.1,2 Uncontrolled asthma can cause significant burden to patients, including decreased quality of life, lost days of school or work, hospitalizations, and death. When patients are diagnosed with asthma, it is important to educate them about proper asthma management, including, but not limited to, medication use and adverse effects, inhalation technique, and signs and symptoms of asthma exacerbations.
Appropriate asthma management relies heavily on the patient's ability to regularly self-monitor asthma symptoms. Even well-controlled patients need to be monitored over time to reassess asthma severity and adjust medications as needed. Self-monitoring involves not only the assessment of the frequency and severity of symptoms but also the measurement of pulmonary function, which is often done by measuring the peak expiratory flow (PEF). Daily PEF monitoring can be helpful to detect changes in disease states that require treatment, evaluate response to changes in therapy, and can provide a quantitative measurement of impairment.3 The current National Asthma Education and Prevention Program Expert Panel Report 3 guidelines suggest that, in addition to symptomatic monitoring in asthmatic patients, pulmonary function should also be assessed periodically.3 The Expert Panel suggested that long-term, daily PEF monitoring should be considered for patients who have moderate or severe persistent asthma, who have a history of severe exacerbations, who poorly perceive airflow obstruction and worsening asthma, and for those patients who prefer that method of monitoring.3 Monitoring PEF can assist in determining the severity of the patient's asthma and can guide therapeutic decisions in the home, the school, the clinician's office, or the emergency department.
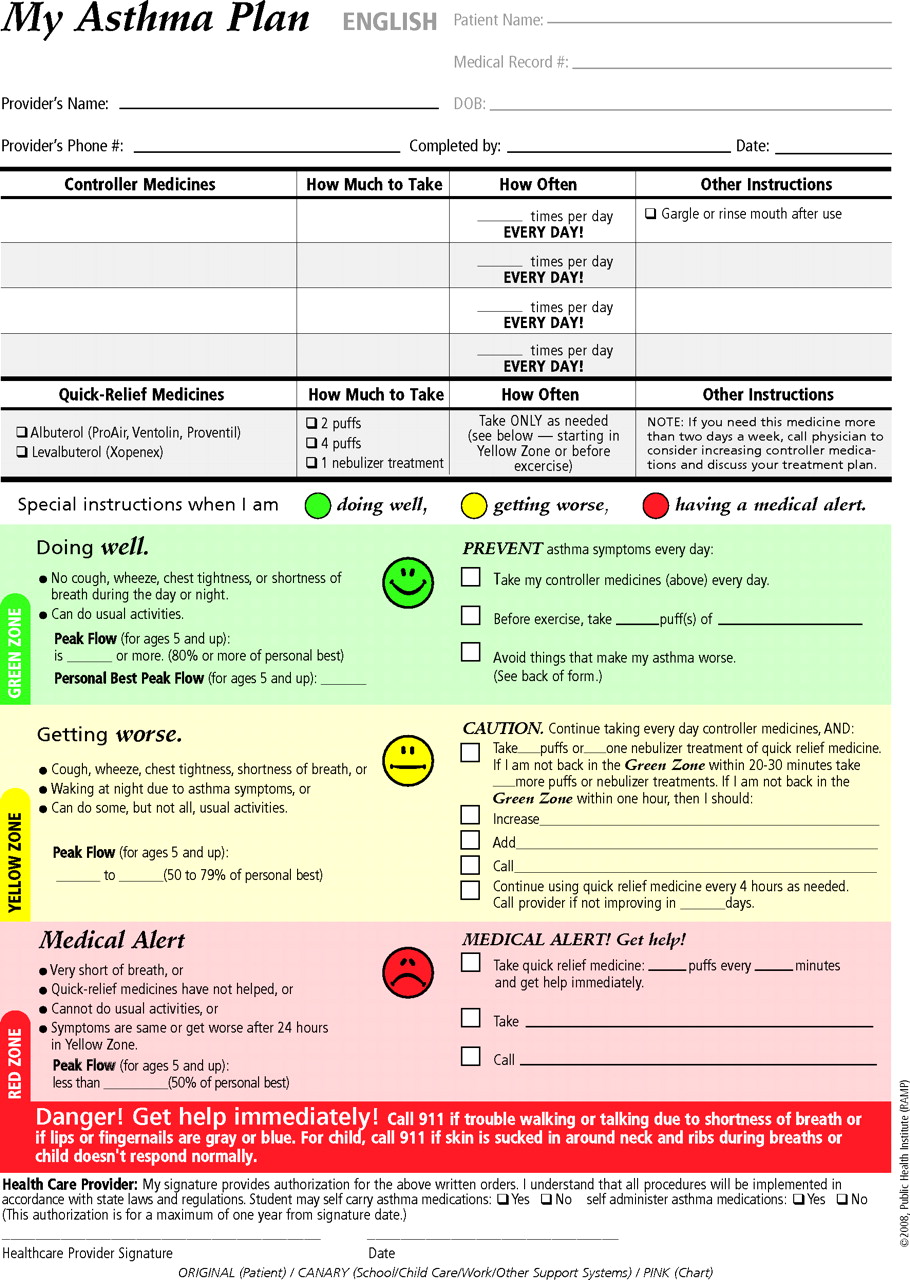
PEF measurements are also useful in the development of a written Asthma Action Plan, which should be given to every patient with asthma. The Asthma Action Plan should include instructions for both daily management and management of exacerbations (Figure 1). It is important to note that the 3 zones in the Asthma Action Plan are determined by the patient's personal best PEF measurement.
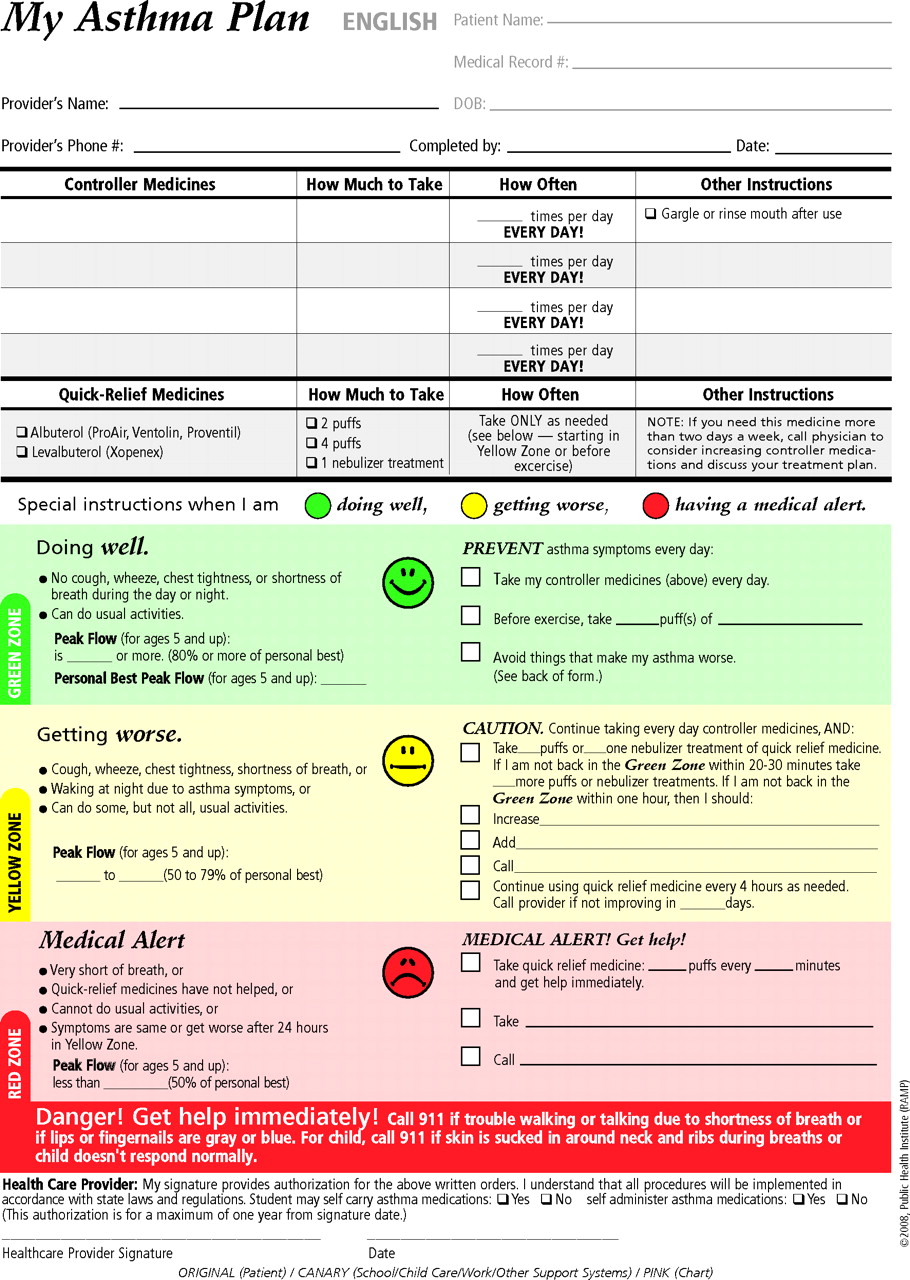
Sample Asthma Action Plan. (Reprinted with permission from Regional Asthma Management and Prevention [RAMP], a program of the Public Health Institute. The RAMP Asthma Action Plan was supported by Cooperative Agreement Number 1U58DP001016-01 from the Centers for Disease Control and Prevention. The contents of the RAMP Asthma Action Plan are solely the responsibility of the authors and do not necessarily represent the official views of the CDC.4)
Current guidelines suggest that patients be standing as they use their peak flow meter; however, patients may be unable to stand for numerous reasons. Therefore, the purpose of this study is to evaluate what, if any, differences exist between PEF measurements taken in the standing and sitting positions.
Methods
Study Design and Participants
This was a prospective, randomized study in which participants were recruited from the University of Tennessee Health Science Center in Memphis, Tennessee. The study was approved by the Institutional Review Board of the University of Tennessee.
Men and women of all ethnic groups who were at least 18 years of age and were enrolled in the Basic Clinical and Communication Skills course at the University of Tennessee College of Pharmacy were eligible to participate in this study. The participants had received a lecture and demonstrations regarding correct and incorrect PEF technique before enrolling in the study. Participants who reported a history of asthma and smokers were also included. Participants were excluded if they were not enrolled in the Basic Clinical and Communication Skills course or were younger than 18 years of age.
Procedures
Data collected included age, gender, height, the presence or absence of obstructive airway disease or other pulmonary diseases, current smoking status, and any medications that may affect pulmonary function. If the participant was taking medications that could affect pulmonary function, he or she was asked to list the name of the medication, dose, and the time of the last dose taken. To ensure privacy of each individual, the data collection forms were assigned a study number rather than a personal identifier.
Participants were randomized to perform the PEF maneuver in either the sitting or standing position first; however, they performed the PEF maneuver in both positions. Participants were divided into groups of 8 to 12 and an investigator was assigned to each group. Using a TruZone® peak flow meter (Monaghan Medical Corp., Plattsburg, NY), the respective investigator demonstrated the proper use of the peak flow meter in the standing position (as directed in the current National Asthma Education and Prevention Program guidelines; Figure 2).3 For the sitting position, participants were instructed to sit with their backs straight in a chair with knees bent and feet flat on the floor rather than standing with legs shoulder width apart. Participants were then allowed to practice using the peak flow meters until they were comfortable with the technique. Once the participants received adequate instruction and time to practice, investigators directly observed each participant perform 3 PEF measurements in either the sitting or standing position first, as was dictated by the data collection form. Investigators also observed whether the measurement was conducted with proper technique. The participant was allowed to rest briefly and then he or she performed 3 more measurements in the alternate position. Therefore, each subject performed 6 PEF measurements. All measurements were recorded. Consistent with recommended procedures in patient care, only the highest measurements for both the sitting and standing positions were analyzed.
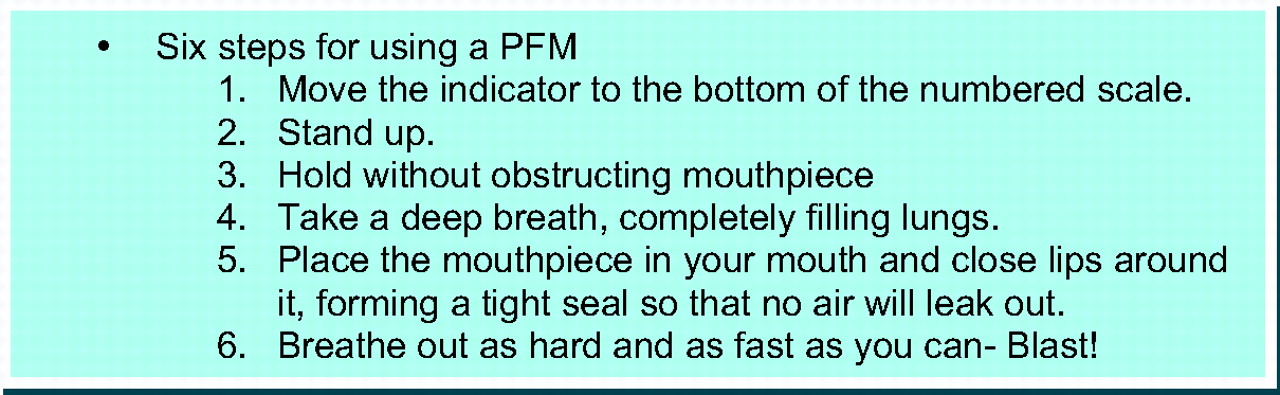
Directions for peak flow meter use. (Adapted from National Heart, Blood, and Lung Institute Expert Panel. Report 3: guidelines for the diagnosis and management of asthma. Bethesda, MD: National Institutes of Health; 2007.3)
Statistical Analysis
For demographic variables, means, standard deviations, and frequencies were computed. The primary variable of interest was PEF (L/min) obtained in the sitting and standing positions. These results were analyzed using the repeated measures analysis of variance, with subject included as a random (block) variable and position as a fixed effect. Additional analyses were conducted using a nested factorial design with the following effects in the model: sex (fixed effect), subject nested within sex (random), position (fixed effect), and the interaction of sex and position (fixed effect). All contrasts were preplanned and made with α = 0.05. SAS software for Windows (SAS Institute, Cary, NC) was used for all statistical analysis.
Results
A total of 211 healthy men and women, ranging from 20 to 43 years of age, completed the study (Table 1). Twenty-nine (13.7%) participants reported a history of asthma. Of those who had a history of asthma, 19 reported currently using medications to treat asthma symptoms. Ten particiapants (4.7%) reported smoking, with 4 of these being current smokers and 6 being previous smokers who had quit at least 3 months before the study began.
Demographics
Overall, the means for PEF were not significantly different when obtained from the sitting position versus the standing position (506 ± 2 L/min vs 508 ± 2 L/min; P = .45). No differences were seen between mean PEF measurements from the sitting and standing positions among either women or men (Table 2). There was also no significant difference between mean PEF values for the sitting and standing positions among participants who reported a history of asthma or in those who reported a history of smoking (Table 2). Consistent with predicted values, there were significant differences detected when comparing the PEF measurements of men to those of women in both sitting and standing positions (P < .0001).
Peak Expiratory Flow Measurements (L/min)*
Discussion
In this study we assessed the impact of body position on PEF measurements in both the sitting and standing positions. Overall there was no significant difference in mean PEF seen in the standing versus sitting positions, nor were there significant differences seen in subgroup analysis. Although the asthmatic population did have higher average PEF measurements than women, this is most likely because the asthma subgroup included both men and women.
The current National Asthma Education and Prevention Program guidelines include patient instructions for using a peak flow meter that require patients to stand while using the peak flow meter.3 However, spirometry testing, which is used in the initial diagnosis of asthma and other pulmonary diseases, may be performed either sitting or standing, but the position must be recorded.5,6
The literature examining the impact of patient position on PEF measurements is limited. Vaswani and colleagues7 evaluated peak flow measurements in both the standing and sitting positions for 33 healthy men and women aged 18 to 58 years. Patients were excluded if they had asthma or any other respiratory problems, if they were taking any medication (particularly bronchodilators), and if they smoked.7 The authors found no significant differences between the standing and sitting peak flow measurements, nor were any differences seen when the patients used a nose clip.7
A similar study performed in Japan by Nagasaka et al8 included a total of 74 patients, 32 of which reported a history of asthma. The authors found no differences between standing and sitting peak flow measurements and that peak expiratory flow did not differ when a nose clip was used in either the healthy population or the patients who reported a history of asthma.8 However, healthy patients did have higher average PEF measurements than did those with asthma.8 A third study examined the impact of gestational age and maternal position in sitting, standing, and supine positions on the rate of decline of PEF measurements. This study included 38 healthy, pregnant women with a mean age of 31.2 years. The authors found that, although gestational age had a significant impact on PEF measurements, no significant differences were seen between the measurements taken in the sitting and standing positions.9
Each of these studies was conducted with a small number of relatively healthy patients; this can limit the applicability of these studies to larger, asthmatic populations. In contrast, our current study was conducted among a larger population. However, there are some limitations to this study. Our participants were mainly young, healthy students at the health science center but we recognize the need for further study among patients with asthma who have a range of ages. There were also a small number of asthmatics included, but not every participant who reported a history of asthma was taking medications for asthma. Because asthma medications, particularly bronchodilators, can affect PEF, it would be extremely useful to determine the impact of testing PEF results by position among a larger group of asthmatics. Further studies are needed in a strictly asthmatic population to determine what, if any, differences exist in PEF measurements.
Conclusion
Based on the results of this study, it may be unnecessary to stand while performing PEF measurements. Larger studies involving the previously mentioned populations, particularly a larger asthmatic population, are needed to further evaluate the impact of patient position on PEF measurements.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication May 18, 2009.
- Revision received August 21, 2009.
- Accepted for publication August 24, 2009.




{kind=link}
{kind=link}