
Abstract
Purpose: The purpose of this study was to evaluate the use of the Fischer cone biopsy excisor (FCBE) as the primary electrode for treatment of cervical dysplasia in a family medicine office.
Methods: Retrospective analysis of cervical electrosurgical excision procedures in patients with cervical intraepithelial neoplasia (CIN) performed in our Family Medicine Center between 2002 and 2005.
Results: We reviewed 91 cases. Indication for excision was ≥CIN II in 86.8% of the patients. In the FCBE group (n = 86), 95% of the specimen margins were negative for dysplasia, 90% had no reported thermal artifact, and 81% were submitted unfragmented. In the FCBE and the loop electrosurgical excision procedure (LEEP) group (n = 5), 4 of the 5 specimens’ margins were negative for dysplasia. Reported complications included palpitations or flushing during cervical block (32%), pain (9%), and heavy bleeding (3%).
Conclusion: In this case series the use of the FCBE with or without the LEEP in a family medicine office provided a high rate of negative margins for dysplasia and a low rate of fragmentation and thermal artifact. Family physicians who perform LEEP can also use the FCBE safely in their offices to treat cervical dysplasia.
- Cervical Intraepithelial Neoplasia
- Fischer Cone Biopsy Excisor
- Loop Electrosurgical Excision Procedure
- Procedures
- Cancer Prevention and Control
- Pap Smears/Colposcopy
- Case Series
Treatment of cervical dysplasia in an outpatient setting involves either electrosurgical excision or cryotherapy of the cervical transformation zone. Two electrosurgical excision methods are most commonly used: the loop electrosurgical excision procedure (LEEP) and the Fischer cone biopsy excisor (FCBE). The LEEP was introduced in 1989,1 followed by the FCBE in 1994.2 Disadvantages of the LEEP include residual dysplasia at the margins of the specimen, thermal artifact, and fragmentation of the specimen.3–6 These factors can increase the risk of recurrence of dysplasia after excision and can negatively affect the ability of the pathologist to evaluate the specimen.7–10
The FCBE was designed to minimize the disadvantages of the LEEP by increasing the support and stabilization of the excising stainless steel wire. The FCBE consists of a straight stainless steel electrode attached to an insulated shaft and stop arm. After activation the electrode is inserted into the cervix until the stop arm touches the cervix. The shaft is rotated 360 degrees and a cone shaped cervical specimen is cut. Seven sizes of the wire are available, with different lengths and widths.2,11
Many articles describe family physicians’ experience with the use of LEEP to treat cervical dysplasia.12–15 However, there is currently no published article that describes the use of the FCBE for this purpose in a family medicine office.
In this study we evaluated the use of the FCBE in a family medicine office for the treatment of cervical dysplasia. To evaluate its effectiveness we documented rates of dysplasia at the tissue margins, fragmentation of the specimen, thermal damage, and procedure complications. In addition, for patients in whom the dysplasia was very large and we visualized residual Lugol negative epithelium after the use of the FCBE, the LEEP was used to remove these areas. We hypothesized that by doing so we will decrease the incidence of residual dysplasia in these cases.
Methods
After obtaining approval from our institutional review board we collected data from cervical excision procedures done for women who presented to the William Beaumont Hospital Family Medicine Residency Colposcopy Clinic from 2002 to 2005. Most patients were referred to our center by the local health department for evaluation and treatment of an abnormal Papanicolaou smear. Indications for electrosurgical excision were (1) biopsy proven CIN II or greater, (2) persistent CIN I, or (3) cytologic/histologic discrepancy in women with Papanicolaou smears showing high-grade squamous intraepithelial lesion.
A single family medicine attending physician performed the procedures or directly supervised family medicine residents who performed the excision. After positioning the patient in the lithotomy position and visualizing the cervix, the physician performed a cervical block by injecting into the cervix 1% lidocaine with 1:100,000 units of epinephrine. Lugol solution, which can be used either before or after the lidocaine injection, was then applied to the cervix to outline the extent of the lesion. After visualization of the entire lesion, the operating physician selected the FCBE size with the objective of the removal of the entire dysplastic epithelium in a single pass. Before the actual excision, the physician practiced the excision of the dysplasia without electricity to determine whether the selected electrode could remove the entire lesion. Under colposcopic guidance, the operator performed conization using a blend setting (cut and coagulation), with wattage determined by the size of the instrument and the manufacturer's recommendations. To achieve hemostasis we used a ball electrode to fulgurate any bleeding areas then applied Monsel solution. In cases where the dysplasia covered a large area of the cervix that we could not remove completely after one pass with the FCBE, we used a loop electrode to remove any residual Lugol negative tissue (Figure 1). Use of the LEEP to remove residual dysplasia after the use of the FCBE is a method used in our center but has not been evaluated.

Combining the use of the Fischer cone biopsy excisor (FCBE) and loop electrosurgical excision procedure for certain lesions. A: The cervix after application of Lugol solution. B: Conization with the FCBE. C: The cervix after conization with the FCBE. D: Use of the loop electrode to remove residual Lugol negative epithelium.
A single family medicine resident measured the sample's width and depth after it was processed for interpretation on the pathology slide. We measured only unfragmented specimens. We summarized categorical variables using frequencies and percentages and compared them in contingency tables using the Fisher exact or χ2 tests wherever appropriate. We further compared the results of the colposcopy and FCBE tests using the agreement statistics of simple and weighted kappa and the Bowker test of symmetry.
Results
We reviewed the results of 91 procedures. The mean age of the women in the study group was 26 years (range, 16–44 years). The mean age when women started having intercourse was 16.5 years, and the mean number of lifetime sexual partners was 7.5. Two thirds of the women reported current use of tobacco. Eleven percent reported a history of chlamydia infection, 1% reported a history of gonorrhea infection, and 10% reported a history of human papillomavirus infection. Thirty-six percent of women in the study were nulliparous.
The indication for conization was ≥CIN II in 86.8% of cases, persistent CIN I in 7.7% of cases, and discordance between a Papanicolaou smear showing a high-grade squamous intraepithelial lesion and colposcopy results in 5.5% of cases. We compared the histologic results from cervical biopsy with histologic results from the cone biopsy (Table 1).
Histology Results from Colposcopy Compared with Fischer Cone Biopsy Excisor (n = 91)
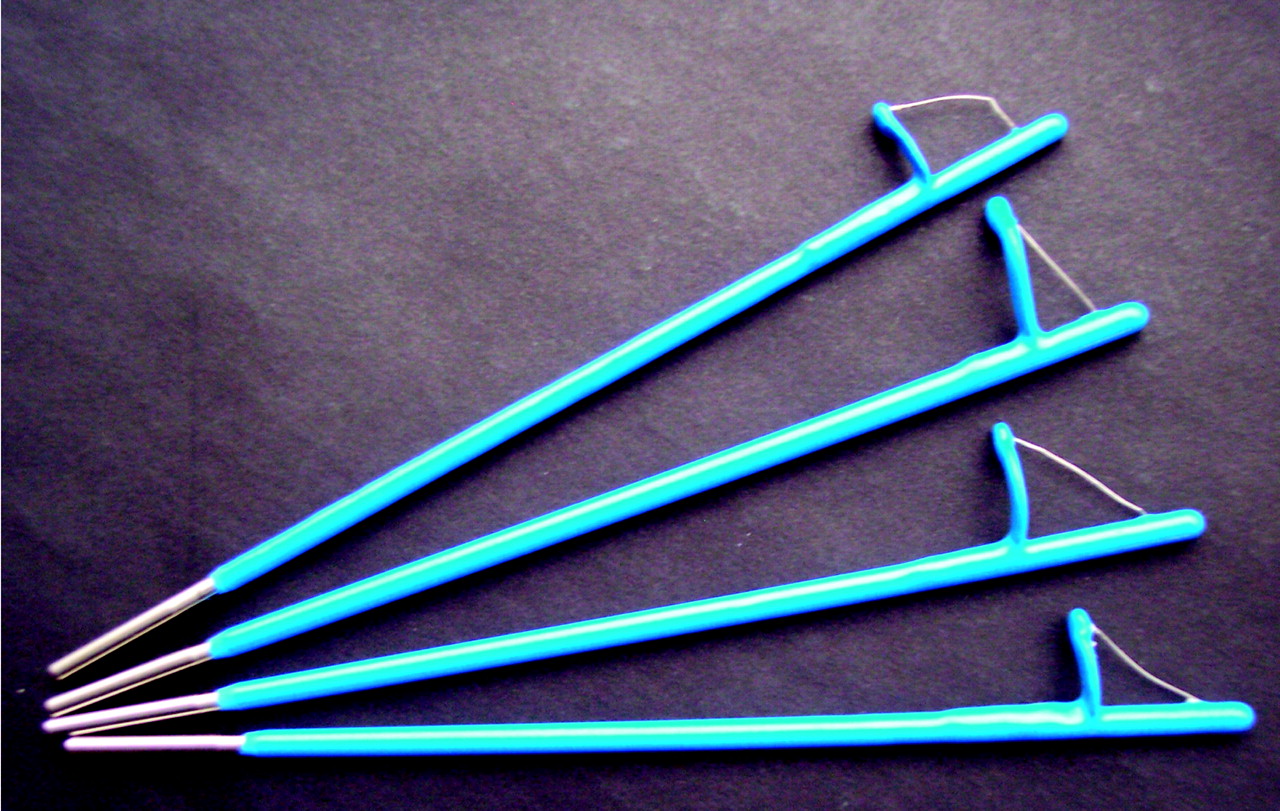
The FCBE is available in 7 sizes; however, we needed to use only 4 sizes during the study (Figure 2). The small FCBE was most frequently used (44%), followed by the large shallow (37%), then the medium (18%); we used the small, wide-angle electrode in only one case.
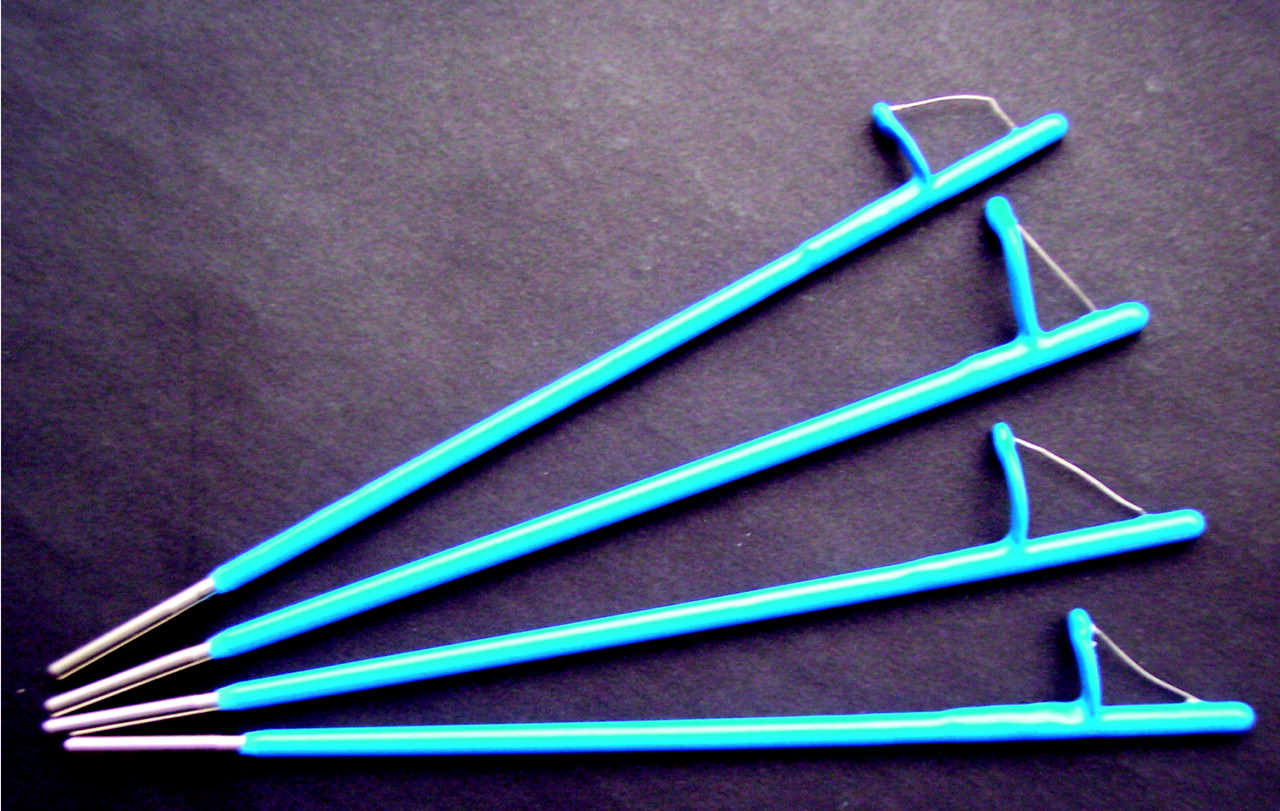
The Fischer cone biopsy excisor electrodes used in our study. (From the bottom: small, medium, large shallow, small wide angle.)
Overall, specimen margins were negative for dysplasia by pathologic examination in 86 of 91 (94.5%) patients. In cases where the operating physician did not visualize any residual Lugol negative epithelium after one pass with the FCBE, negative margins were reported in 82 of 86 (95.3%) patients. All lesions for which the small FCBE was used had negative margins. For the 5 cases in which the operating physician noted Lugol negative epithelium after one pass with the FCBE, we used a loop electrode to remove all Lugol negative tissue. This resulted in negative margins in 4 of the 5 cases. The endocervical curettage was positive in 12 samples during colposcopy, of which only 2 had positive margins after conization.
Most specimens (90%) had no thermal artifact as reported by the pathologist. When the FCBE and loop electrodes were used, 2 of 5 specimens showed thermal artifact, per the pathology report.
Of the specimens in the FCBE group, we submitted 72 of 86 (84%) unfragmented, 10 of 86 (11%) in 2 fragments, and 3 of 86 (3.4%) in 3 fragments. There was no correlation between the size of the FCBE used and the fragmentation of the specimen.
The average (± SD) specimen width and depth was 13.7 ± 2.6 mm and 6.5 ± 1.3 mm, respectively. Table 2 shows the mean measurement of the specimen for each of the FCBE sizes used.
Mean Specimen Size (mm) Produced from Each Fischer Cone Biopsy Excisor Electrode
Thirty-nine percent of the women complained of mild symptoms during the cervical block. These symptoms consisted of flushing, palpitations, or lightheadedness. Symptoms resolved spontaneously after holding the injection of the lidocaine. Patients complained of mild pain during the procedure in 9% of the cases. Only 3 (3.2%) cases had an estimated blood loss of more than 25 mL; in these cases we used fulguration and Monsel solution to control the bleeding. Eleven percent of the women returned to the clinic within 4 weeks after the procedure with complaints of bleeding, vaginal discharge, or cramping. Most women followed up with their local health department for continued surveillance; no Papanicolaou smear results were available to report about disease recurrence.
Discussion
Most family physicians who treat cervical dysplasia in the office use the LEEP.12–15 Although the FCBE has been available for many years as a safe and effective method for the treatment of cervical dysplasia, no study has reported on its use by family physicians.
Three previous studies documented advantages with the use of the FCBE compared with the LEEP. Scribner et al,2 Fischer et al,11 and Rosen et al16 all showed that the FCBE, compared with the LEEP, leaves less dysplasia in the specimen margins (8% vs 17%) and provides a specimen that is significantly less fragmented (82% vs 30%) and has less thermal artifact (2.5% vs 24.6%). A more recent study by Boardman et al,17 however, evaluated the same variables and showed no difference between the 2 electrodes. In that study, the FCBE produced higher rates of thermal artifact compared with the 3 previous studies (35% vs 2.5%) and much higher rates of dysplasia at the specimens’ margins (28% vs 8%).
In our case series, which was performed in a family medicine office, we were able to duplicate the favorable results from the 3 earlier FCBE trials that were published in the gynecology literature. Specifically, we were able to achieve low rates of dysplasia at the specimen margins (5.5%) as well as low rates of thermal artifact (10%).
The main limitation of our study is the lack of a LEEP comparison group. Other limitations include lack of follow-up data and the fact that some of the patients included in our study would not need treatment based on today's treatment guidelines because the guidelines for treatment of CIN I and CIN II have changed since our study period.18
The design of the FCBE offers the operator more support than do the LEEP electrodes. This allows the operator to better tailor the excision area, but the FCBE offers only one pass to remove the cervical transformation zone and the dysplastic tissue. One advantage of the FCBE is the ability to use it in cases where the endocervical curettage is positive without the need for the “top hat” excision that is done after LEEP.
In cases where a large area of the cervix is involved with dysplasia, or among patients with cervical ectropion, removing the desired area of the cervix in one pass using the FCBE or the LEEP can be a challenge. In these cases we used the Loop electrode after the first pass with the FCBE. This 2-step method could help decrease the rate of residual disease in the majority of cases compared with using the FCBE or LEEP alone. No increase in bleeding or pain was noted in these patients. The option to use the 2 electrodes in certain cases uses the advantages offered by both electrodes in an effort to remove the entire dysplastic lesion, although it increases the cost of the procedure. A larger trial is required to confirm the benefit of this 2-step method.
In our experience, one of the concerns reported by physicians regarding the use of the FCBE is the perception that it removes larger cervical specimens than the LEEP. In our study the mean depth (± SD) of the specimens was 6.5 ± 1.3 mm, which compares favorably to the reported depth of the LEEP specimen. This also corresponds to the fact that 7-mm depth is adequate to remove 99% of dysplastic lesions.19–20
The use of the FCBE in our family medicine office provided similar results to what is reported in the gynecology literature. Patients tolerated this procedure well with a low rate of complications. Family physicians who use the loop electrode as the primary electrode for office treatment of cervical dysplasia can consider using the FCBE for certain patients after understanding the advantages and disadvantages of each electrode.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
See Related Commentary on Page 151.
- Received for publication January 5, 2009.
- Revision received May 5, 2009.
- Accepted for publication May 12, 2009.




{kind=link}
{kind=link}