
Abstract
Background: The frequency of recurrent aphthous stomatitis (RAS), the most common oral mucosa lesions seen in primary care, is up to 25% in the general population. However, there has been no optimal therapeutic approach. Our objective was to confirm our previous clinical observation of the beneficial treatment of RAS with vitamin B12.
Methods: A randomized, double-blind, placebo-controlled trial was done using primary care patients. A sublingual a dose of 1000 mcg of vitamin B12 was used in patients in the intervention group for 6 months.
Results: In total, 58 patients suffering from RAS participated in the study: 31 were included in the intervention group and 27 were included in control group. All parameters of RAS among patients in the intervention group were recorded and compared with the control group. The duration of outbreaks, the number of ulcers, and the level of pain were reduced significantly (P < .05) at 5 and 6 months of treatment with vitamin B12, regardless of initial vitamin B12 levels in the blood. During the last month of treatment a significant number of participants in the intervention group reached “no aphthous ulcers status” (74.1% vs 32.0%; P < .01).
Conclusion: Vitamin B12 treatment, which is simple, inexpensive, and low-risk, seems to be effective for patients suffering from RAS, regardless of the serum vitamin B12 level.
Recurrent aphthous stomatitis (RAS) is one of the most common oral mucosa lesions seen in primary care. The Greek term “aphthai” was initially used for disorders of the mouth and is credited to Hippocrates.1 The frequency of aphthous ulcers is up to 25% in the general population, and 3-month recurrence rates are as high as 50%.2 RAS is an idiopathic condition in most patients. The most likely precipitating factors are local trauma and stress. Other associated factors include systemic diseases, nutritional deficiencies, food allergies, genetic predisposition, immune disorders, medications, and human immunodeficiency virus infection. Although RAS may be a marker of an underlying systemic illness, such as celiac disease, or may present as one of the features of Behcet disease, in most cases no other body systems are affected and patients remain otherwise fit and well. Because the etiology is unknown, diagnosis is entirely based on history and clinical criteria; no laboratory procedures exist to confirm the diagnosis.3–6 RAS usually appears as single or clusters of painful ulcers with a surrounding erythematous border. Lesions heal in 1 to 2 weeks but may recur monthly or several times a year.
A comprehensive Medline search, starting at the year 1951, found 578 articles related to the treatment of RAS, including 110 clinical trials. Medical preparations from herbs and multivitamins,7,8 adhesive pastes,9 local antiseptics,10 local and systemic antibiotics,11,12 topical nonsteroidal anti-inflammatory drugs,13 topical corticosteroids,14 and even topical and systemic immunomodulators, immunosuppressants, and corticosteroids15–18 were among the treatments given to patients with RAS. Most of these achieve “short-term” therapeutic goals, such as the alleviation of pain, a reduction in the number of ulcers and their size and duration.9–14 Very few treatments have achieved “long-term” therapeutic goals, such as reduction of the frequency of RAS and maintenance of remission.7,13,15–17 As we previously reported, according to our own 6-year clinical observations,19,20 treatment of RAS with vitamin B12 was successful in a group of patients, who achieved “long-term” therapeutic goals. We conducted a randomized, double-blind, placebo-controlled trial to determine if the usefulness of vitamin B12 could be confirmed.
Methods
Patients older than 18 years of age and who had been suffering from RAS for at least 1 year with a frequency of at least 1 outbreak every 2 months were included. We excluded patients who had known systemic diseases concurrent with lesions in the mouth (Behcet disease, rheumatoid arthritis, lupus, and Acquired Immune Deficiency Syndrome); had received treatment with vitamin B12 in any form for the last year; had received other concurrent treatment for apthous ulcers; were pregnant or nursing; had Leber's optic atrophy; suffered from psychosis; or had a known vitamin B12 deficiency.
The research was conducted between March 2006 and December 2007 in Southern Israel (the Negev). From previous clinical observations we knew that patients rarely complain of RAS, except when it influences their daily lives and that the RAS is not considered a reason to pay a visit to the primary physician. We asked 20 family physicians in the personal letter sent by e-mail to identify patients about suffering from RAS and willing to participate in the study.
At the baseline appointment candidates received full written and verbal information about the study and possible side effects of treatment. Those meeting the inclusion and exclusion criteria signed the informed consent form. Participants were asked to estimate the number of years they had suffered from ulcers, as well as the number and average duration of episodes during the past year. A careful medical history relating to comorbidity and medical treatment (including treatment for RAS) was taken, and sociodemographic information was gathered. Each patient also had a blood test to measure their initial vitamin B12 level. The patients received instructions for estimating severity of pain according to the Numerous Rating Scale21 (NRS) and for filling out the “Aphthous Ulcers Diary.”
The patients were divided randomly (by batch numbers generated by a computer program) into 2 groups: an intervention group and a control group. The physicians and the participants were blinded to the group assignment until the study ended. The intervention group received sublingual vitamin B12 tablets (Solgar, Leonia, NJ). Each tablet contained 1000 mcg of vitamin B12, mannitol, stearic acid, magnesium stearat, and natural cherry flavor; the weight of each tablet was 100 mg. The control group received placebo tablets (containing the same ingredients except for the vitamin B12). The 2 types of tablets were the same in shape, size, color, and flavor. The patients received instructions about daily treatment: for 6 months, they were to take one tablet each day before going to sleep.
The patients met the research staff every month during 6-month period. During every meeting the “Aphthous Ulcers Diary” was collected, the patient was asked about side effects, and the number of remaining tablets in the bottle was counted. The patient received the next dose of 30 tablets of either active ingredients or placebo, according to his assignment (control group or intervention group). The measurement for treatment effectiveness was the average duration (days) of an aphthous stomatitis episode, monthly number of aphthous ulcers, and severity of pain according to the NRS.
The sample-size calculations were determined as follows. According to our previous clinical observations, as many as 73% of patients were “aphthous-free” with prolonged vitamin B12 treatment.20 To achieve a statistical power of 80% and a level of significance of 5%, given the assumption of a “no aphthous ulcers status” of 73% among patients in the intervention group and 30% of those in control group, we calculated a sample size of 24 patients in both groups. Estimating a drop-out rate of 20%, we decided to recruit 29 participants for each group.
The Mann-Whitney test was used to compare the different measurement for treatment effectiveness among the patients in the intervention and control groups. The Freidman test was used to compare the 6 months of treatment among the 2 study groups, and χ2 tests were used to analyze statistically significant differences of categorical variables. P ≤ .05 was considered statistically significant.
Results
Eighty-four patients suffering from RAS were referred by their family physicians; 58 of these patients fulfilled the inclusion and exclusion criteria and agreed to participate and were included in the study. The 2 main reasons for any unwillingness to participate was the long study period and disagreeing to the possibility of being included in the control group. Through randomization, 31 patients were assigned to the intervention group and 27 patients were assigned to the control group. Table 1 compares the sociodemographic characteristics of the 2 study groups. No statistically significant differences were found between the groups in terms of gender, age, marital status, country of birth, and the initial level of vitamin B12. No patient had a vitamin B12 level lower than 150 pg/mL in either study group.
Sociodemographic and Basic Clinical Characteristics of Population
The intervention group that received vitamin B12 was divided into 2 subgroups: 6 patients with a initial level of vitamin B12 within the limits of 150 to 250 pg/mL and 25 patients in whom the level was >250 pg/mL. These 2 subgroups were compared using the Mann-Whitney test, a nonparametric variant of the t test for 2 independent samples because the 2 subgroups were small. Results of test concerning each of the parameters (pain, number of ulcers, outbreak frequency, and duration of outbreak) indicated no statistically significant differences between the 2 subgroups. No adverse events were associated with receiving vitamin B12 or the placebo in this study.
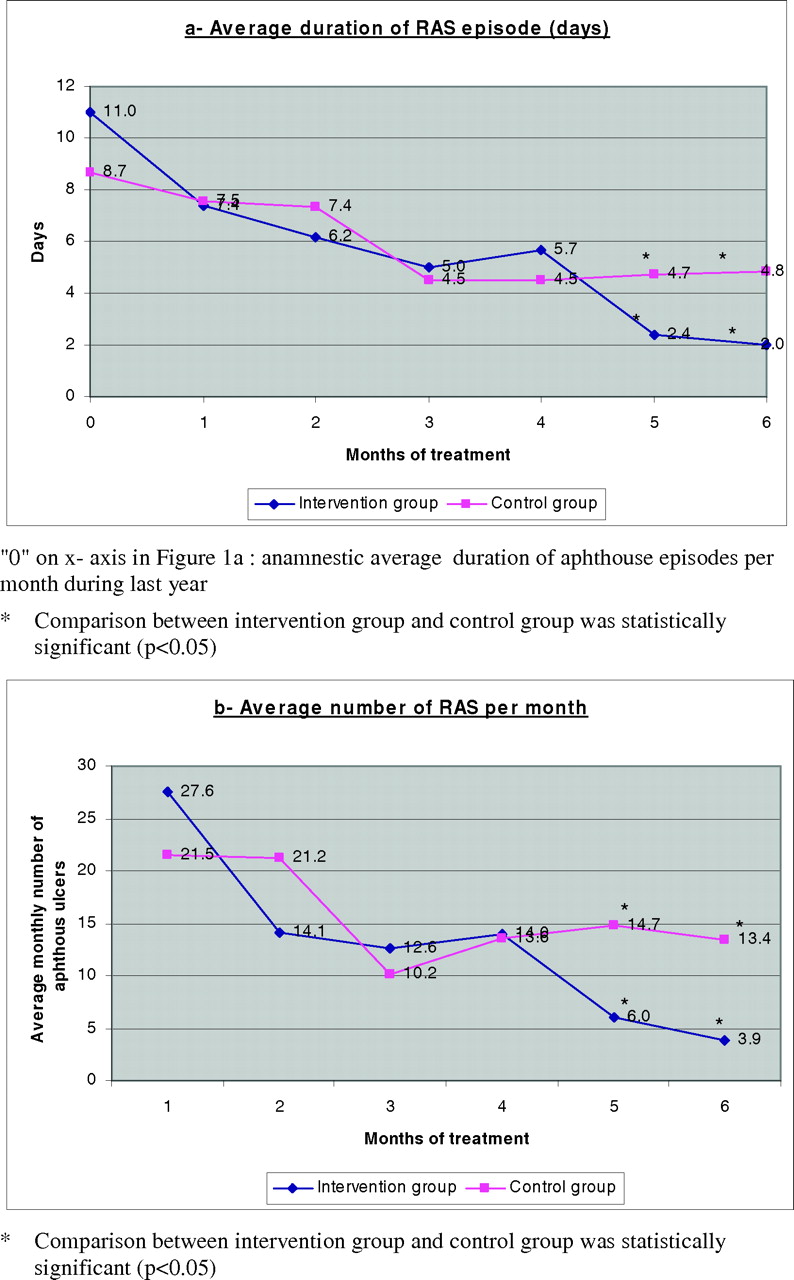
Figure 1A–C shows the comparison between the control and intervention groups in 3 main study measurements for treatment effectiveness. The average duration of RAS episode (number of days) decreased in both groups during the first 4 months of treatment, but the decrease was significantly higher in the intervention group after 5 months and 6 months when compared with control group (2.36 ± 3.65 vs 4.74 ± 4.49; P < .05 and 1.98 ± 3.77 vs 4.84 ± 5.71; P < .05, respectively). The average number of aphthous ulcers per month also decreased during the first 4 months of treatment in both groups. However, in the intervention group it continued to decrease in months 5 and 6 of treatment and became significantly lower than the number of ulcers among patients in the control group (6.00 ± 11.79 vs14.74 ± 17.75; P < .05 and 3.88 ± 7.98 vs 13.39 ± 23.56; P < .05, respectively). The subjective level of pain (according to the NRS) declined throughout the study period, as reported by patients in the intervention group. On the other hand, among those patients in the control group there was a decline in reported pain level only during the first 3 months; pain level increased in the control group during the fourth, fifth, and sixth months of treatment. Statistically significant differences were found in pain level during the fifth and sixth months of treatment between intervention group and control group (1.51 ± 2.54 vs 2.93 ± 2.40; P < .05 and 0.64 ± 1.45 vs 2.36 ± 2.21; P < .01, respectively).

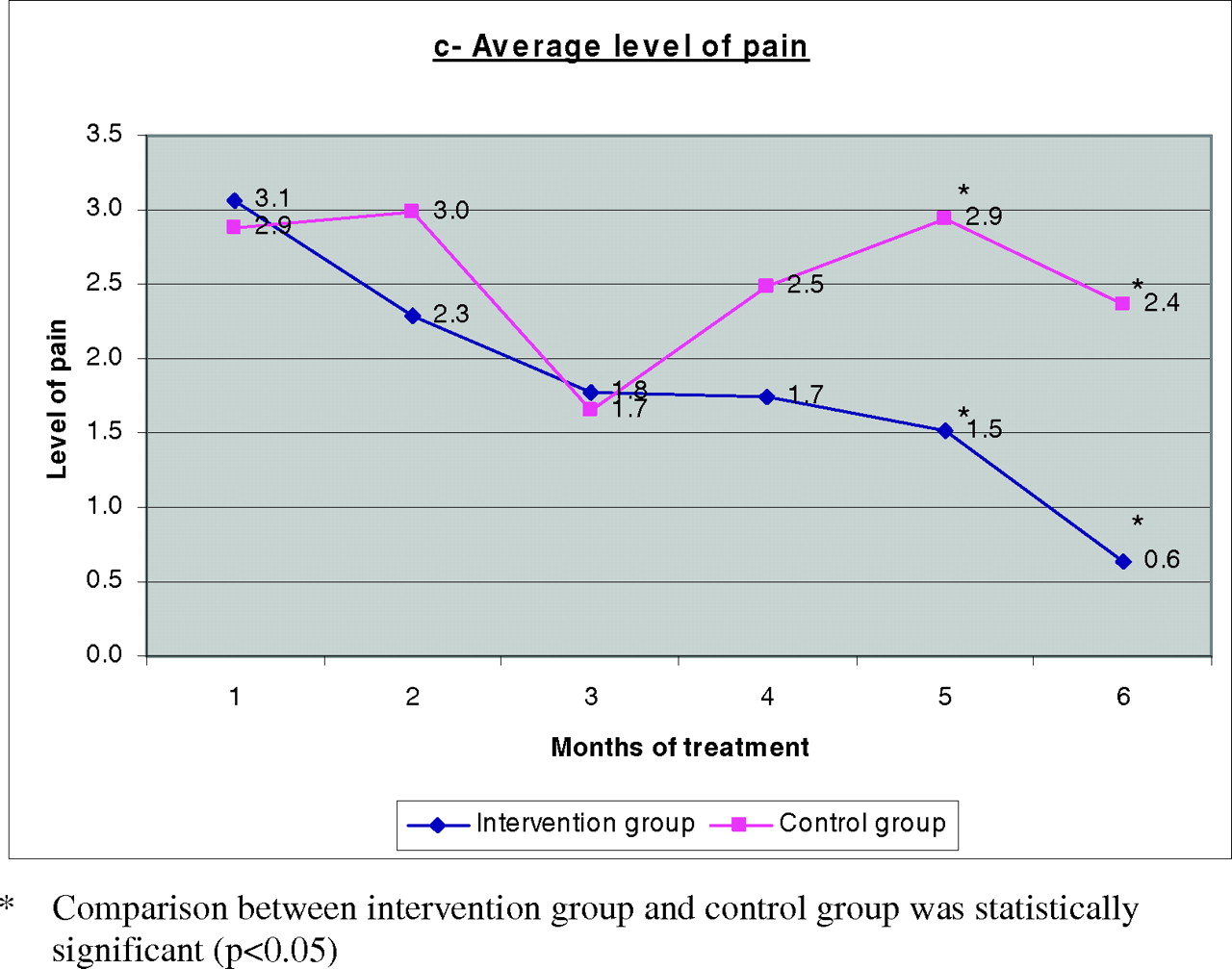
Comparison between control and intervention groups in 3 main study measurements for treatment effectiveness of recurrent aphthous stomatitis (RAS).
Table 2 presents the changes of the 3 main study measurements for treatment effectiveness among each group during the 6-month study using the Freidman test. Among the intervention group there was a statistically significant decrease during 6 months of the study period for all 3 measurements: the average duration of RAS episode in days (χ2 = 30.68, P < .0001); the average level of pain (χ2 = 29.95, P < .0001); and the average number of aphthous ulcers per month (χ2 = 32.97, P < .0001). No statistically significant decrease in these measures was found in patients in the control group. Twenty-seven patients in the intervention group and 25 patients in the control group completed the 6 months of treatment (Table 3). During the last month of treatment, 20 patients (74.1%) from the intervention group and 8 patients (32%) from the control group reached to a “no aphthous ulcers status” (P < .01). When we analyzed the last 2 months of treatment, 15 patients (55.6%) from the intervention group and 4 patients (16%) from the control group had reached to a “no aphthous ulcers status” (P < .01). This tendency was observed already after the fourth month of treatment (29.6% vs 12.0%), but statistical significance had not been reached (P = .11).
Changes of the 3 Main Study Measurements for Treatment Effectiveness During the 6 Months of the Study
Patients Achieving Recovery ("No Aphthous Ulcers Status") By the Time of Examination
Discussion
Results of this double-blind, placebo-controlled study conducted with primary care patients indicate that vitamin B12 treatment was associated with decreases in the level of pain, the number of ulcers, and the duration of outbreaks among patients with RAS. This outcome did not depend on initial level of vitamin B12.
How can we explain this phenomenon? The possibility of “functional” vitamin B12 deficiency was not excluded because we did not check methylmalonic acid (MMA), homocysteine (HCY), or holotranscobalamin II (holoTC). To increase specificity and sensitivity when diagnosing vitamin B12 deficiency, the concept of measuring HCY, MMA, and holoTC (a subfraction of vitamin B12) has aroused great interest. HoloTC, as a biologically active vitamin B12 fraction, promotes uptake of its vitamin B12 by all cells.22 However, diagnostic algorithms using vitamin B12, MMA, and HCY measurements are reflected in studies from some academic centers, and their negative predictive values have not been established. Therefore, the identification and measurement of functional vitamin B12 deficiency remains controversial.23 The recommended “cut off” serum level for vitamin B12 deficiency is 250 pg/mL.24 The probability of “functional” vitamin B12 deficiency decreases when the blood level of vitamin B12 is increased. Because the vitamin B12 level was >250 pg/mL in 80.6% of participants in the intervention group, the probability of “functional” vitamin B12 deficiency was low. Another explanation for the possible effectiveness of vitamin B12 in treating RAS is that vitamin B12 has some unique but still unrecognized functions.25
The response seemed delayed to about 4 months. One possible explanation of delayed response was the low treatment dosage. According to our previous clinical observations, some patients responded more rapidly (after 1 or 2 months) to injections of vitamin B12, which were of a higher dose than the oral treatment.
Although statistical significance was found between the groups, we must interpret the results carefully because of the small sample size. However, this was a prospective double-blind study design and is consistent with our previous clinical observations.20 More than 74.1% of patients in the intervention group were free from aphthous ulcers at the end of the treatment period compared with 32% of patients in the control group.
Vitamin B12 seems to be an effective treatment for patients suffering from RAS regardless of their serum vitamin B12 level. This treatment is simple and inexpensive and has no known significant toxic effects.
Acknowledgments
The authors thank the staff of Siaal Research Center for Family Medicine and Primary Care for assistance with data analysis of the manuscript. The authors thank the pharmaceutical company Solgar, which has supplied our order for sublingual vitamin B12 tablets and placebo.
Notes
This article was externally peer reviewed.
Funding: Solgar pharmaceutical company provided partial funding for this study. Solgar did not take any part in planning this research, its implementation, data analysis, or writing this manuscript.
Conflict of interest: none declared.
- Received for publication May 27, 2008.
- Revision received August 7, 2008.
- Accepted for publication August 20, 2008.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Oxidative Stress and Oral Mucosal Diseases: An Overview
- Multivitamin therapy for recurrent aphthous stomatitis: A randomized, double-masked, placebo-controlled trial
- Re: Effectiveness of Vitamin B12 in Treating Recurrent Aphthous Stomatitis: A Randomized, Double-Blind, Placebo-Controlled Trial
- Optimism: A Good Theme for Family Medicine