
Abstract
Lemierre syndrome is a potentially fatal complication of oropharyngeal infections that is characterized by jugular vein thrombosis and septic emboli. Fusobacterium spp. are the causative organisms. Patients typically present with high fevers, neck pain, and pulmonary symptoms. Prompt clinical diagnosis and treatment with appropriate antibiotics are critical. Anticoagulation for this syndrome is controversial. We present 3 cases within a 12-month period of young, family practice patients seen with oropharyngeal infections who developed Lemierre syndrome. The incidence of Lemierre syndrome may be increasing and primary care physicians should be aware of this rare though serious condition.
“Sore throat” is one of the most common presenting symptoms seen by primary care physicians, accounting for 1% to 10% of office visits.1–3 A recent prospective population-based study estimated the incidence of acute sore throat to be 33% per person-year for children aged 5 to 12 years and 14% per person-year for adults.4 Although the etiology is usually viral and the course self limited, investigations are often undertaken to determine whether the causative organism is group A β hemolytic streptococcus. Physicians should be aware of a rare but potentially lethal complication of oropharyngeal infections: Lemierre syndrome, which is characterized by superinfection with Fusobacterium necrophorum, jugular vein thrombosis, and septic pulmonary emboli. Its incidence has been estimated at 1 per million per year.5
Fusobacterium infections were first recognized in the late 19th century,6 but it was not until 1936, when Andre Lemierre published a case series of 20 patients with Fusobacterium sepsis complicating pharyngitis, that this symptom complex became known as Lemierre syndrome.7 In the preantibiotic era, this syndrome was common and the outcome grim: 18 of Lemierre's original 20 patients died.8 With increasing use of penicillin in the 1960s and 1970s, the condition was only rarely reported and became the “forgotten disease.”6 Thirty-eight cases of Lemierre syndrome were found in the literature between 1974 and 1989,8 and only 14 pediatric cases were reported between 1980 and 1995.9 However, in the last 10 years, already more than 80 cases have been published. This apparent increase may be related to the less frequent prescribing of penicillin for tonsillitis, improved identification techniques of Fusobacterium spp.,5 its growing resistance to erythromycin,10 or increased reporting. We present 3 cases of previously healthy patients seen in a university family practice between April 2006 and April 2007 with an oropharyngeal infection who developed Lemierre syndrome.
Case 1
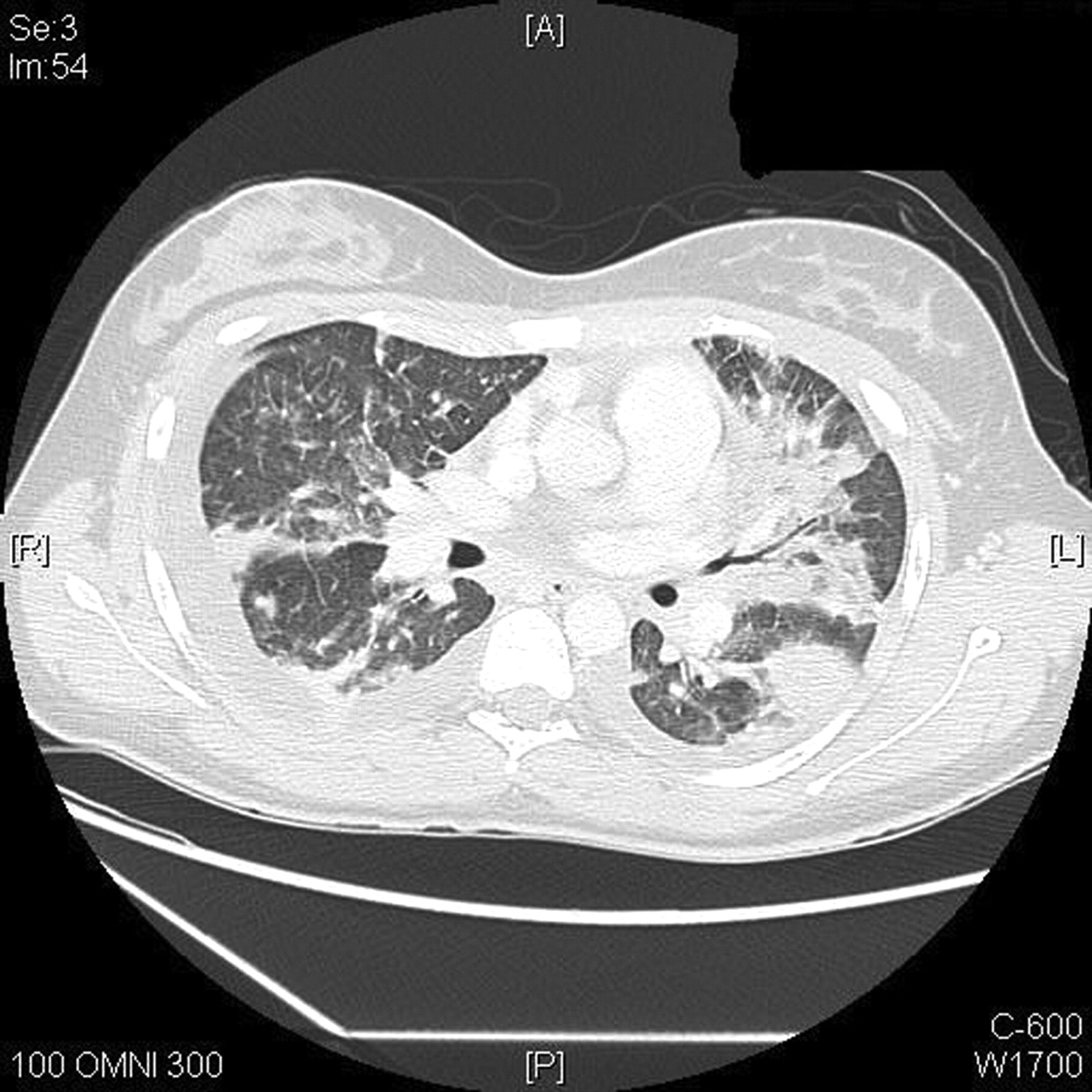
A healthy 19-year-old woman presented with sore throat, low-grade fever, and malaise and was diagnosed with a viral pharyngitis. She developed vomiting and a productive cough, and at a return visit 3 days later had new tender anterior cervical lymphadenopathy and a pulse of 151. Labs at that time showed a white blood cell (WBC) count of 28.4, platelets of 79, blood urea nitrogen (BUN) of 19, and a creatinine of 1.7. She was given empiric ceftriaxone and levofloxacin in the clinic and was sent home but later developed worsening dyspnea and pleuritic chest pain. Examination in the emergency room was notable for marked right-sided neck tenderness and swelling and rales over the right lung field. Chest x-ray (CXR) showed multifocal bilateral infiltrates. Computed tomography (CT) scan showed thrombosis of the right external jugular vein and retropharyngeal phlegmon (see Figure 1) along with multiple pulmonary opacities with central necrosis suggestive of septic emboli (see Figure 2).

Computed tomography scan of the neck with contrast shows complete thrombosis of the right external jugular vein with lymphadenopathy and fat-stranding of the surrounding soft tissues. Retropharyngeal phlegmon is noted (measuring bars).

Computed tomography scan of the chest shows pleural thickening with multiple cavitating lesions (most-notably bottom right) and moderate pleural effusion.
The patient was started on piperacillin-tazobactam and metronidazole. Anticoagulation was held due to thrombocytopenia, international normalized ratio of 1.7, and lack of thrombus extension. She required bilateral thoracostomy tubes for exudative pleural effusions. Blood cultures grew anaerobic Gram-negative rods, ultimately speciated as Fusobacterium necrophorum after 2 weeks, and she was discharged on hospital day 16 with intravenous piperacillin-tazobactam for a total of 6 weeks. CXR 1 week later showed improvement of effusions, and CT scan of the neck 1 month after discharge documented resolution of external jugular thrombus with sclerosis.
Case 2
A previously healthy 14-year-old male initially presented to clinic with a 4-day history of sore throat, 3 days of fever and vomiting, and 1 day of chest and back pain. On examination, he appeared ill with shaking chills, a pulse of 109, blood pressure of 77/42, and a temperature of 38.6°C. He had swollen, erythematous tonsils and a tender cervical lymph node. A complete blood count revealed a normal WBC count with a predominance of neutrophils. Monospot, rapid strep screen, and throat cultures were negative. CXR was normal. Chemistries were significant for a BUN of 24 and a creatinine of 1.7. Blood cultures were obtained, the patient was treated with intravenous hydration in clinic, and he was sent home. The following day, he was symptomatically unchanged and his SpO2 was noted to be 91% on room air. Blood cultures were growing Gram-negative rods. The patient was admitted to the pediatric hospital where a CT scan revealed left internal jugular vein thrombosis and multiple pulmonary nodules concerning for septic emboli. The Gram-negative rods were identified as Fusobacterium species, and he was diagnosed with Lemierre syndrome.
At admission, he was anticoagulated with heparin, which was changed to enoxaparin on hospital day 5. He was started on intravenous meropenem for 9 days and then switched to intravenous clindamycin for a day. The patient remained febrile for 17 days. He was discharged from the hospital in stable condition on hospital day 19 with oral clindamycin to complete a 6-week course and subcutaneous enoxaparin for a total of 3 months. He recovered fully, although repeat ultrasound 10 months after admission still showed occlusion of the left internal jugular vein with the formation of some collaterals.
Case 3
A 28-year-old man presented to the emergency room with 5 days of fever, chills, vomiting, and subjective throat swelling. On the day before admission, he noted a productive cough, pleuritic chest pain, pain in his left arm, and decreased urine output. He had a history of ulcerative colitis in remission and was otherwise healthy. On examination, he was slightly tachycardic but normotensive. He had scleral icterus and an unremarkable oropharynx. Inspiratory crackles were heard at the right lung base. His abdomen was tender with involuntary guarding. Initial labs showed a BUN of 142, creatinine 7.4, WBC count of 27, and platelets of 17. A CT scan of the chest showed multiple bilateral nodular air space opacities.
On hospital day 2, he developed hypotension, acute respiratory distress syndrome, and worsening renal failure. He was transferred to the intensive care unit, intubated, and started on imipenem and vancomycin as well as vasopressors. Blood cultures grew Fusobacterium spp. on hospital day 9 and antibiotics were narrowed to clindamycin. An upper extremity duplex showed thrombosis of the right internal jugular vein and systemic anticoagulation was started. The patient required a pigtail catheter to drain a right-sided pleural effusion. After transfer out of the intensive care unit on hospital day 20, the patient developed electroencephalography confirmed left frontal lobe partial seizures attributed to septic emboli and was loaded on phenytoin. He was discharged on hospital day 26 to complete a 6-week course of clindamycin and 6 months of anticoagulation. In clinic, his antiepileptic medication was weaned and his anticoagulation managed until he was lost to follow-up 4 months after discharge. At the time of this writing, he is healthy and seizure-free.
Discussion
F. necrophorum exists in normal oral flora. Oropharyngeal mucosal damage from another pathologic organism can facilitate its extension into the parapharyngeal spaces.10 Several of the organism's virulence factors are implicated, including hemolysin, hemagglutinin, lipase, leukocidin, and lipopolysaccharide.6 Septic thrombophlebitis of the jugular vein develops with local invasion, either from the tonsillar veins or via lymphatic channels.11 From here, the bacteria can spread hematologically via septic emboli, most commonly to the lungs. Microabscesses in the joints, central nervous system, liver, and kidneys have also been described.6,8,12
Patients most often present with high fever and rigors within 1 week of onset of a sore throat.13 Other symptoms include neck pain, swelling along the sternocleidomastoid, and dysphagia, which result from thrombophlebitis, but can also signal a local abscess. Septic emboli to the lungs occur in 79% to 100% of cases and manifest with cough, dyspnea, pleuritic chest pain, and hemoptysis.10 Arthralgias can occur in 11% to 27% of cases.12 Jaundice is reported in 11% to 49% of cases and abnormal liver function is seen in up to half of patients.10 Coagulopathies can be seen, but are rarely clinically significant.14 Our patients presented typically with sore throat, fever, and respiratory complaints. Two had neck swelling. Curiously, all had vomiting, which is not commonly reported. Hypovolemia, along with bacteremia, may have contributed to the acute renal insufficiency seen in all 3 cases. All appeared significantly ill.
The diagnosis of Lemierre syndrome is primarily clinical and should be entertained early when respiratory symptoms, significant neck swelling, or signs of toxicity occur in the week after an oropharyngeal infection. Common laboratory abnormalities include leukocytosis, thrombocytopenia, abnormal liver function, and elevated C-reactive protein.6 Two of our 3 cases had a significant leukocytosis and thrombocytopenia. Initial chest radiograph typically shows multiple nodular infiltrates and small pleural effusions. CT scans of the neck and lungs aid in diagnosis by identifying thrombus in the jugular veins and cavitary lung lesions.10 Laboratory confirmation is obtained when F. necrophorum grows in blood or fluid cultures. Of note, this organism can take 2 to 7 days to grow.10 All our patients had radiographic evidence of jugular vein thrombosis as well as septic pulmonary emboli, and Fusobacterium spp. were isolated from each. One case was complicated by empyema requiring thoracostomy tubes, and another had acute respiratory distress syndrome and seizures (see Table 1).
Key Features in Lemierre Syndrome
The differential diagnosis of Lemierre syndrome includes infectious mononucleosis, parapharyngeal abscess, pneumonia, and other conditions causing septic emboli such as endocarditis.10
Treatment is directed at oral anaerobes.8 Fusobacterium spp. have 100% sensitivity to metronidazole, ticarcillin-clavulanate, cefoxitin, and imipenem15 and are resistant to gentamicin and quinolones.16 In addition, resistance rates to penicillins and macrolides are as high as 22% and 66%, respectively.15,17,18 Duration of treatment is not well established, ranging from 9 to 84 days depending on severity and patient response.14 Patients are generally treated with intravenous antibiotics for 2 to 3 weeks until clinical improvement, followed by oral treatment to complete a 4- to 6-week course (see Table 2). 12 After obtaining sensitivities, 2 of our patients were discharged on clindamycin. The patient in case 1 was discharged on piperacillin-tazobactam given her good clinical response to that antibiotic. Persistent symptoms despite adequate antimicrobial coverage may suggest loculated abscesses or infectious foci. Any parapharyngeal or peritonsillar abscess, empyema, septic arthritis, or other cavitation should be drained.19,20
Antibiotic Treatment of F. necrophorum Infections
Anticoagulation remains controversial in Lemierre syndrome.21 Clinical practice varies widely and no consensus exists. Most pediatric cases reported in recent years received anticoagulation,22 but overall, there are limited data and no randomized controlled trials. Possible indications for anticoagulation include lack of improvement despite 48 to 72 hours of adequate antimicrobial therapy, concomitant thrombophilia,21 and advancement of the jugular vein thrombosis.23 Optimal duration is not known. Cardiovascular and respiratory support may be required in the septic patient, as in case 3. In rare cases, surgery is required for excision of persistent thrombi.24 Overall, emphasis should be placed on prompt and appropriate antimicrobial therapy, which results in reported mortality rates of 0% to 18%,14 compared with 25% when antibiotics are held for 4 days or more.10
With prompt use of antibiotics, the prognosis for Lemierre syndrome is good. However, as demonstrated by our cases, morbidity can be significant in otherwise healthy, young patients. Fatalities do still occur, particularly in cases of F. necrophorum meningitis, where mortality rates reach 30%.6
Conclusion
Lemierre syndrome is a rare, potentially fatal illness that is often preceded by a commonly seen infection in primary care settings—pharyngitis. The incidence may be increasing. Primary care providers should be aware of the syndrome and suspect it in young patients with an initial oropharyngeal infection, who subsequently show signs of systemic illness or pulmonary involvement. Rapid diagnosis and appropriate treatment can make the critical difference in preventing consequent morbidity and mortality.
Acknowledgments
We thank Petra Lamon, BSRT, Radiology Education Coordinator at the University of Washington Medical Center, for her assistance in obtaining images for this manuscript.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication November 5, 2007.
- Revision received February 22, 2008.
- Accepted for publication March 4, 2008.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Lemierres syndrome with cavernous sinus thrombosis caused by dental infection
- Internal jugular vein thrombosis associated with Granulicatella adiacens
- Lemierres syndrome: a forgotten life-threatening entity
- Lemierres syndrome: a rare cause of sepsis presenting with an absence of throat symptoms
- Lemierre's syndrome: forgotten, but not absent
- Hepatic abscess caused by Fusobacterium necrophorum after a trip to the dentist
- Internal Jugular Vein Septic Thrombophlebitis (Lemierre Syndrome) as a Complication of Pharyngitis
- Doctor, I have a sore throat
- Lemierre syndrome: from pharyngitis to fulminant sepsis
- Optimism: A Good Theme for Family Medicine