
Article Figures & Data
Figures
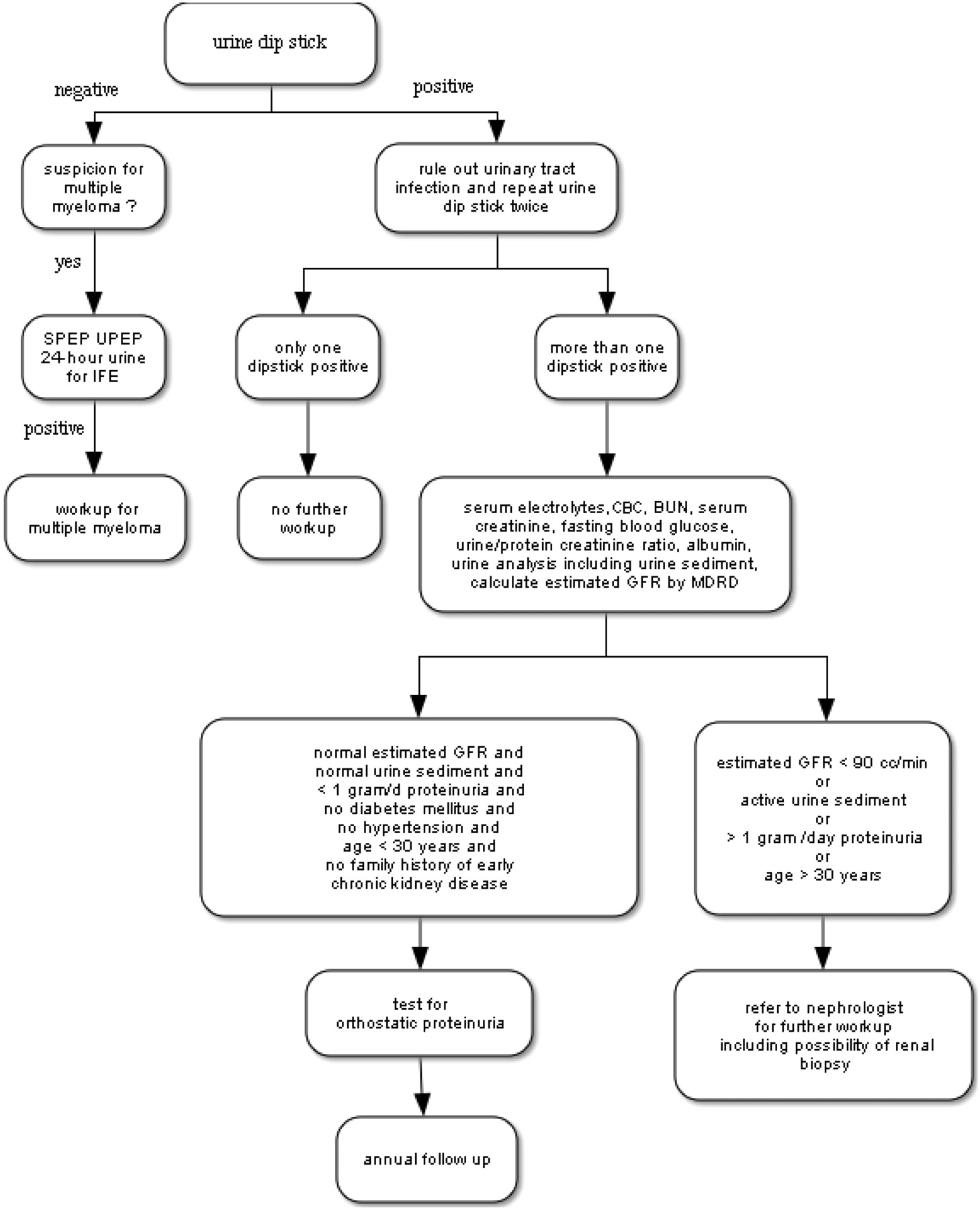
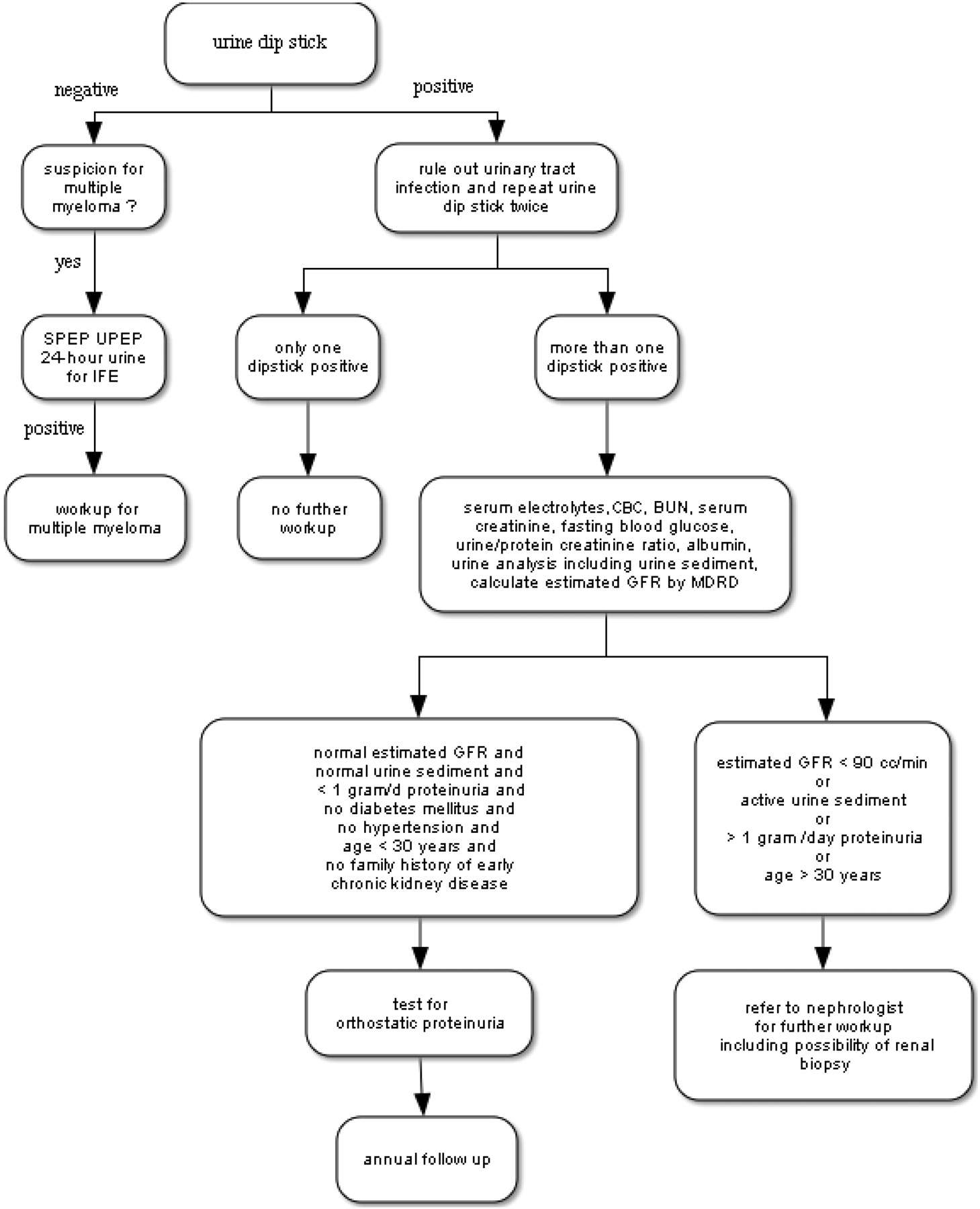
- Figure 1.
Algorithmic approach to proteinuria. SPEP, serum protein electrophoresis; UPEP, urine protein electrophoresis; IFE, Immunofixation electrophoresis; GFR, glomerular filtration rate; MDRD, Modification of Diet in Renal Disease equation.
Tables
Albuminuria Proteinuria Physiologic range proteinuria <20 mg/day (15 μg/min) <150 mg/day Microalbuminuria 30–300 mg/day (20–200 μg/min) Macroalbuminuria >300 mg/day (>200 μg/min) Nephrotic range proteinuria >3.5 g/day Cause Renal Manifestation Clinical Presentation Laboratory/Imaging Diabetes mellitus type 1/type 2 Ranging from microalbuminuria to nephrotic range proteinuria; most common etiology of end-stage renal disease in the US Polyuria, polydipsia, nocturia, weight loss Fasting plasma glucose ≥126 mg/dL (7.0 mmol/L) Hypertension Protein excretion is usually less than 1 g/day13 Often asymptomatic (excluding hypertensive crisis) Retinopathy, LVH, atherosclerosis, small kidneys Pre-eclampsia Nephrotic syndrome,* decreased GFR compared to healthy pregnant women14 Edema Hypertension Multiple myeloma SCr is increased in 50% of patients15; urine protein is not detected on urine dipstick; sulfosalicylic acid test and UPCR detect proteinuria Pallor, radiculopathy, peripheral neuropathy, bone pain in the back or chest is present in 60% of patients27 Monoclonal protein in serum and/or protein electrophoresis, lytic lesions and fractures on x-ray, hypercalcemia Light chain deposition disease Most commonly associated with multiple myeloma; in rare cases it is occurs with lymphoma Related to renal, cardiac, or hepatic involvement Tissue deposition of kappa light chains, urinary light chain excretion Primary amyloidosis Nephrotic syndrome with or without renal insufficiency Peripheral neuropathy, macroglossia, hepatomegaly Amyloid deposition on biopsy; evidence of a clonal plasma cell proliferative disorder HIV nephropathy Nephritic syndrome,† slowly progressive renal dysfunction More common in African-American patients; nephritic syndrome HIV positive, normal to big kidney size Immunoglobulin A nephropathy Nephritic syndrome Hematuria Renal immunoglobulin A deposition; active urine sediment,‡ decreased GFR Minimal change disease and membranous glomerulonephritis Nephritic syndrome Edema, anasarca, foamy urine Hypercholesterinemia, hypoalbuminemia, proteinuria; diagnostic renal biopsy findings Streptococcal glomerulonephritis Ranging from microscopic hematuria to acute nephritic syndrome Recurrent episodes of hematuria 1 to 3 days after URI Kidney biopsy with immunofluorescence shows immunoglobulin A deposits Rare forms of glomerulonephritis, other infectious or systemic diseases Depending on underlying disease patients may have proteinuria with or without an active urinary sediment (red blood cell casts, dysmorphic erythrocytes) Depending on underlying disease ANA, complement C3 and C4, VDRL, hepatitis serology, cryoglobulins * Nephrotic syndrome= more than 3.5 g proteinuria/day, hypoalbuminemia, edema, hyperlipidemia, lipiduria.
† Nephritic syndrome = red to brown urine, proteinuria (usually <3.5 g/day, edema, hypertension, and acute renal failure).
‡ Active urine sediment = red blood cell casts or dysmorphic erythrocytes.
RBC, red blood cell; GFR, glomerular filtration rate; ANA, antinuclear antibodies; HIV, human immunodeficiency virus; LVH, left ventricular hypertrophy; SCr, serum creatinine; URI, upper respiratory tract infection; VDRL, Venereal Disease Research Laboratory.




{kind=link}