
Abstract
Background: To compare the postpartum pelvic floor function of women with sutured second-degree perineal lacerations, unsutured second-degree perineal lacerations, and intact perineums.
Methods: A prospective cohort of nurse-midwifery patients consented to mapping of genital trauma at birth and an assessment of postpartum pelvic floor outcomes. Women completed validated questionnaires for perineal pain and urinary and anal incontinence at 12 weeks postpartum and underwent physical examination to assess pelvic floor strength and anatomy at 6 weeks postpartum.
Results: One hundred seventy-two of 212 (80%) eligible women provided follow-up assessment data at 6 or 12 weeks postpartum. Women with an intact perineum (n = 89) used fewer analgesics (P < .002) and had lower pain scores at the time of hospital discharge than women with second-degree lacerations (sutured, n = 46; unsutured, n = 37; intact, n = 89) (P ≤ .02). The sutured group was more likely to use analgesics (52%) than the unsutured (35%) or intact (23%) groups at time of hospital discharge (P < .002), although pain scores were not different between sutured and unsutured groups. Postpartum reports of urinary or anal incontinence, sexual inactivity, or sexual function scores did not vary between groups. Weak pelvic floor exercise strength was more common among the women with second-degree lacerations compared with women with an intact perineum (53% vs. 28%; P = .03) but did not differ between sutured (58%) and unsutured (47%) groups (P = not significant). Likewise, perineal body or genital hiatus measurements did not vary between groups (P = not significant).
Conclusions: Women with sutured lacerations report increased analgesic use at the time of hospital discharge compared with women with intact perineums or unsutured lacerations. At 12 weeks postpartum, no differences were noted between groups regarding complaints of urinary or anal incontinence, sexual inactivity, or sexual function.
Is there any benefit to not suturing spontaneous second-degree obstetrical perineal lacerations? Second-degree lacerations involve the muscles of the perineal body but do not extend into the external anal sphincter. These lacerations are common; the majority of perineal trauma in births without episiotomy is classified as second-degree.1 Repair of second-degree lacerations has been considered standard practice by physicians throughout the history of modern obstetrics and is one of the most commonly performed surgical procedures in the United States.2 In contrast, some midwives do not suture second-degree lacerations if they are hemostatic and approximate well because suturing has been shown to increase pain and interfere with initiation of breastfeeding.3,4
Postpartum alterations in urinary and anal continence, sexual function, dysparunia, and perineal pain are common. Postpartum urinary incontinence is linked to both pregnancy5 and childbirth.6 Anal incontinence symptoms occur in 20% to 50% of women with known anal sphincter lacerations; however, up to 50% of women with postpartum anal incontinence symptoms do not have a reported anal sphincter laceration.7 Women who have episiotomies or spontaneous perineal lacerations complain of increased perineal pain, decreased sexual satisfaction after giving birth, and delayed return of sexual activity compared with women who give birth with an intact perineum.8,9 It is not known whether suturing second-degree lacerations has any effect on the incidence of postpartum pelvic floor dysfunction.
Second-degree lacerations occur in approximately 18% of the University of New Mexico nurse-midwifery patients and the decision whether or not these lacerations are repaired is based on the discretion of the midwife.10 This study was initiated to determine whether functional outcomes of childbirth (including perineal pain, sexual function, and anal and urinary incontinence) differed in women with unsutured second-degree perineal lacerations compared with women with sutured second-degree lacerations or women who delivered over an intact perineum.
Methods
During prenatal visits, a prospective cohort of 576 midwifery patients (at least 18 years of age and able to speak and write English or Spanish) gave written informed consent to the documentation of genital trauma and perineal repair at birth and to the assessment of functional pelvic floor outcomes postpartum. All women in the current study were also enrolled in a randomized trial to evaluate the impact of perineal warm compresses and massage on genital tract trauma, the results of which have been previously published.10 All women were delivered vaginally at the University of New Mexico Health Sciences Center and were attended by a member of the nurse-midwife group. The rates of episiotomy and operative vaginal delivery were less than 1% and 2%, respectively; these women were excluded from further analyses. The decision of whether or not to repair second-degree perineal lacerations was at the discretion of the attendant nurse-midwife.
Immediately after birth, data collection included demographic data, care measures during labor, birth events, and a detailed map of genital tract trauma. Depending on the location of the trauma, it was defined as perineal, labial, vaginal, periurethral, or clitoral. Second-degree lacerations involved the muscles of the perineal body without transgressing the anal sphincter complex.
The suture technique and suture (delayed absorbable 2-0 or 3-0 polyglactin 910) were standardized for the repair of perineal lacerations.11,12 The apex of the laceration was identified and, after an anchoring suture was placed, a running suture was conducted to the hymenal ring. Care was taken to incorporate the underlying vaginal fascia as well as the vaginal mucosa. The suture was locked only if excessive bleeding was encountered from the edges of vaginal and perineal lacerations. Interrupted sutures were placed to bring together the transverse perineal and the bulbocavernosus muscles. At the discretion of the attendant, a subcuticular running suture was placed to repair the skin edges. Anterior lacerations were repaired as needed to restore anatomy and achieve hemostasis.
The 6-week postpartum visit included a physical examination of the perineum, with measurement of the perineal body and the genital hiatus (vaginal opening) according to the Pelvic Organ Prolapse Quantification System.13,14 Pelvic floor exercise strength was graded by digital examination on a scale of 0 to 5, with 0 indicating inability to volitionally contract the pelvic floor.13 For analysis, pelvic floor muscle strength was further dichotomized into “weak” (indicating a muscle strength of nil, flicker, or weak) or “strong” (indicating a muscle strength moderate, good, or strong). The midwife also made a subjective assessment of the appearance of the perineum to categorize it as “intact” or “not intact.”
Validated questionnaires were used to assess functional outcomes. Perineal pain was assessed using the Present Pain Intensity and Visual Analog Scale components of the modified short-form McGill pain questionnaire15 at the time of discharge, at 6 weeks, and at 3 months. Anal incontinence was defined as a score greater than zero on the Fecal Incontinence Scale; higher scores indicate worse anal incontinence.16 Fecal incontinence (loss of loose or formed stool) was defined as a score greater than 3 on the Fecal Incontinence Scale. Urinary incontinence was defined as an affirmative answer to the question “Do you leak urine when you do not mean to?”17,18 The impact of urinary incontinence on quality of life was measured with the Incontinence Impact Questionnaire-7, with higher scores indicating greater impact on quality of life. Incontinence measures were taken at 6 weeks and 3 months postpartum. Women were asked if they had been sexually active since the birth of their baby. Sexual function was evaluated at 3 months with the Intimacy Relationship Scale (IRS).19 Higher IRS scores indicate better sexual function.
Before initiation of the study, the principal investigators held teaching sessions to standardize intrapartum evaluation of genital tract trauma, repair of perineal lacerations, and assessment of postpartum pelvic floor muscle strength. Midwives viewed a teaching video on measurement of the perineal body and genital hiatus and had a training session with a clinician experienced with the Pelvic Organ Prolapse Quantification System measurements. The accuracy and reliability of genital tract trauma assessments has been previously published.10 If women did not return for their 6-week or 3-month evaluations, they were asked to complete questionnaires by telephone interview. Women who completed both interviews were compensated $10.00. The study was a collaborative effort between the departments of Obstetrics and Gynecology, Family Medicine, and the College of Nursing at the University of New Mexico Health Sciences Center. Approval was obtained by the University of New Mexico Human Research Review Committee.
For all functional outcomes, descriptive statistics (means, proportions) were generated (urinary and anal incontinence scores; perineal measurements; and the evaluation of pelvic floor exercise strength, pain, and sexual function). Fisher's exact test and t tests were used for comparison of continuous and categorical variables between women who did and did not follow up. Comparison of women with trauma versus those with no trauma was assessed by one-way analysis of variance (for continuous dependent variables) or χ2 tests for the differences in proportions for all outcome measures. Analyses were performed using SAS version 9 (SAS Inc., Cary, North Carolina, 2005). Significance was set at P ≤ .05.
Results
Between March 2002 and December 2005, 576 women were recruited and gave vaginal birth (Figure 1). Eleven women underwent episiotomy and/or operative delivery (known risk factors for pelvic floor dysfunction) and were excluded from this analysis. Second-degree perineal lacerations occurred in 97 of 565 (17.2%) women; 53 of the second-degree lacerations (55%) were sutured and 44 (45%) were not sutured. One hundred eighteen women with an intact perineum comprised a third group for comparison with the women who had sutured and unsutured second-degree lacerations. Multiparity, less education, and smaller fetal weight were associated with an intact perineum (Table 1).
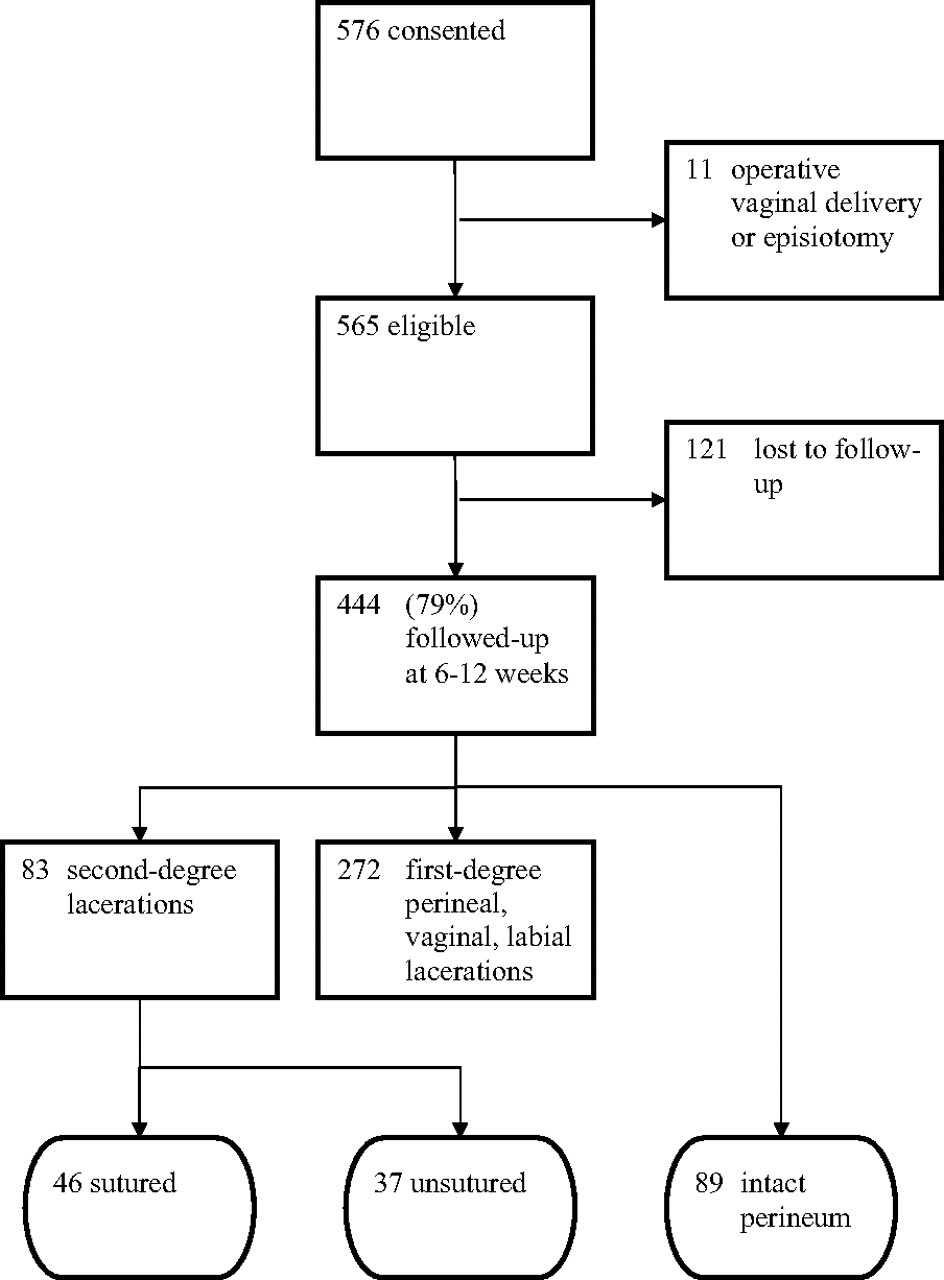
FACT study participant flow chart.
Demographic, Maternal, and Labor Characteristics
Follow-up assessment was provided at either 6 weeks or 3 months postpartum by 444 of 565 (79%) women (Figure 1). One hundred seventy-two of the 215 women (80%) in the 3 comparison groups included in this study provided follow-up data: 83 of 97 (86%) women with second-degree lacerations and 89 of 118 (75%) women without trauma (Table 1). There was no difference between 6-week and 3-month functional outcomes (P was not significant among all); 6-week data were used only if 3-month data were not available. Women who were lost to follow-up completed fewer years of education (P = .001) and had a higher body mass index (P = .049) but did not differ with respect to age, infant birth weight, maternal weight gain, length active pushing in the second stage of labor, ethnicity, use of oxytocin, use of epidural, type of pushing efforts (directed versus nondirected), or maternal position at birth (P was not significant among all).
Women with an intact perineum had less use of pain medicines and lower pain scores at the time of hospital discharge than did women with second-degree lacerations. The sutured group was more likely to use analgesics than the unsutured or intact groups at the time of hospital discharge, although pain scores were not different between sutured and unsutured patients at the time of discharge or at postpartum follow-up visits (Table 2). No differences between groups were observed in reports of urinary or anal incontinence, or Incontinence Impact Questionnaire-7 scores. The groups also did not differ in reports of sexual activity or in the mean IRS scores at 3 months postpartum (Table 2).
Pelvic Floor Complaints Up to 3 Months Postpartum
The postpartum pelvic examination at 6 weeks revealed weaker pelvic floor muscle strength in the women with second-degree lacerations compared with women with an intact perineum; however, in women with second-degree lacerations, there was no difference in pelvic floor muscle strength between the sutured versus unsutured groups (Table 3). Groups did not differ in the proportion of women with a lengthened genital hiatus or shortened perineal body. The proportion of women with subjectively gaping asymmetrical or open perineal wounds was similar at 6 weeks between the groups.
Perineal Exam Findings at 6 Weeks Postpartum
Discussion
Women with sutured second-degree perineal lacerations used significantly more analgesics during their postpartum stay than women with unsutured lacerations, although pain scores were not different between the sutured and unsutured groups. There were no differences between the sutured and unsutured groups with respect to postpartum sexual activity or function, anal or urinary incontinence, pelvic floor muscle strength, or perineal body or genital hiatus measurements.
Little high-quality evidence regarding optimal repair of second-degree perineal trauma exists. Studies have demonstrated decreased postpartum pain after repairs that do not suture the skin22 and with the use of continuous subcutaneous rather than interrupted transcutaneous skin sutures.23 Women who had repairs that left the skin unsutured were also less likely than women with sutured perineal skin to report that the perineal area felt different compared with how it felt before delivery.24 The use of a synthetic absorbable suture, such as polyglactin, for the repair of perineal lacerations results in less pain than a chromic suture but occasionally requires removal because of its longer life.25 A fast-absorbing polyglactin 910 may be the optimal suture23,26 because suture removal is seldom required. We standardized our repair of perineal laceration to the use of a polyglactin 910 (Vicryl) 2-0 or 3-0 suture, which should help to mitigate differences in pain or dehiscence that may have been caused by differences in suture material.
Two small studies of primiparous women have compared perineal outcomes in women with sutured lacerations versus those with unsutured second-degree lacerations. The SUNS trial found significantly better wound approximation at 6 weeks in the sutured group and no difference in postpartum pain or depression between groups.3 A small randomized controlled trial (n = 80) of first- and second-degree lacerations showed no difference in perineal wound healing or postpartum pain between groups, but more women in the sutured group felt the laceration repair had a negative impact on breastfeeding.4 Both of these trials failed to differentiate between first- and second-degree lacerations, did not exclude women with episiotomy, and did not examine the impact of not suturing lacerations on functional outcomes including urinary or anal incontinence. In the current study we also found no impact on functional pelvic floor outcomes from not suturing lacerations.
Limitations of the present study include the lack of a standardized system for describing the depth of second-degree laceration, the inclusion of both nulliparous and multiparous patients, and the lack of long-term follow-up for functional outcomes. In addition, we had a small sample size, but a post hoc power analysis, with 80% power and an α value of 0.05, indicated that our sample size was adequate to detect a 31% difference in women who leaked compared with those who did not leak postpartum, a difference that we felt would be clinically significant. The study was prospective but not randomized, and it is possible that the midwives decided to suture women with more severe second-degree lacerations. The use of a defined methodology, such as that developed by Nager27 for measuring the depth of second-degree lacerations, would allow for comparisons that include laceration depth to determine whether functional benefits exist in women with deeper second-degree lacerations. Finally, women may have had sustained pelvic floor damage from a previous delivery and not from the present delivery. Although follow-up is limited to 3 months postpartum, women with persistent stress urinary incontinence at 3 months postpartum have a 91% risk of having stress urinary incontinence at 12 years.28 Similar short-term predictors for anal incontinence and sexual dysfunction do not exist.
Second-degree perineal trauma occurs in close to 20% of births without episiotomy. We found no benefit to the suturing of second-degree lacerations on postpartum pelvic floor function in the short term. If the repair of these lacerations has no benefit on functional outcomes, then suturing should be deferred because of the increased postpartum pain of a sutured laceration. Larger cohort studies with a longer follow-up period and randomized trials comparing sutured and unsutured second-degree perineal lacerations with regard to functional outcomes are indicated.
Acknowledgments
We thank Clifford Qualls, PhD, for his statistical assistance.
Notes
This article was externally peer reviewed.
Funding: This work was supported in part by the National Institutes of Health: DHHS/NIH/NCRR/GCRC grant # 5M01 RR00997 and by 1R01HD049819-01A2.
Conflict of interest: none declared.
- Received for publication December 22, 2006.
- Revision received May 11, 2007.
- Accepted for publication May 15, 2007.




{kind=link}