
Abstract
Transcranial Doppler (TCD) is a diagnostic tool that can be used at bedside to assess the cerebral vasculature noninvasively. It is inexpensive, safe, and reliable when compared with other techniques. It can be repeated multiple times and can be used for continuous monitoring if needed. Screening of children with sickle cell disease to assess and prevent ischemic strokes and monitoring for vasospasm after subarachnoid hemorrhage are well established, evidenced based utilizations of TCD. It is useful for the evaluation of occlusive intracranial vascular lesions with many emerging indications in the management of ischemic stroke. TCD with micro-bubble enhancement has comparable sensitivity to transesophageal echocardiogram in detecting right-to-left atrial cardiac shunts. TCD is underused as a clinical tool despite well established indications. The pressure to contain increasing medical cost will likely result in increased utilization of this test in future.
Christian Johann Doppler, a mathematician, physician, and astronomer, first described the Doppler principle in 1843. Its use in neurology was first reported in 1982,1 and since then, its convenience and growing range of uses have made it an attractive tool to evaluate the cerebrovascular tree in patients with neurovascular disorders. Transcranial Doppler (TCD) is a noninvasive ultrasound device that allows real-time evaluation of the intracranial cerebral circulation. It is currently under-utilized in part due to the lack of awareness about the diagnostic usefulness of this test. In this article, we will review TCD testing as a procedure and discuss its clinical applications of special interest to the primary care physician.
Examination and Doppler Instrument
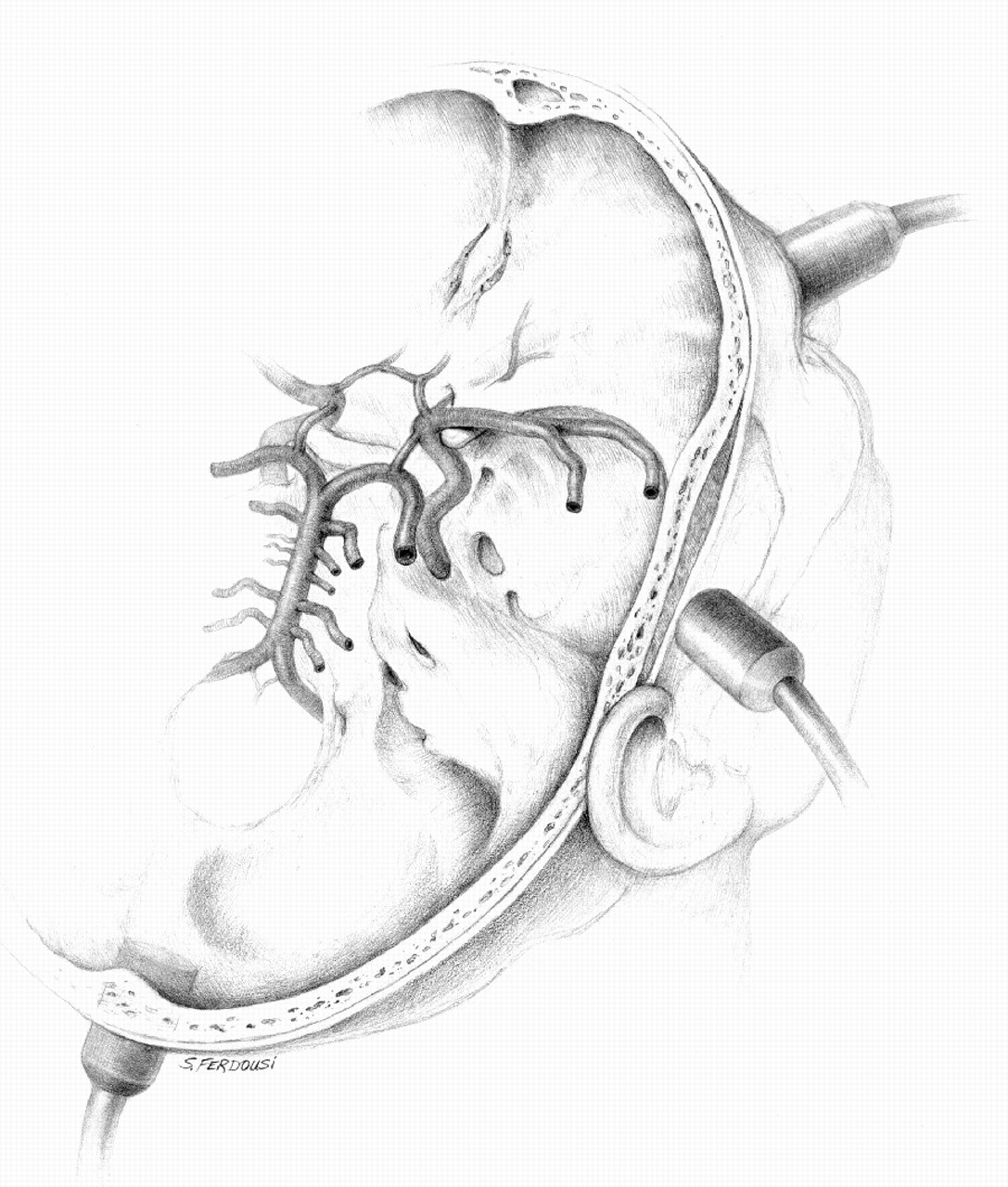
Ultrasound examination of a vessel by means of TCD is referred to as insonation. The TCD probe is placed over different “acoustic windows” that are specific areas of skull where there is a lack of boney covering or the cranial bone is thin (Figure 1). The transtemporal (temporal) window is used to insonate the middle cerebral artery (MCA), the anterior cerebral artery (ACA), the posterior cerebral artery (PCA), and the terminal portion of the internal carotid artery (TICA), before its bifurcation. The transorbital (orbital) window gives access to insonate the ophthalmic artery (OA) as well as the internal carotid artery at the siphon level. The transforaminal (occipital) window allows insonation of the distal vertebral arteries (VA) and the basilar artery (BA). Finally, the submandibular window allows insonation of the more distal portions of the extracranial internal carotid artery.
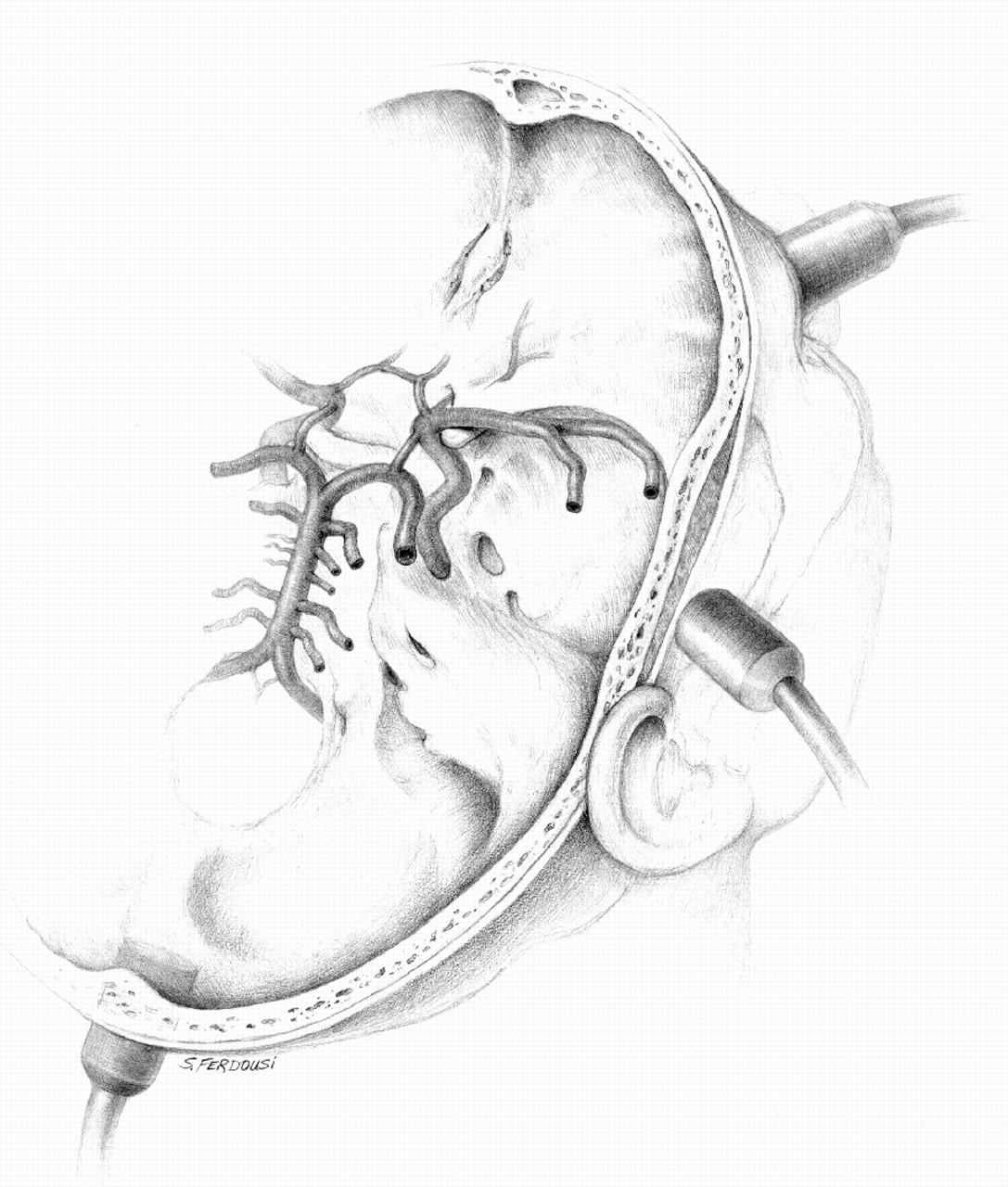
TCD probe positions over different acoustic windows of the skull.
TCD does not allow direct visualization of insonated vessels like carotid Doplex, rather it is an indirect evaluation by means of an ultrasonic beam of 2 MHz frequency that is produced from piezoelectric crystals that have been stimulated electrically. This beam bounces off the erythrocytes within the insonated artery. The reflected signal is received by the transducer and converted to an electric signal (Figure 2). This information is subtracted from the transmitted signal and then processed to obtain a waveform that allows accurate determination of blood flow velocities, direction of flow, and also allows for certain calculated parameters to be added to the evaluation. The pulsatility index (PI) is one of the useful calculated parameters, and it is considered a reliable marker of resistance distal to the insonated site. It is usually calculated by the Gosling equation.2 PI = (Peak systolic velocity − end diastolic velocity)/mean velocity.
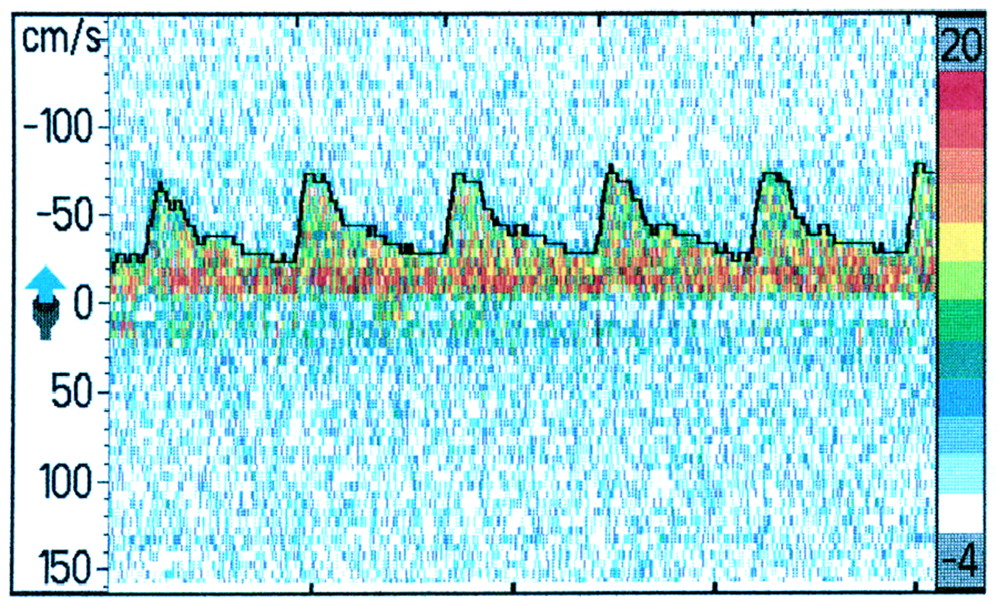
TCD screen waveform with velocity scale on the left.
Introduction to Basic Cerebrovascular Hemodynamics
The relationship between resistance, pressure, and flow can be expressed by Ohm’s law: flow = pressure/resistance. If we want to apply this relationship to cerebrovascular hemodynamics it translates to cerebral blood flow = cerebral perfusion pressure/cerebrovascular resistance (CBF = CPP/CVR).
CPP can be calculated from the mean arterial blood pressure and the intracranial pressure (CPP = MAPB-ICP). CVR is influenced in physiologic states by constriction and dilatation of the small size vessels (arterioles) in the brain. In pathologic states, focal changes in resistance can be seen immediately behind an area of significant stenosis.
The main goal of brain cerebrovascular hemodynamics is to keep CBF stable despite alterations in CPP and CVR. This is usually achieved by vascular autoregulation, a process that lowers resistance by inducing vasodilatation to maintain CBF when CPP is decreased. In cases of increased CPP (like increased BP), increasing resistance by vasoconstriction occurs, and thus CBF is maintained.
TCD Examination and Interpretation of Findings
Different depth range, flow direction, and normal age-related flow velocity (FV) ranges have been established for each vessel. The vessels are identified using these parameters for each of the windows already discussed. Table 1 is a simplified illustration of these values.3 TCD measurements are influenced by different physiologic and pathologic factors and by vasoactive medications (Table 2).
Accepted Guidelines for a Normal TCD Study
Effects of Different Physiological States on TCD Flow Velocity
Basic Observations Regarding Blood FVs and PI in Different Vascular Scenarios
Pure focal narrowing at the site of insonation will cause an increase in FV.
Narrowing or obstructing lesions proximal to the insonation site will cause a decrease in FV observed at the insonation site.
Downstream (distal) decrease in vascular resistance (as in the presence of arteriovenous malformation will increase FV and decrease PI at the site of insonation.
Downstream increased vascular resistance (as in stenosis or obstruction) will decrease FV and increase PI proximal to lesion.
Clinical Applications
The clinical applications of TCD are growing. The American Academy of Neurology published TCD guidelines for clinicians.4 Although directed to neurologists, these guidelines may be useful for the primary care physician.
Sickle Cell Disease
This may be one of the most important TCD applications, and it is of very special interest for the primary care physician. Recent guidelines regard the use of TCD4 as a type A level of evidence (established as useful predictive for suspected condition), and class I (evidence provided by prospective studies in broad spectrum of persons with suspected condition) screening tool to assess stroke risk in children aged 2 to 16 years with sickle cell disease.
Sickle cell disease is associated with progressive occlusion of large intracranial arteries (most frequently the intracranial ICA and MCA). Total occlusion of any one of these arteries will lead to a massive stroke. These arteries are very accessible to TCD insonation and TCD can monitor FVs over time.
According to the TCD criteria for sickle cell disease, a MFV of up to 170 cm/s is considered normal and a MFV of 171 to 199 cm/s is called “conditional.” MFV of equal or greater than 200 cm/s is considered abnormal and require transfusion.5
A mean FV (MFV) of 200 cm/s or greater is accompanied by a stroke risk of 40% within the next 3 years. Transfusion, with reduction of hemoglobin S to less than 30% of total hemoglobin, will lower this risk by 70% compared with standard care alone.5–8 An optimal timing to re-screen children with sickle cell disease and normal TCD is not set, but a repeat TCD examination every 6 months seems to be a reasonable objective.
Intracranial Vasospasm
Intracranial vasospasm is the constriction of cerebral blood vessels due to the presence of blood in the subarachnoid space after a trauma or rupture of cerebral aneurysm. The vasospasm—if severe—may result in ischemia to the brain and is associated with an increase in mortality of 1.5- to 3-fold during the first 2 weeks after subarachnoid hemorrhage (SAH).9 Vasospasm typically occurs within 3 to 21 days after SAH and may last for 12 to 16 days.10 Clinically this manifests a deterioration of the patient’s level of consciousness, new focal neurological signs, and headaches.
The pathophysiological changes that underlie vascular constriction after SAH is not completely known but may include changes within the vessel walls themselves, alteration of levels of vasoactive substances, and broader pathologic conditions such as immune responses, inflammation, and oxidative damage.
Subarachnoid hemorrhage occurs in an estimated 25,000 to 30,000 people in the United States each year.10 It could be identified by TCD up to 1 to 2 days before it becomes clinically symptomatic allowing for immediate initiation of triple H therapy.
Vasospasm that follows SAH causes increased FV inside intracranial vessels. This can be detected by TCD indicating the need for treatments before the onset of ischemia. TCD is already in use to diagnose and monitor management of vasospasm in emergency and critical settings according to established guidelines.11–16 Usually a baseline TCD is performed at the earliest possible time (day 0); a daily TCD is then performed during days 3 to 10. A mean FV of 120 cm/s is considered a sign of mild spasm and a value above 180 cm/s is considered a sign of severe spasm. Mean FV obtained by TCD was found to correlate well with the angiographic residual lumen diameter of the MCA, and it was found to have excellent specificity (100%) but only good sensitivity (58.6%) in diagnosing vasospasm only due to the involvement of vessels that are not evaluated by TCD at times.13 The accuracy of TCD in the diagnosis of cerebral vasospasm can be increased by using the Lindegaard ratio (see Table 3). By calculating the MFV ratio between MCA, ACA, and the ipsilateral ICA (VMCA/VICA or VACA/VICA), changes due to generalized hyperemia can be distinguished from vasospasm.17
TCD’s Mean Flow Velocity Criteria for Cerebral Vasospasm
Arterial Stenosis and Occlusion
TCD measurements that correlate with stenosis would be increase FV at the stenotic site.
Decrease FV downstream from a stenotic site.
Decrease FV proximal and increase PI proximal to the stenotic site.
Increase FV and/or reverse flow in collateral vessels (like the finding of reverse blood flow in the OA in case of ipsilateral carotid artery occlusion and the finding of increased FV of the first segment of contralateral ACA shunting blood through the anterior communicating artery to the contralateral hemisphere in the same scenario).
In a case of total occlusion, there should be no flow signal from the occluded site. Increased velocity and/or reversed flow in the collateral vessels may also be seen. Other vessels in the same window should be accessible for insonation. A decrease in blood FV proximal to the site of the occlusion may also be seen. The presence of multiple findings described above increase the likelihood of the presence of stenosis or occlusion in a given vessel.18
Similar TCD approaches are already utilized in some centers for the detection of occluded vessels in acute and subacute stroke. It is the noninvasive test of choice to evaluate the cerebrovascular tree when a contraindication exists to the use of MRI and CT and cerebral angiography. TCD testing has a high positive predictive value of >80%19 making TCD an attractive tool for assessing the cerebrovascular tree in low risk patients.
In the Midwestern region of the United States, Medicare pays $62.31 for the professional component and $465.30 for the technical component of MRA of the intracranial vessels and pays additional and a similar amount for MRA of the cervical vessels. It only pays $51.99 for the professional component and $245.47 for a complete TCD study (for both intracranial and extracranial vessels). Since TCD is a noninvasive20,21 and inexpensive technique with no known risks or side effects, it can be an excellent tool for frequent follow-up of vascular lesions to assess effectiveness of a therapy without the concern of subjecting the patient to frequent radiation and the increasing costs of diagnostic testing like MRI.
TCD can also be used to observe the effectiveness of thrombolytic treatment in stroke patients. If the vessel is not recannulized, other treatments can be considered.21
Monitoring for Sources of Emboli and Heart Shunts during Procedures
Microemboli traveling along an insonated vessel will appear as high intensity transient signals (HITS) on the TCD spectrum. Although the exact clinical relevance of these findings remains uncertain, it may identify high-risk status for clinical stroke offering an opportunity to localize the source in patients with multiple potential sources and providing a possible monitoring tool for the efficacy of a chosen treatment.
TCD can also be used as a quality control, training, and monitoring tool inside operation rooms for surgeries with risk of embolization22–24 their contribution to the postoperative neurobehavioral changes.
TCD can detect the presence of right-to-left shunts such as patent foramen ovale (PFO) in patients with contraindications to transesophageal echo (TEE) with similar sensitivity and specificity25–28. This clinic use requires the administration of agitated saline after which the patient performs a valsalva maneuver28. The test is positive for right-to-left shunt if a shower of high signal material (air) is detected in the MCA by TCD 5 to 10 seconds after the intravenous injection of 10 mL of agitated saline26. If this shower of air emboli is detected after a minute of injection, it might indicate the presence of a pulmonary shunt; a diagnosis that cannot be obtained by TEE.
Brain Death (cerebral circulatory arrest)
TCD evaluation of a brain death patient yields a “reverberating or oscillating” pattern of flow (normal arterial blood flow in systole and reversed flow in diastole secondary to the very high distal brain resistant in the brain dead patients) leading to absence of net flow per unit of time.29–32 The reverberating pattern may progress to “no flow” in the advanced stages of brain death. Although it is not a common practice to get a TCD as part of a brain death examination, it can, however, be used as a useful adjunct test.33
Testing for Cerebrovascular Autoregulation
Cerebral autoregulation is the ability to maintain the cerebral blood flow despite minute-to-minute variation in cerebral perfusion rate. In a normal physiologic state, this can be achieved by the arteriolar control over the cerebral peripheral vascular resistance. People with impaired cerebral autoregulation might have a variety of presentations such as headache, dizziness, and syncope.
TCD measurements of FV and PI before and during pharmacological or mechanical manipulation of autoregulation and systemic blood pressure can be used to monitor the reactivity of the intracranial vasculature tree. Breath-holding and acetazolamide administration are two of the most used maneuvers to manipulate cerebral autoregulation.34–36
The breath-holding test is used to assess cerebrovascular reactivity to hypercapnia as calculated by means of the breath-holding index (BHI). The index is calculated by dividing the percent increase in mean FV (MFV) during breath-holding by the breath-holding time (in seconds) that subjects held their breath after a normal inspiration: BHI = {[MFV at the end of breath-holding − resting MFV]/resting MFV} × (100/seconds of breath-holding).
This technique can be useful in testing the candidacy of asymptomatic patients with internal carotid artery stenosis for endarterectomy surgery. Recent data37 showed increased risk of ischemic strokes in patients with severe (>70%) carotid stenosis and impaired autoregulation as tested by TCD. TCD can also assess the potential risk of cerebral ischemia in patients with carotid stenosis going for major anesthesia and surgery. TCD might also be a useful investigation in work up of a patient with vasovagal syncope38–41.
Conclusion: Advantages and Limitations of TCD
TCD is relatively inexpensive, noninvasive, portable and fairly easy to use. It allows frequent repeated measurements and continuous monitoring. Immediate, real time detection of changes in cerebrovascular hemodynamics is possible. It can be utilized by any medical specialty to evaluate several neurovascular disorders.
In many communities (especially rural ones), there is no neurologist and/or MRI machine available for appropriate stroke workup. In those settings and in many other places a “complete” stroke workup consists of carotid Doppler and two-dimensional echocardiogram. This misses the important evaluation of intracranial vasculature. A TCD may be the inexpensive, simple mean to determine which patients must be referred to a specialized center for further evaluation. In addition, and in patients who decline intervention initially, TCD gives a tool for monitoring the identified lesions through the years and evaluate the effectiveness of medical treatment.
Finally, TCD may be the only mean possible to evaluate intracranial vessels in cases when other radiographic means are contraindicated. TCD is a “blind procedure”; its accuracy relies on the knowledge and experience of a trained technician and interpreter. It has limited ability to detect distal branches of intracranial vessels. In 5% to 10% of cases, sufficient penetration of the bone window can not be achieved for ample insonation.
A certificate in neurosonology (TCD and carotid Doppler) is granted by the American neuroimaging society after specific training requirements are met and an examination is passed.
Notes
This article was externally peer reviewed.
Conflict of interest: none declared.
- Received for publication August 4, 2006.
- Revision received October 17, 2006.
- Accepted for publication October 21, 2006.
References




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Sex Differences in Middle Cerebral Artery Reactivity and Hemodynamics Independent from Changes in Systemic Arterial Stiffness in Adult Sprague-Dawley Rats
- Through the looking glass: early non-invasive imaging in TBI predicts the need for interventions
- HOBOE (Head-of-Bed Optimization of Elevation) Study: Association of Higher Angle With Reduced Cerebral Blood Flow Velocity in Acute Ischemic Stroke
- Inside the March/April 2008 Issue and the Most Frequently-Read Articles in 2007