
Article Figures & Data
Figures
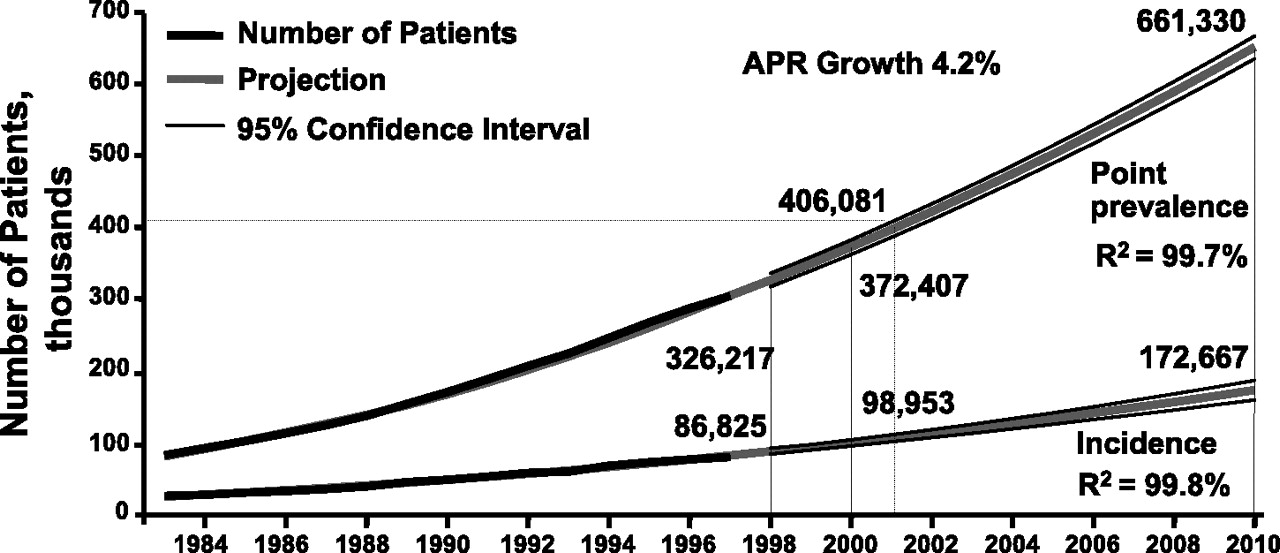
- Figure 1.
The rising tide of end-stage renal disease (ESRD) patients. Projection of incident and point-prevalent ESRD patients for the year 2010. There has been a steady increase in the incidence of ESRD in the US population since 1980 with a tremendous increase in the expenditure. The prevalence of ESRD is projected to increase by 77% from 2000 to 2010.1
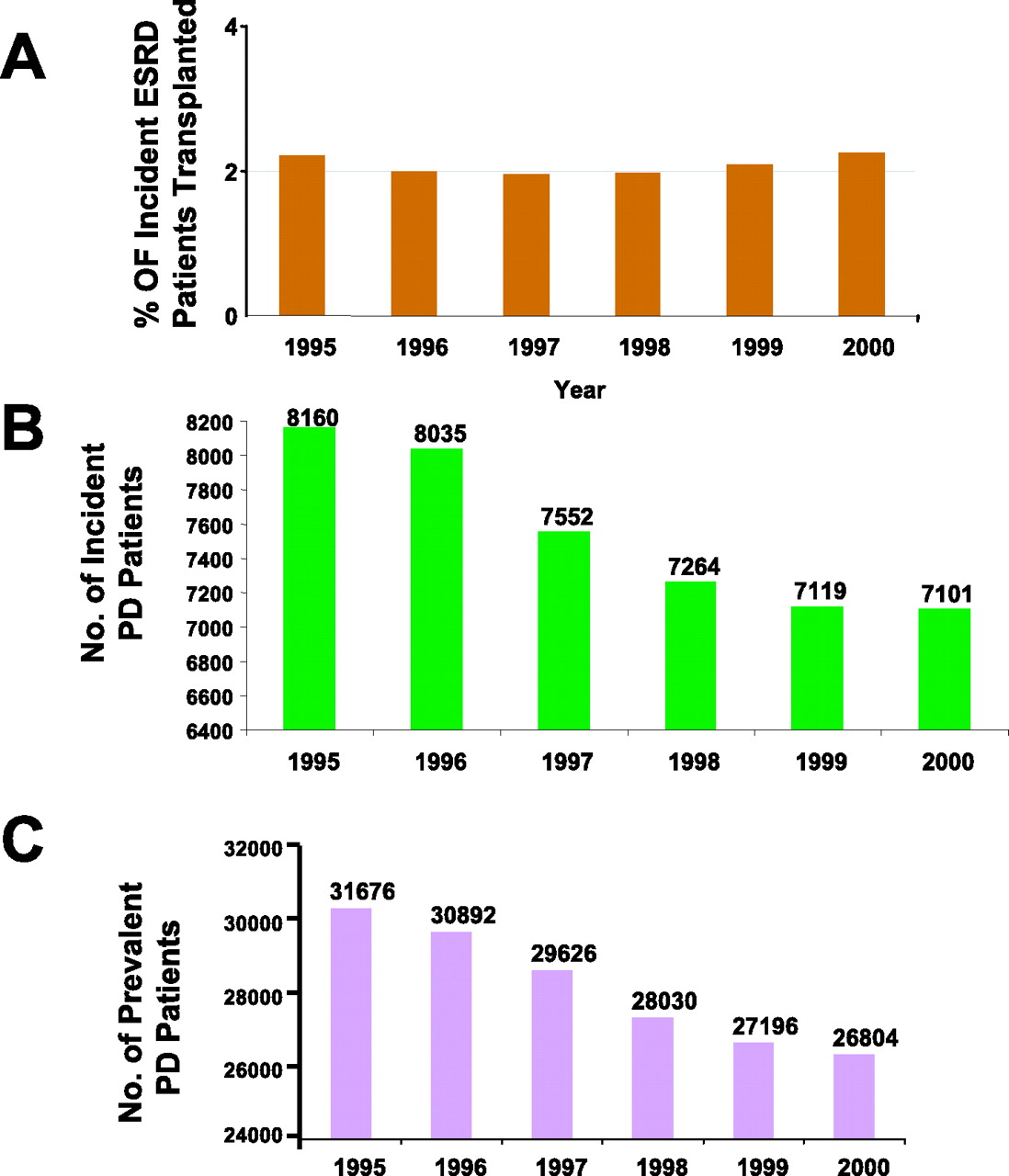
- Figure 2.
Growth of various renal replacement therapies. Whereas the end-stage renal disease (ESRD) patient population is growing steadily, the growth of various renal replacement therapies is disproportional. Although there is a steady growth of hemodialysis population, the proportion of incident ESRD patients receiving kidney transplant has remained constant at approximately 2% (A). On the other hand, the number of incident ESRD patients receiving peritoneal dialysis (PD) has progressively declined since 1995 (B) such that the prevalent PD population has decreased by 15% since 1995 (C).1
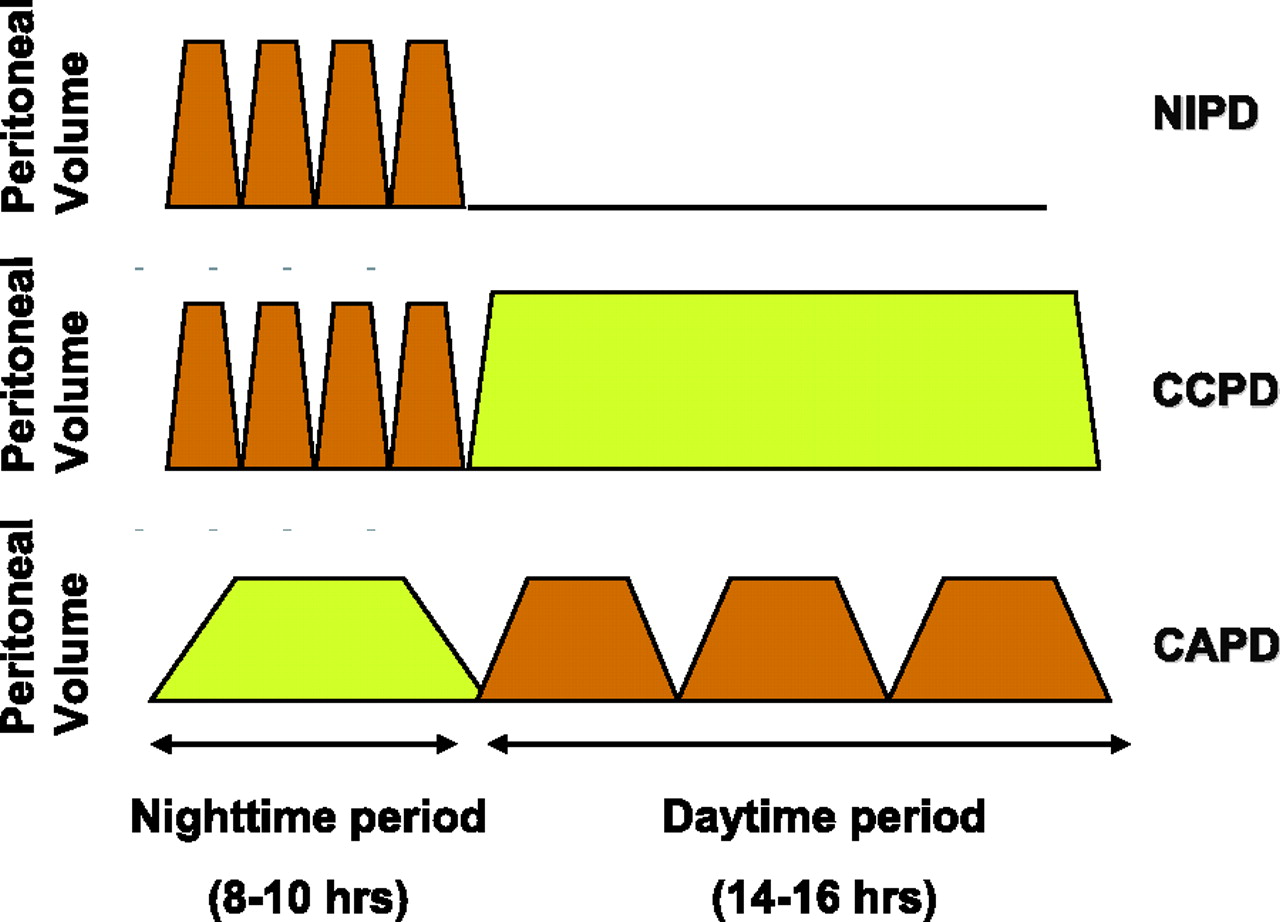
- Figure 3.
Various peritoneal dialysis (PD) schedules. NIPD, nocturnal intermittent PD; CCPD, continuous cycler-assisted PD; CAPD, continuous ambulatory PD.
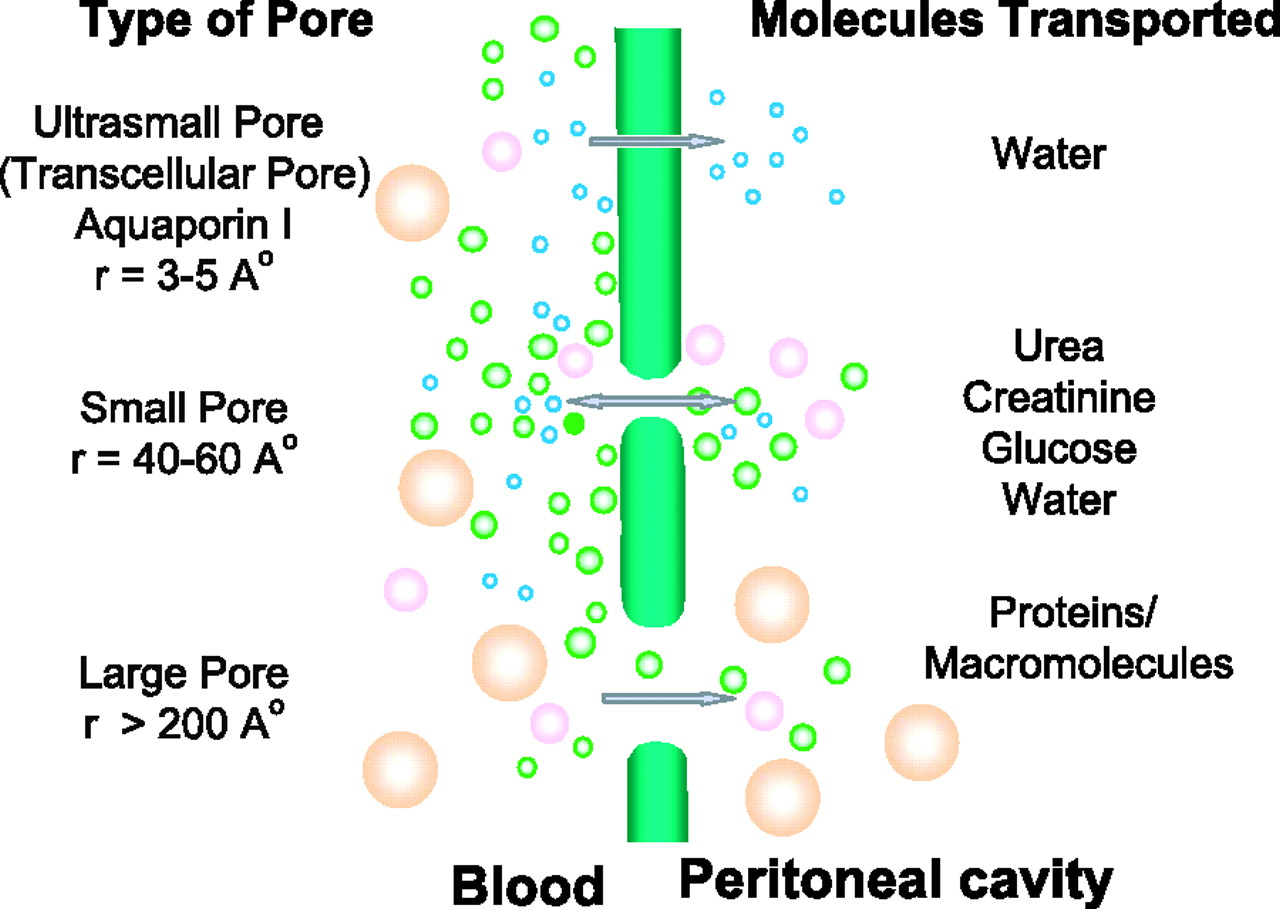
- Figure 4.
Three-pore model of the peritoneal membrane. Although various models of peritoneal membrane have been proposed, the 3-pore model is most widely accepted to explain solute and water transport across the peritoneum. It assumes the capillary endothelium to be the major barrier to solute and water transport, which ensues through a system of pores that are classified into 3 broad categories, ultrasmall, small, and large pores. The abundant small pores (40 to 60 Å radii) are the tortuous intercellular clefts between the endothelial cells. They are responsible for small solute transport. The ultrasmall pores (radius 3 to 5 Å), also present in large number, are probably the transendothelial aquaporin-1. Solute free water transport occurs across them. In addition, a few large pores (200 to 300 Å radii) are present. The nature of the large pores is not well known. Macromolecules like albumin are transported across them.
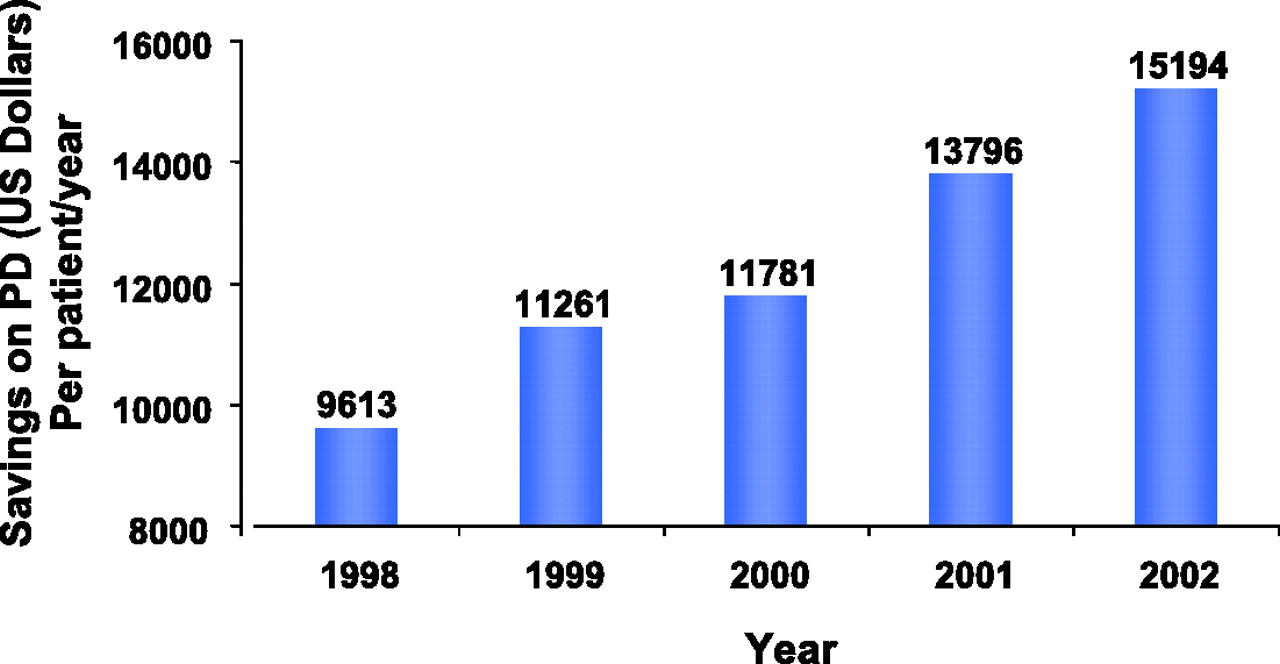
- Figure 5.
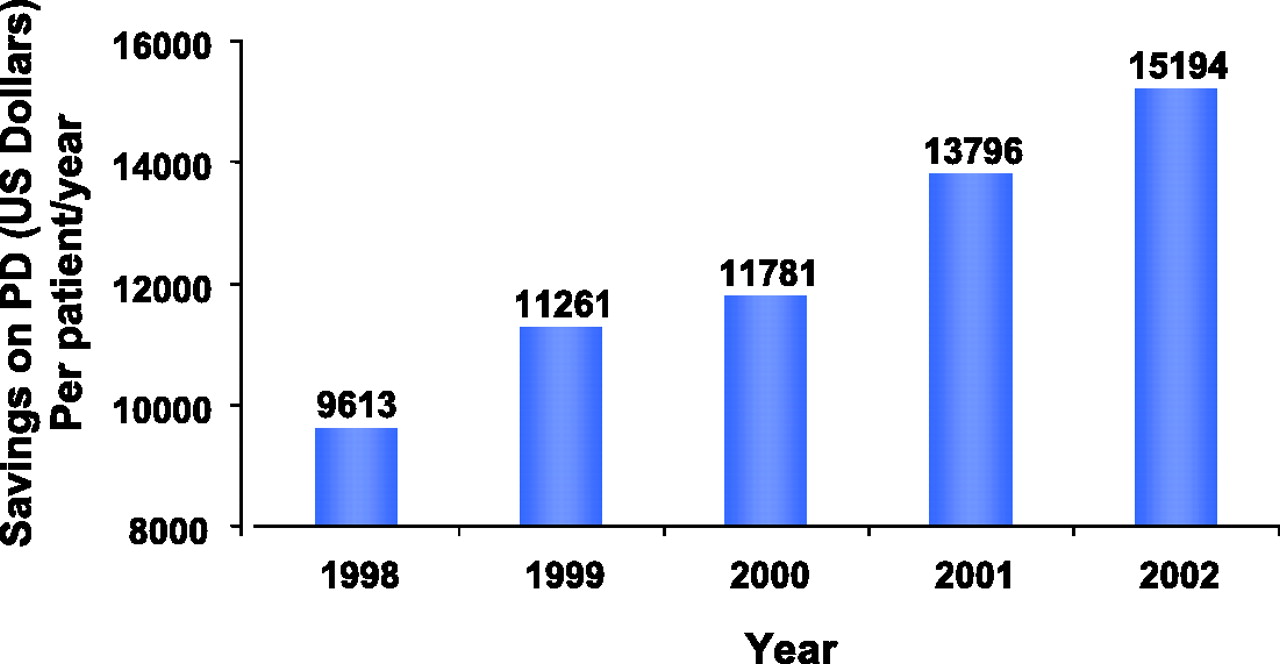
Cost savings on peritoneal dialysis (PD). Medicare savings on PD per patient per year have progressively increased over the years.11
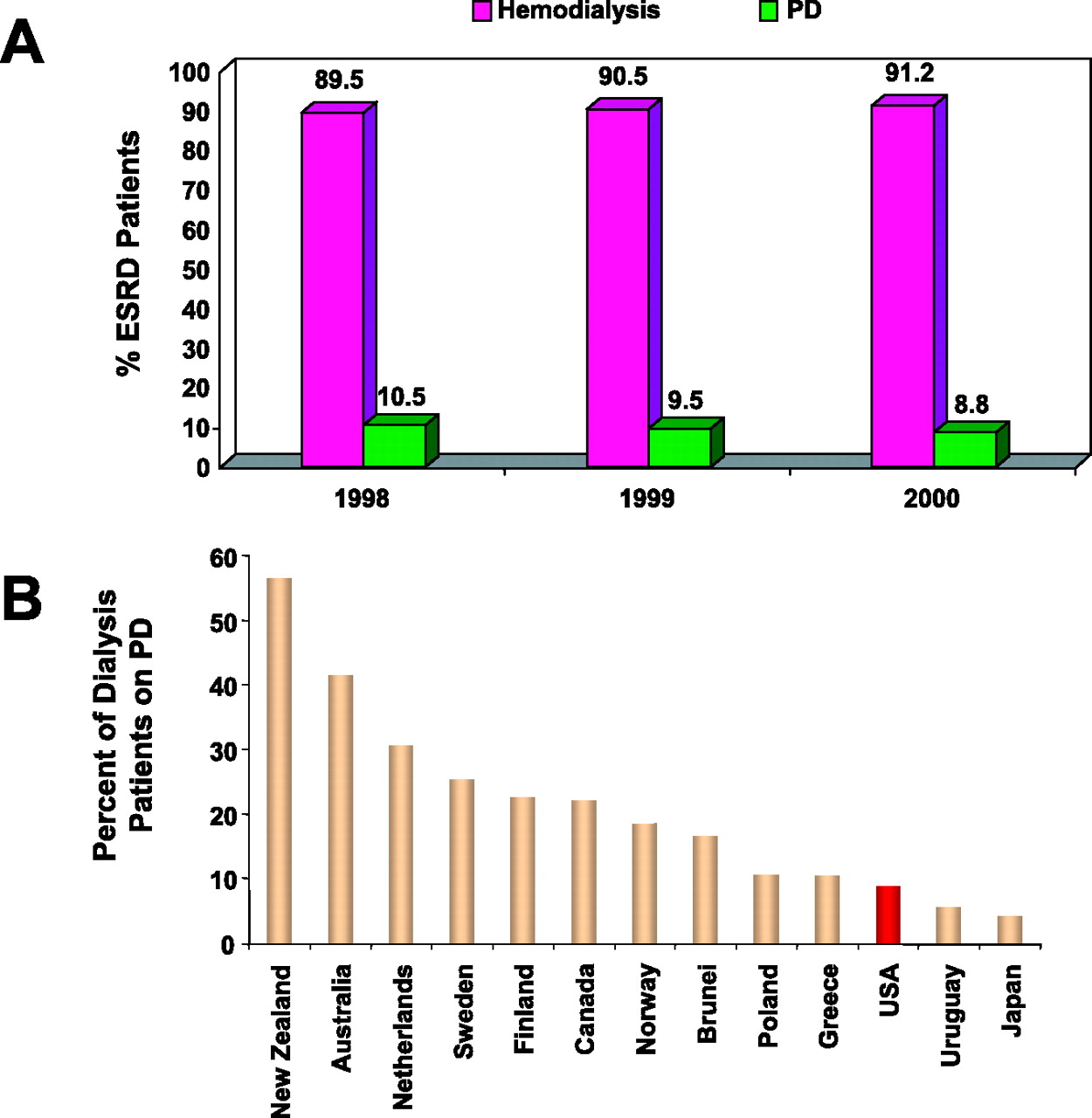
- Figure 6.
Utilization of peritoneal dialysis (PD) in various countries. Whereas PD is being used less and less in the United States with only 8.8% of dialysis patients receiving PD in 2000 (A), a much larger proportion of dialysis patients receive PD in most developed countries across the globe (B).



Tables
Absolute Peritoneal adhesions Encapsulating peritoneal sclerosis Pleuro-peritoneal leak Relative (major) Psychosis* Mental retardation* Quadreplegia/ hemiplegia* Other physical handicap* Blindness Colostomy/gastrostomy Poor motivation Relative (minor) Obesity Hernia Polycystic kidneys Low back problems * Will need assistance. Contraindicated for self-treatment.
Conventional Icodextrin Dextrose (g/dL) 1.5, 2.5, 4.25 0 Icodextrin (g/dL) 0 7.5 Sodium (mmol/L) 132.0 132.0 Chloride (mmol/L) 102.0 96.0 Calcium (mEq/L) 2.5 to 3.5 3.5 Magnesium (mEq/L) 0.5 to 1.5 0.5 Lactate (mEq/L) 40.0 40.0 Bicarbonate (mmol/L) 0 0 Osmolality (mOsm/kg) 346 to 485 282 to 286 pH 5.2 5.2 Pros Lower cost than hemodialysis (HD) Patients more satisfied with overall care compared with HD Steady-state treatment. Better tolerated hemodynamically Flexible schedules Needleless Preservation of vascular sites for future hemodialysis Lower risk of blood-borne infections12,13 Alleviates anxiety from needle sticks Better preservation of residual renal function Fewer diet and fluid restrictions Cons Continuous therapy. No days off. Leads to patient and family burnout Body image concerns because of presence of catheter and fluid in the abdomen High technique failure rate compared with HD Space needed for monthly supplies of dialysis equipment/solutions Inability to lift >25 lbs. Non-compliance with dialysis can lead to complications such as infections, uremia, and technique failure Infections Peritonitis Tunnel infections Exit site infections Associated with increased intra-abdominal pressure Hernia Abdominal wall edema Scrotal/vulvar edema/hydrocele Hydrothorax Mechanical Catheter leakage Catheter tip migration Inadequate drainage Metabolic Hyperglycemia Hyperlipidemia Obesity Protein loss Hypokalemia Hypomagnesemia Miscellaneous Encapsulating peritoneal sclerosis Eosinophilic peritonitis Condition Drug Adult Dose Prophylactic regimen for dental, oral, or upper respiratory procedures Standard regimen Amoxicillin 2 g orally (po, per os) 1 hour before procedure Penicillin allergy Clindamycin, Cephalexin, Cefadroxil, Azithromycin, or Clarithromycin 600 mg po 1 hour before procedure; 2 g po 1 hour before procedure; 500 mg po 1 hour before procedure Patients unable to take oral medication Ampicillin 2 g IV/IM 30 minutes before procedure Penicillin allergy and cannot take oral medications Clindamycin or Cefazolin 600 mg IV 30 minutes before procedure; 1 g IV/IM 30 minutes before procedure Prophylactic regimen for genitourinary/gastrointestinal (excluding esophageal) procedures Standard regimen Ampicillin and Gentamycin plus Amoxicillin or Ampicillin 2 g IM/IV 30 minutes before procedure; 1.5 mg/kg (maximum 120 mg) IM/IV 30 minutes before procedure; 1 g po 6 hours after the initial dose; 1 g IM/IV 6 hours after the initial dose Patients allergic to penicillins Vancomycin Plus gentamycin 1 g IV over 1 to 2 hours completing within 30 minutes of the starting procedure; 1.5 mg/kg (maximum 120 mg) IM/IV 30 minutes before procedure IV, intravenously; IM, intramuscularly.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}