
Article Figures & Data
Figures
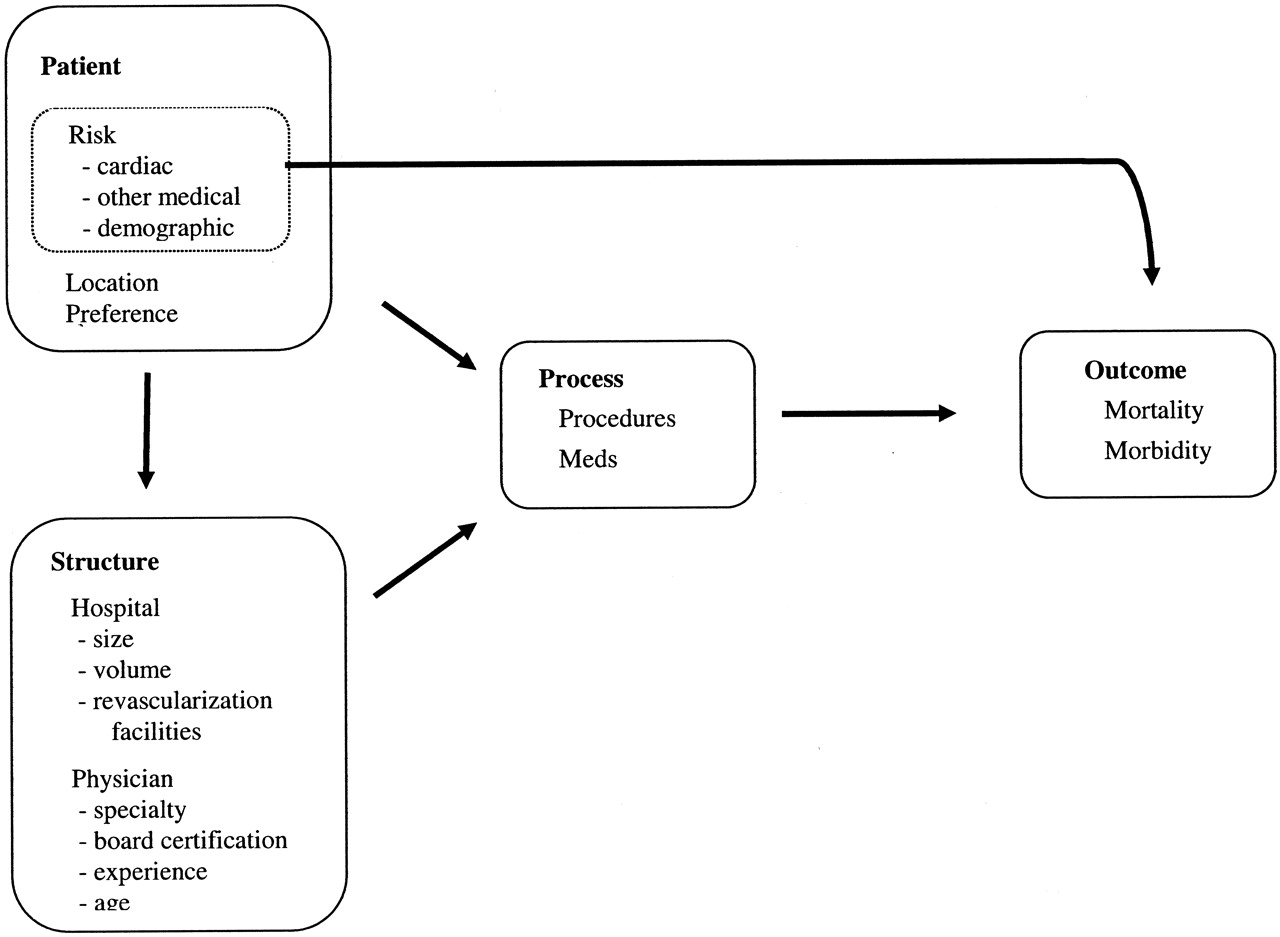
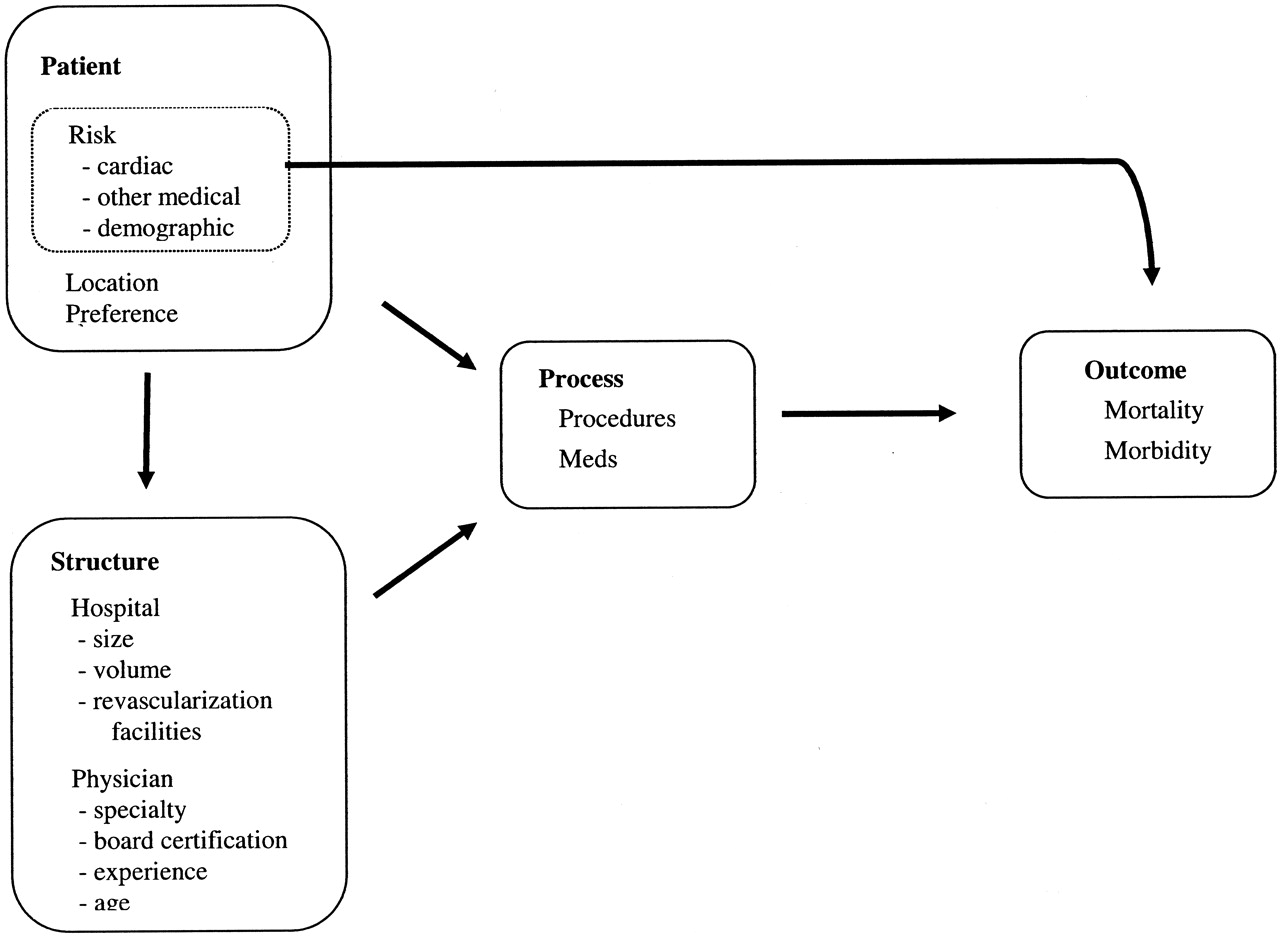
- Figure 1.
Model of Factors Influencing Patient Outcomes
Tables
Author and Year Study Site/Design/Duration Sample Size Inclusion Criteria Exclusion Criteria Physician Characteristics Data Abstracted from the Records Factors Controlled Chen 2000 USA except the following states: AL, IA, WI, and MN/retrospective chart review/1994–1995/109,243 patients Medicare beneficiaries discharged from the hospital with a diagnosis of MI and chart documentation of either a serum creatine kinase MB index >5%, serum LDH level more than 1.5 times the upper limit of the normal value, or 2 of the 3 following criteria: chest pain, serum creatinine level twice the hospitals normal value, EKG evidence of MI. Transfer patients (18.0%) Subsequent hospitalization for MI. Those treated by physicians of other specialties, self-declared specialists (not confirmed Board Certified) Patients with terminal illness Missing data Cardiologists Medical subspecialty General Internists Family practice General practice Confirmed Board Certification Demographics, clinical history, presenting symptoms, use of medications, treatments, procedures, hospital course, vital status. Dates of death (30 day and 1 year mortality) Age, systolic BP, Killip class, heart rate, infarct location, previous MI, previous bypass surgery, height, weight, DM, smoking status, HT, cerebrovascular disease.Hospital factors: onsite availability of coronary angiography, angioplasty, bypass surgery, location of hospital, ownership status of hospital, teaching status,Inability to ambulate, urinary incontinence, dementia, admission for nursing home, chronic obstructive pulmonary disease, peripheral vascular disease, liver disease, HIV, or other immunological compromise, trauma within the previous month, serum urea nitrogen level >40 mg/dL, serum creatinine level >20 mg/dL, serum albumin level <3 mg/dL, hematocrit <30%. Dummy variables were included for missing values. Frances 2000 USA/retrospective cohort/April 1994 to July 1995/210,996 identified from the Medicare beneficiaries final sample size: 161,558 Creatine kinase MB index ≥5% or an elevated LDH level with LDH-1 ≥ LDH-2, or 2 of 3 criteria: chest pain, creatine kinase ≥ twice the normal value and EKG evidence of AMI. Only first visits were included. Transfer patients (6.7%) Patients who lacked a confirmed diagnosis of AMI, records not indicating the treating physician, geographical location of their homes CardiologistNon-cardiologistsBased on UPIN and self-report Pri.: 30 day and 1 year mortality rates, Sec.: treatment decisions.Med. outcomes: in hospital treatment with thrombolytic therapy, aspirin, beta-blockers, ACE inhibitors, calcium channel blockers.Procedure outcomes: coronary angiography, PTCA, CABG during hospitalization Demographics, geographic variables, comorbidity, severity variables, hospital volumes variables. Norcini 2000 Pennsylvania/retrospective chart review/during 1993/28,756 patients Patients who were admitted directly to a hospital for MI (as opposed to those transferred from another acute care hospital) Transfer patients (20.4%). Patients with “clinical complexity” (cancer, transplant, etc), patients who left the hospital against medical advice, patients of physicians who treated more than 100 patients, patients treated by specialties other than cardiology or primary care, and patients treated at a hospital that closed since 1993 or at a hospital that treated <30 AMI patients in 1993 Cardiologist, Family Medicine and Internal Medicine Based on AMA master file of Board Certification, years of experience since medical school. Age, gender, cardiac dysrhythmias, cardiogenic shock, cardiomyopathy, conduction disorders, diabetes, dialysis, heart failure, HTN, infarct site, payer, prior CABG, renal failure Probability of death, availability of advanced cardiac care, hospital location, physician volume, number of years since physician graduated from medical school, physician certification Frances (Arch) 1999 California/retrospective chart review/April 1994-July 1995/7663 patients Medicare beneficiaries 65 years and older who had a diagnosis of MI confirmed by either chart review and required a creatine kinase MB index above 0.05 or elevated LDH level with LDH-1 > LDH-2, or 2 of the following criteria: chest pain, creatine kinase MB level at least 2-fold greater than normal, or evidence of AMI on EKG. Transfer patients (17.2%), those with missing data. Cardiologist, medical sub-specialists, internists, family practitioners Based on UPIN and self-report Thrombolytic therapy, aspirin during hospitalization, β adrenergic blocking drugs, ACE inhibitors, calcium channel blockers, at hospitals and at discharge, exercise stress test, EKG, coronary angiography, revascularization procedures, mortality during 1 year. Patient demographics, comorbidity, severity of illness characteristics on admission, hospital characteristics including volume of admissions for AMI and the availability of revascularization principles Casale 1998 Pennsylvania during 1993/retrospective chart review/30,205 patients Patients who were admitted directly to a hospital for MI (not those transferred from another acute care hospital) Transfer patients (23%) Under 30 years or over 99 years of age, patients who left the hospital against medical advice, patient with “clinical complexity”(cancer, transplant, etc.) patients of physicians who treated >100 patients, patients treated by specialties other than cardiology or primary care and patients treated at a hospital that closed since 1993 or at a hospital that treated <30 AMI patients in 1993 Cardiologist Primary care Based on self-report Age, gender, infarct location, Prior CABG<cardiac dysrhythmia, cardiogenic shock, diabetes, cardiomyopathy, conduction disorder, dialysis, renal failure.Patient race not identified Age, gender, infarct location, Prior CABG<cardiac dysrhythmia, cardiogenic shock, diabetes, cardiomyopathy, conduction disorder, dialysis, renal failure Ayanian 1997 Texas USA/retrospective chart review of Medicare provider analysis.February and May 19902087 eligible.1837 records available. Patients who underwent coronary angiography within 90 days of initial hospitalization and a random sample of those who did not undergo angiography. Patients hospitalized during the previous year with a principal diagnosis of acute myocardial infarction, enrolled in HMO, discharged alive in less than 5 days, transferred to another hospital within 2 days without a principal diagnosis of AMI at the receiving hospital Attending cardiologists Attending generalist Attending generalist with cardiology consultation Based on self-report Initial hospitals and contiguous transfers to other hospitals, presenting symptoms and vital signs, coexisting illnesses, mobility, results of laboratory tests, EKG findings, major complications, use of cardiac drugs and procedures, mortality rates at 30 days and 1 year after admission. Date of death if applicable Age, gender, type of infarct, h/o hypertension, heart failure, angina pectoris, diabetes, initial heart rate and systolic BP, impaired mobility and initial creatinine level. History of stroke and time of onset of chest pain until presentation. Hospital characteristics. Jollis 1996 4 states in USA/retrospective chart review/June–December 1992/8241 Medicare beneficiaries Patients who had a confirmed diagnosis of AMI (criteria for diagnosis of an AMI similar to previous studies) Subsequent hospitalization for MI. Transferred patients included in analysis but number not listed (assigned to first hospital) Cardiology, Internal medicine, Family medicine, General practice, other or unknown Based on UPIN and self-report Age, systolic BP at admission, pulse, location of MI, Killip class, height, weight, h/o infarction, h/o bypass surgery, smoking status, presence or absence of DM, HT, cerebrovascular disease, hospital characteristics, urban or rural site, Charlson comorbidity score Age Rural Patients (%) Heart Failure (%) Dementia (%) COPD (%) Revascular Hospital (%) Impaired Mobility (%) Chen et al 5 Cardiologists (35%)* 75.3 9† 17 3 16 51 13 Family physicians 77.5 42† 24 8 22 21 23 Frances et al7 Cardiologists (38%)* 73.7 28.3 18.0 3.4 18.6 80.1 17.4 Non-cardiologist 76.6 28.2 26.0 8.8 23.4 55.3 28.0 Norcini et al18 Cardiologists (30%)* 66.1 29.4 41.5 Family physicians 69.2 35.2 23.4 Frances et al23 Cardiologists (50%)* 76.6 4.0 19.5 4.5 18.0 75.6 14.2 Family physicians 78.5 11.1 27.7 12.0 23.2 53.7 26.0 Casale et al10 Cardiologists (37%)* 66.1 10.8† 41.2 Family physicians 70.0 26.7† 25.0 Ayanian et al6 Cardiologists (36%)* 71.3 32.4 72.8 7.4 Generalists 72.0 31.8 34.9 11.4 Jollis et al22 Cardiologists (26%)* 75.0 10.9† 59.3 Family physicians 77.0 53.3† 39.7 * Percentage of patients treated by cardiologist.
† Rural measured by location of hospital.
Demographic factors ↑ age,7,12,14,18–20 ↑ female,7,12,14,18–20 ↑ minority,12,19 ↑ Medicare,7,14 ↓ commercial insurance7,14 Clinical factors Cardiac ↑ New York Heart Association Class (worse),12,19 ↑ Killip Class,12,18 ↑ tachycardia,12,19 ↓ prior myocardial infarction,12,18,19 ↑ prior congestive heart failure,7,12,14,19,20 ↓ cardiogenic shock,7,14 Non-cardiac ↓ cardiac arrest on admission,12,19 ↓ CABG, and ↓ angioplasty,7,12,14,19 ↑ GUSTO predicted mortality18,19 ↑ Prior hypertension,12,19 ↑ admission from nursing home,12 ↓ mobility,12,19,20 ↑ incontinence,12 ↑ prior stroke,12,18,19 ↑ diabetes,12,18–20 ↑ depression,19 ↑ dementia,12 ↑ renal,12,19,20 ↑ liver,12,19 ↑ obstructive lung disease,12,19 ↑ anemia,12,19 ↑ (DNR or terminal patients),12,19 ↓ ideal candidate for intervention12,19 ↑ admission severity score7,14 Health system:(Hospitals) ↓ size,19 ↓ MI volume,7,12,19 ↓ cardiac resources,12,18,19 ↑ rural,7,12,14,18,19 ↑ public,12 ↓ major teaching hospitals12 * Arrows indicate that the increase (↑) or decrease (↓) of patient or hospital variables for generalists relative to cardiologists is statistically significant.
Study Reasons Confounding May Be Less Reasons Confounding May Be Greater Chen et al5 Good measures of comorbidities and functional status. Eliminated patients with terminal illness. Compared board certified physicians. Francis et al7 Instrumental variable related to hospital distance was used to reduce confounding. Strong confounding of physician type with patient age. Norcini et al18 Excellent assessment of comorbidities. No information on functional status or race. Strong confounding of physician type with patient age. Frances et al23 Good measures of comorbidities and functional status. Generalists patients have very high risk. Patient location not assessed. Nash et al9 Analyzed patients in two age strata. Adjusted for some demographic variables using propensity score. No information on functional status or race. Casale et al10 Excellent assessment of comorbidities. No information on functional status or race. Strong confounding of physician type with patient age. Ayanian et al6 Excluded patients 80 or older. No information on functional status or race. Nash et al13 No information on functional status or race. Jollis et al22 No comorbidity or functional status. Study 30-day or In-hospital Rates 1 year MR (%) OR ORadj MR (%) OR ORadj Chen et al Card* 16.1 1.00 1.00 26.8 1.00 1.00 Spec 20.2 1.32† 0.98 36.9 1.60† 1.05 IM 19.2 1.24† 0.99 33.6 1.38† 1.03 FP 19.7 1.28† 0.96 34.4 1.43† 1.01 GP 22.2 1.49† 1.06 37.0 1.60† 1.08 Frances et al7 Card* 1.00 1.00 1.00 1.00 NC 1.30† 1.04† 1.37† 1.10† NC (IV) 1.10 1.06 Norcini et al18‡ Card* 8.5 1.00 1.00 IM 11.9 1.45† 1.25† FP 10.8 1.30† 1.25† Frances et al23 Card* 18.9 1.00 1.00 31.3 1.00 1.00 Spec 25.6 1.48† 1.25† 46.5 1.91† 1.20† IM 21.0 1.14† 1.25† 43.0 1.66† 1.11† FP 21.7 1.19† 1.11† 43.0 1.66† 1.30† Nash et al9‡ age <65 Card* 4.1 1.00 1.00 Generalists 4.3 1.05 0.95 Nash et al9‡ age >65 (in hospital rates) Card* 13.7 1.00 1.00 Generalists 16.8 1.27 1.22 Casale et al10‡ Card* 8.5 1.00 1.00 Gen 11.8 1.44† 1.20† Nash et al13‡ 1.00 Card* 7.9 1.00 1.26† IM 12.0 1.59 1.29† FP 11.1 1.44 Ayanian et al6 Card* 16.6 1.00 1.00 24.4 1.00 1.00 Gen 20.8 1.32† 1.06 29.5 1.30† 0.99 Jollis et al22 Card* 15.7 1.00 1.00 27.3 1.00 1.00 IM 20.3 1.37† NR 34.0 1.37† 1.14† FP 20.4 1.38† NR 34.7 1.42† 1.11† GP 22.1 1.52† NR 36.1 1.50† 1.20† Uk 24.7 1.76† NR 36.9 1.56† 1.32† * Reference group. Odds ratios are 1.00 because cardiologists are the reference group.
† Significant at P < .01.
‡ Studies reported mortality rates in the hospital rather than 30 day. MR, mortality rate; OR, odds ratios of cardiologist compared with other specialties; ORadj, adjusted odds ratio; Card, cardiologists; Spec, internal medicine subspecialist not in cardiology,; IM, general internist; FP, family physician; GP, general practice; N-C, non-cardiologists; NC (IV), noncardiologist adjusting for instrumental variable; NR, not reported; Uk, unknown.




{kind=link}
Jump to section
Related Articles
Cited By...
- The Paradox of Primary Care
- The Medical Home: Growing Evidence to Support a New Approach to Primary Care
- North American Primary Care Research Group President's Award
- Interpersonal continuity: old and new perspectives
- Myocardial Infarction Mortality in Rural and Urban Hospitals: Rethinking Measures of Quality of Care