
Abstract
Objective: To describe coexisting medical conditions and lifestyle factors associated with asymptomatic peripheral arterial disease (PAD) in a population of white, African American, and Hispanic patients.
Study Design and Setting: White, African American, and Hispanic patients 50 years or older were recruited for this cross-sectional study from 4 primary care clinics in Houston, TX. Patients with an ankle-brachial index (ABI) < 0.9 and without leg symptoms typical of PAD were diagnosed with asymptomatic PAD.
Results: 403 patients were screened for PAD. Of these, 25 (6.2%) had asymptomatic PAD. Compared with patients without PAD, diabetes mellitus ([OR] 3.8; 95% CI 1.6, 9.0) and a history of smoking at least 1 pack of cigarettes per day ([OR] 2.5; 95% CI 1.1, 6.0) were significantly associated with asymptomatic PAD. An interaction effect existed between diabetes mellitus and smoking at least 1 pack of cigarettes per day. Diabetes mellitus combined with heavy smoking showed the highest predicted value positive (15%) and the highest specificity (92%). A lack of both demonstrated low rates for predicting asymptomatic PAD (predicted value positive, 1%).
Conclusion: The ankle-brachial index could become routine screening among patients with diabetes mellitus and/or who smoke.
Among patients aged 50 years and older, the prevalence of peripheral arterial disease (PAD) for both symptomatic and asymptomatic patients is 12% to 19%.1–4 Previous research has outlined risk factors associated with PAD, which include diabetes mellitus, hypertension, older age, and dyslipidemia.1–17 A higher prevalence of PAD has also been found among older African Americans and Hispanics when compared with whites.11,12
Research has shown that 53.8% of patients with PAD within a general medicine practice are asymptomatic.13 The inadequate recognition of PAD may place many patients at risk of its complications, including ischemic ulceration, gangrene, limb loss, and/or increased cardiovascular morbidity and mortality.5,14 As Hirsch demonstrated in a large study in 2001, the under-utilization of early screening and diagnosis of PAD could be a barrier to preventing further cardiovascular risk.18 Increasing physicians’ awareness of the importance of screening patients at high risk for PAD has important benefits. Patients treated early for PAD could have a significantly improved quality of life as well as the decreased likelihood of future cardiovascular morbidity and mortality.
The purpose of this study was to describe coexisting medical conditions and lifestyle factors associated with asymptomatic PAD in a population of white, African American, and English- and Spanish-speaking Hispanic patients attending a primary care clinic.
Methods
This study was based on a subgroup analysis of a previously identified PAD cohort. Data were collected as part of a cross-sectional study on the epidemiology of PAD among whites, African Americans, and English- and Spanish-speaking Hispanics. It obtained equal representation of 3 ethnic groups to assess the prevalence of PAD by race. The study took place between September 2000 and August 2001 and was approved by the Institutional Review Board for Human Subjects Research for Baylor College of Medicine and Affiliated Hospitals and by the Department of Veterans Affairs (VA) Research and Development Committee. Written informed consent was obtained from all patients.
Study Population
All patients attended one of 4 primary care clinics in Houston, TX: Martin Luther King Clinic, the primary care clinics at the Michael E. DeBakey Veterans Medical Center (formerly the Houston VA Medical Center), and the primary care clinics at Ben Taub Hospital (later to be replaced by Gulfgate Clinic because of feasibility of recruitment). Martin Luther King Clinic, Ben Taub Hospital, and Gulfgate Clinic were affiliated with the Harris County Hospital District (HCHD) and served lower income patients from racially diverse backgrounds. Patients who identified their ethnicity as non-Hispanic white, African American, or Hispanic were recruited. Both English- and Spanish-speaking Hispanics were eligible for participation in the study. Subjects were consecutively identified using patient appointment lists and were then telephoned at home or approached in the clinic. A research assistant determined further eligibility for the study, and patients gave informed consent for study participation.
Exclusion Criteria
The study initially included all men and women older than 50 years. However, after finding no patients with an ankle-brachial index (ABI) of less than 0.90 between the ages of 50 and 54, the recruitment age was increased to 55 years and older. Those patients aged 50 to 54 years were not excluded from the analyses. Patients unable to read or speak English or Spanish were excluded. Patients were also excluded if there was a history of dementia, chronic obstructive pulmonary disease requiring oxygen, a malignancy other than skin (with a probability of survival of less than 6 months or with a recent diagnosis), leg ulcers or gangrene, or a lower extremity amputation. Patients were also excluded from participating if they were unable to provide a contact telephone number or if they resided outside of Texas. Patients with symptomatic PAD were excluded from the analysis, so that characteristics solely associated with asymptomatic disease could be determined.
Data Collection Techniques and Instruments
Ankle-Brachial Index
The ABI is the ratio of the systolic blood pressure in the ankle to that in the arm. The ABI measurement was obtained by a research assistant trained at the Houston VA Medical Center vascular laboratory. The ABI and questionnaires were performed in the clinic room before the patient’s scheduled appointment with the physician. The patient was asked to lay supine for 5 minutes before the ABI was measured, to assure an accurate blood pressure reading. Blood pressure cuffs were placed on the arms and ankles, and the pulse was detected with an ultrasound Doppler. The systolic pressure was taken in the arm and the dorsalis pedis (DP) and posterior tibialis (PT) pulse of the ankle. The pressures were always taken in the following order: right arm, right DP, right PT, left PT, left DP, left arm. The higher of the DP and PT measurements in each ankle was taken again and recorded. The highest arm systolic pressure was remeasured if it was at least 10 mm Hg higher than the systolic pressure in the other arm. To calculate the ABI, the average of the 2 highest of the 3 pressures taken in the ankle was divided by the average of the arm systolic pressures (or the average of the highest 2 if a third pressure was taken). A patient with an ABI of <0.9 was classified as having PAD, as many studies have found that a ratio of ≤0.90 signifies the presence of PAD.19–24
San Diego Claudication Questionnaire
The San Diego Claudication Questionnaire (SDCQ), a self-administered questionnaire developed by Criqui et al,1 was given to determine classic intermittent claudication, atypical leg symptoms, or no leg symptoms. Within this study, we defined asymptomatic PAD as patients with an ABI of <0.9 and no leg symptoms per the SDCQ.
Lifestyle and Clinical Survey
The Lifestyle and Clinical Survey was developed and validated by Dr. Tracie Collins, the principal investigator on the study.25 It involved 88 items that identified patient sociodemographics, a history of heart failure, hypertension, diabetes, medication use, and social habits (eg, smoking, physical activity). The survey required approximately 10 minutes to administer.
Statistical Analysis
The χ2 for dichotomous variables determined significant univariate associations. The dependent variable was the presence of asymptomatic PAD, and the independent variable was the medical condition or lifestyle factor in question. Multivariate logistic regression determined the association between the independent variables and asymptomatic PAD.
The following independent variables were included in a logistic regression model: race (white, African American, or Hispanic); age (continuous); if the patient reported that their physician had ever diagnosed them with hypertension, congestive heart failure, and/or diabetes mellitus (yes/no); if the patient currently consumed alcoholic beverages (yes/no); if the patient did consume alcohol, how often he or she consumed alcohol (rarely/occasionally or daily/weekly); if the patient smoked at least 100 cigarettes in his or her lifetime (yes/no); if the patient smoked 100 cigarettes in his or her lifetime, then the average number of cigarettes the patient smoked per day (less than 1 pack per day, at least 1 pack per day); the number of years the patient smoked on average in his or her lifetime (0 years, less than 1 year to 40 years, greater than 40 years); how often the patient walked for at least 10 minutes without stopping (rarely or never, 1 time per week, more than 1 time per week). All analyses were performed using SAS 6.0 for PC and SAS 8 for UNIX.
Results
457 patients were approached for study participation, and 403 agreed to participate. According to the SDCQ, 212 patients experienced leg symptoms on exertion and 191 were asymptomatic. Of the 403, 62 patients (15%) had a measured ABI <0.9. Of those with PAD, 25 (40%) were asymptomatic. Ultimately, 6.2% of patients screened in the primary care clinics had asymptomatic PAD.
General characteristics of the study population are presented in Table 1. Of the 25 patients with PAD, 36% were white, 36% were African American, 28% were Hispanic, and 40% were female. The mean age of the entire cohort was 63.6 years (SD, 7.24). This study found that asymptomatic PAD did not differ in prevalence by race.
General Characteristics of the Study Population
Hypertension was reported in 80% of patients with asymptomatic PAD and in 66% of the patients without PAD (P > .05). Congestive heart failure was reported in 12% of patients with asymptomatic PAD versus 5% of patients without PAD (P > .05). The prevalence of diabetes mellitus was significantly higher in patients with asymptomatic PAD when compared with patients without PAD (64% vs. 34%, respectively; P < .05).
Questions and results from the Lifestyle and Clinical Survey are presented in Table 2. A majority of both groups smoked at least 100 cigarettes in their lifetimes (54% vs. 60%). Compared with those who did not smoke, patients who smoked more than one pack of cigarettes per day showed a significantly higher association with asymptomatic PAD (P = .03). Rates did not differ significantly for number of years a patient regularly smoked (P > .05).
Lifestyle and Clinical Survey
A majority of patients in both groups did not consume alcohol, and trended toward statistical significance (65% without PAD vs. 84% with asymptomatic PAD, P = .05). How often patients consumed alcohol did not differ significantly by the presence or absence of asymptomatic PAD (P > .05). More patients with asymptomatic PAD rarely or never walked for at least 10 minutes without stopping (48% vs. 28%, P > .05). The majority of patients in both groups walk at least once a week or more (52% vs. 72%).
After adjusting for age and gender, diabetes mellitus and smoking at least 1 pack of cigarettes per day were significantly associated with asymptomatic PAD when compared with those without PAD. Patients with diabetes mellitus were 3.8 times (95% CI 1.6, 9.0) more likely to have asymptomatic PAD than patients without diabetes mellitus. Patients who smoked at least 1 pack of cigarettes per day were 2.5 times (95% CI 1.1, 6.0) more likely to have asymptomatic PAD than patients who did not smoke at least 1 pack of cigarettes per day.
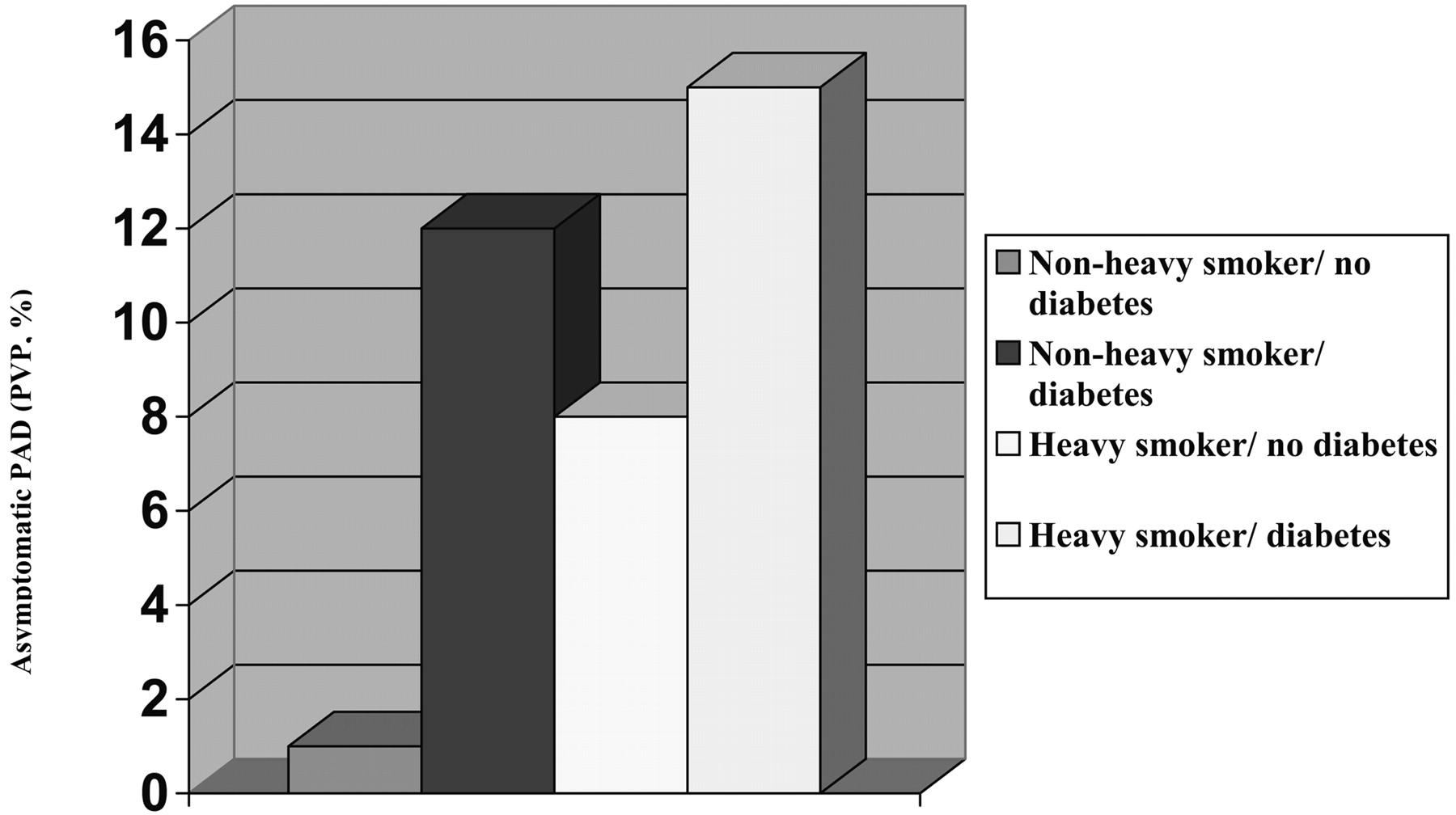
Because diabetes mellitus and smoking at least 1 pack of cigarettes per day demonstrated the strongest associations with asymptomatic PAD, these factors were further examined to determine the presence of an interaction effect. Table 3 presents the sensitivities, specificities, and predicted values of diabetes mellitus and smoking as predictors of asymptomatic PAD. When examined individually, diabetes mellitus predicted asymptomatic PAD more sensitively than heavy smoking (64%), and diabetes mellitus combined with heavy smoking demonstrated the highest positive predicted value (15%) and the highest specificity (92%). Not having diabetes mellitus combined with smoking less than a pack of cigarettes per day showed extremely low rates for predicting asymptomatic PAD (positive predicted value, 1%). Figure 1 graphically presents the positive predicted values of diabetes mellitus and smoking with asymptomatic PAD. An interaction effect of diabetes mellitus and heavy smoking seems to exist in predicting asymptomatic PAD.
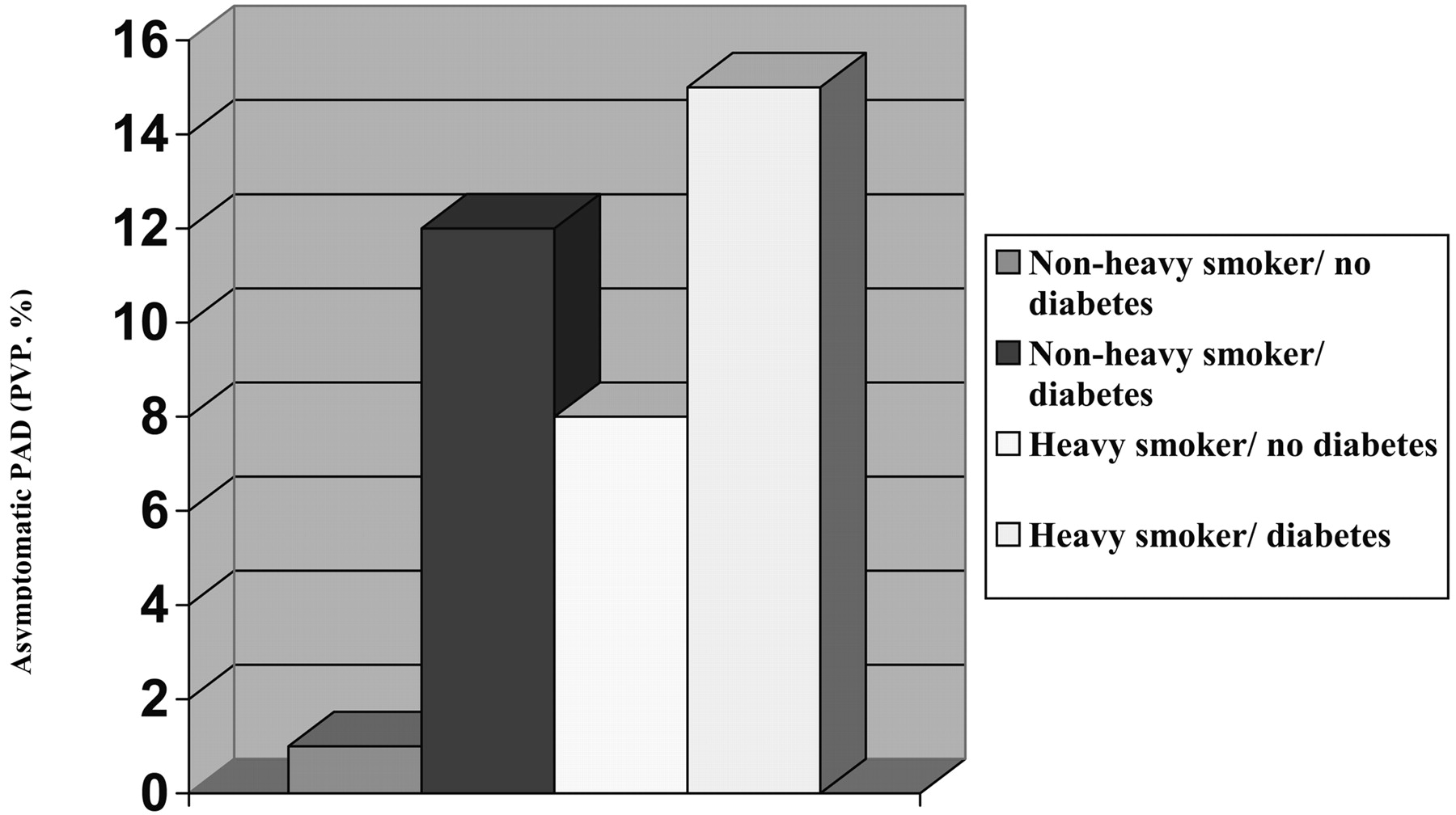
Individual and synergistic associations of diabetes and heavy smoking with asymptomatic PAD.
Predicting Asymptomatic PAD*
Discussion
This study found a 6.2% prevalence of asymptomatic PAD in a racially diverse population attending a primary care clinic. Patients with a history of diabetes mellitus and smoking at least one pack of cigarettes per day were more likely to have asymptomatic PAD. These results are comparable with those of previous studies on both symptomatic and asymptomatic PAD.9,15,19 These results build on previous ones by demonstrating the additive effects of risk factors that are associated with asymptomatic PAD—potentially highlighting criteria for screening.
The complications of diabetes mellitus vary widely, including PAD as one of many problems that can result. A cross-sectional study performed by Walters et al20 found an 8.7% prevalence of PAD among patients with type I diabetes mellitus and a 23.5% prevalence of PAD among patients with type 2 diabetes mellitus. Regardless of the high prevalence and complications that can result from PAD, it is not yet common practice to routinely screen for the disease in patients with diabetes mellitus. Examining the results of this study and those of previous studies, perhaps the ABI should be part of a routine doctor’s office visit for patients with diabetes mellitus.
A multitude of research has agreed on the strong association between cigarette smoking and PAD.2,13,15,19,26 Previously it has been found that current smoking status has a greater effect on PAD than a lifetime history of smoking, because it has been shown that smoking cessation significantly reduces cardiovascular complications.27–31 As this study focused on the patient’s lifetime smoking history, it can only be inferred from our results that a history of heavy smoking is associated with asymptomatic PAD.
In our experience, general medical practices typically do not measure the ABI unless a patient begins to exhibit symptoms of the disease. Previous research has found that regardless of the presence or absence of symptoms, PAD can be reliably diagnosed with the ABI. Newman et al13 examined the association between ABI values and different leg symptoms associated with PAD. Looking at ABI measurements in increments of 0.10, the findings suggested that asymptomatic cases of PAD predominated over symptomatic cases. In general, asymptomatic disease decreased in prevalence as ABI values decreased; the highest prevalence of a lack of symptoms existed in the “borderline” cases with an ABI of 0.80 to <0.90.
Research by McDermott et al32 has demonstrated a significant association between impaired lower extremity functioning and asymptomatic PAD. It is possible that functional limitations resulting from poor health could lead to a decrease in physical activity and therefore prevent the symptoms of PAD from occurring. Examining the significant factors associated with asymptomatic PAD in this study and those of previous ones, it can be theorized that screenings among patients who exhibit a risk for PAD could lead to an early detection of the disease, before any symptoms have appeared. This could alert the patient to modify these risk factors and prevent a further progression of the disease to a more serious case.
This study had some limitations. First, the small sample size of 25 patients with asymptomatic PAD could have led to the insignificant results of the other independent variables found in previous studies to have an association with PAD, such as race/ethnicity, older age, male gender, and history of congestive heart failure and/or hypertension. In addition, a misclassification of leg symptoms could have also occurred. Some patients previously experiencing leg pain on exertion could have limited their physical activity and been misclassified as asymptomatic. Because nearly half the patients (48%) with asymptomatic PAD rarely or never walked outside for at least 10 minutes without stopping, this could have prevented the manifestation of symptoms, which may not have appeared until much later in the progression of the disease and therefore put the patient at a higher risk for cardiovascular events. Another form of misclassification bias could have been in the recording of the ABI. Calcified arteries, resulting as a complication of diabetes mellitus, could have resulted in a falsely elevated ABI and therefore could have prevented a PAD diagnosis in a patient with diabetes mellitus.33,34
Further research should determine whether the control of diabetes mellitus and/or smoking diminishes the prevalence of asymptomatic PAD in older patients attending a primary care clinic. Several studies have already examined the effects of smoking cessation interventions on patients with symptomatic PAD and have shown that smoking cessation reduces rest pain associated with PAD, decreases the prevalence of myocardial infarction and cardiac death, and increases survival rates.29–33 Determining if smoking cessation prevents progression of asymptomatic PAD to intermittent claudication and its subsequent complications might justify the need to screen heavy smokers for PAD.
Further research should look at the effectiveness of screening for PAD in reducing cardiovascular morbidity and mortality. As the population ages, PAD will increase in prevalence, particularly asymptomatic PAD. By examining the effectiveness of ABI and its use with patients at higher risk for PAD, disease may be diagnosed earlier and strategies could be used to delay the progression of the disease and prevent complications.
Notes
Funding: This material is the result of work supported with resources and the use of facilities at the Houston Center for Quality of Care and Utilization Studies, Houston Veterans Affairs Medical Center. TCC was a recipient of a Robert Wood Johnson Minority Medical Faculty Development Award at the time this work was completed and funding from this award also provided support for this project.
Conflict of interest: none declared.
The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs. The results of this study were presented as a poster at the Society of General Internal Medicine conference in Vancouver, BC, Canada, May 1st, 2003.
- Received for publication March 25, 2005.
- Revision received March 25, 2005.




{kind=link}