
Article Figures & Data
Figures
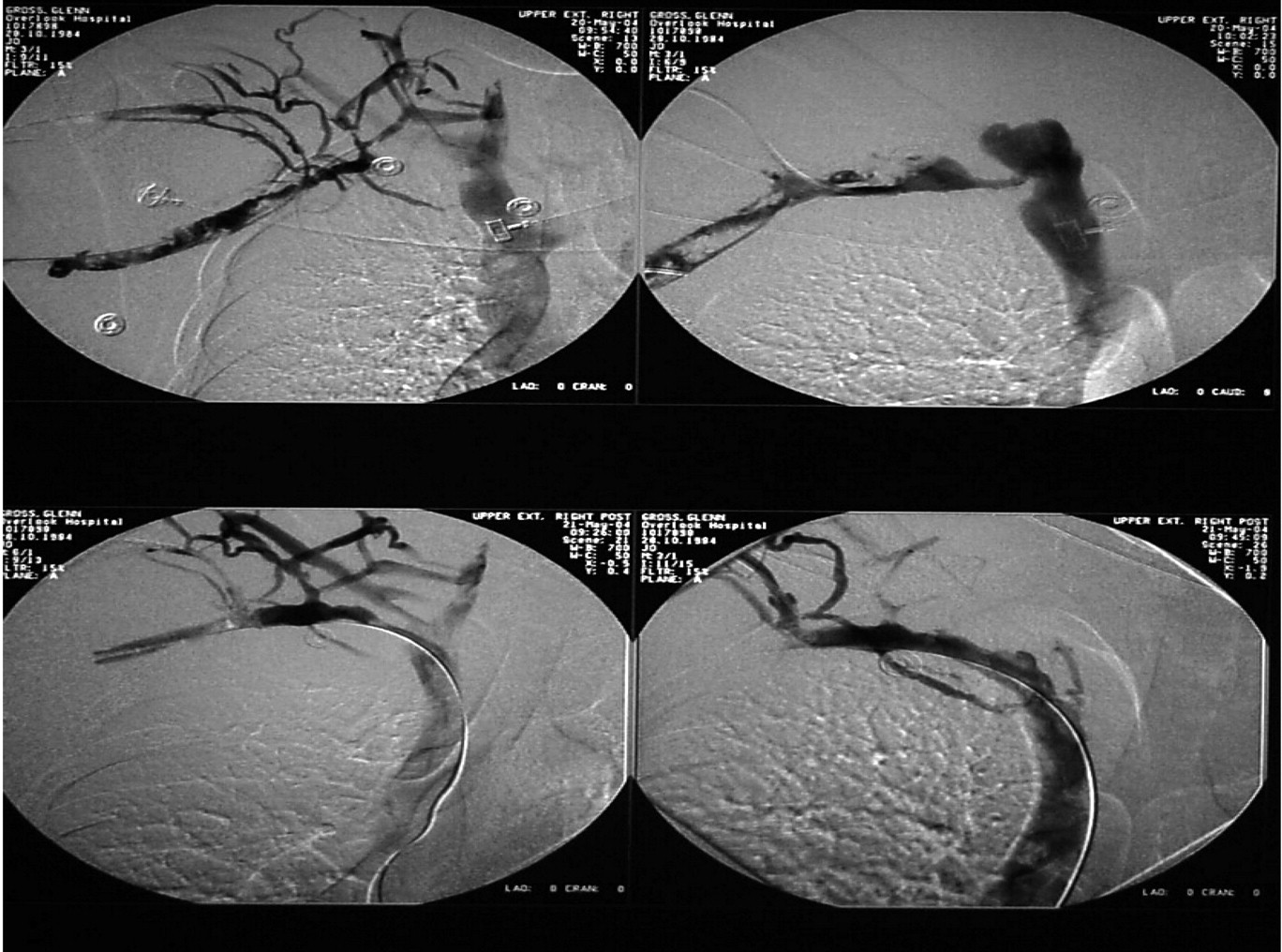
- Figure 1.
Venogram showing initial thrombus in the right brachial, axillary, and subclavian veins (upper left) and different stages of thrombolysis to successful lysis of thrombus (lower right).

Tables
- Table 1.
Signs and Symptoms of Axillary-Subclavianvein Thrombosis versus Thoracic Outlet Syndrome
Condition Symptoms Signs Axillary-subclavian thrombosis Vague shoulder or neck discomfort; arm, hand edema Supraclavicular fullness, palpable cord, extremity edema/cyanosis, jugular vein distention, dilated veins, unable to access catheter Thoracic outlet syndrome Pain radiating to arm; hand weakness Brachial plexus tenderness, arm/hand atrophy, positive Adson or Wright test Diagnostic Test Advantage Disadvantage Duplex Ultrasound Inexpensive, reproducible, noninvasive Failure to detect thrombus under clavicle in subclavian vein CT Vessel compression from outside; may define central thrombus Contrast required; not validated in entirety MRI Detects central thrombus with accuracy; good evaluation of collaterals Unsuitable for patients with metal implant or pacemaker; claustrophobia Diagnostic Test Maneuver Positive Test Mechanism Adson (scalene) The patient is instructed to inspire maximally and hold his or her breath while the neck is fully extended and the head is turned toward the affected side. The loss or decrease of radial pulse or the reproduction of neurologic symptoms suggests a positive test. The Adson (scalene) test causes narrowing of the space between the scalenus anticus and medius, resulting in compression of the subclavian artery and the brachial plexus. Halsted (costoclavicular) The patient is instructed to place his or her shoulders in a military position (drawn backward and downward). The loss or decrease of radial pulse or the reproduction of neurologic symptoms suggests a positive test. The Halsted (costoclavicular) test is used to narrow the costoclavicular space between the first rib and the clavicle, thereby causing neurovascular compression Wright (hyperabduction) To perform the test, the patient’s arm is hyperabducted 180°. The loss or decrease of radial pulse or the reproduction of neurologic symptoms suggests a positive test. The Wright (hyperabduction) test causes the neurovascular structures to be compressed in the subcoracoid region by the pectoralis tendon, the head of the humerus, or the coracoid process and muscles/tendons arising from the process.
Video Excerpts: Paget-Schroetter Syndrome in the Young and Active
1. Inspection: Muscular body habitus, homogenous, no-pitting edema, and diffuse erythema that blanched to palpation are prominent features on inspection. 2. History: Patient reveals swelling, redness, and limitation of function. Opening up of collateral circulation after development of thrombus. 3. History: Patient reveals neurovascular symptoms accentuated on abduction due to extrinsic mechanical compression at sub-coracoid level. A provocative test, Wright�s, is positive. 4. Wrights� Test: attenuation of radial pulse on abduction beyond 180 degrees; here there is disappearance of radial pulse beyond 180 consistent with mechanical obstruction at sub- coracoid level due to hypertrophied muscles. Patient reveals symptoms and signs of thrombosis as palpable cord, in addition to other non-specific features that might be seen in various other diagnoses.
Files in this Data Supplement:
- 1. Inspection - Muscular body habitus, homogenous, no-pitting edema, and diffuse erythema that blanched to palpation are prominent features on inspection.
- 2. History - Patient reveals swelling, redness, and limitation of function. Opening up of collateral circulation after development of thrombus.
- 3. History - Patient reveals neurovascular symptoms accentuated on abduction due to extrinsic mechanical compression at sub-coracoid level. A provocative test, Wright�s, is positive.
- 4. Wright's Test - Wrights� test shows attenuation of radial pulse on abduction beyond 180 degrees; here there is disappearance of radial pulse beyond 180 consistent with mechanical obstruction at sub-coracoid level due to hypertrophied muscles. Patient reveals symptoms and signs of thrombosis as palpable cord, in addition to other non-specific features that might be seen in various other diagnoses.




{kind=link}