
Article Figures & Data
Figures
- Figure 1.
The patient as the center of care.
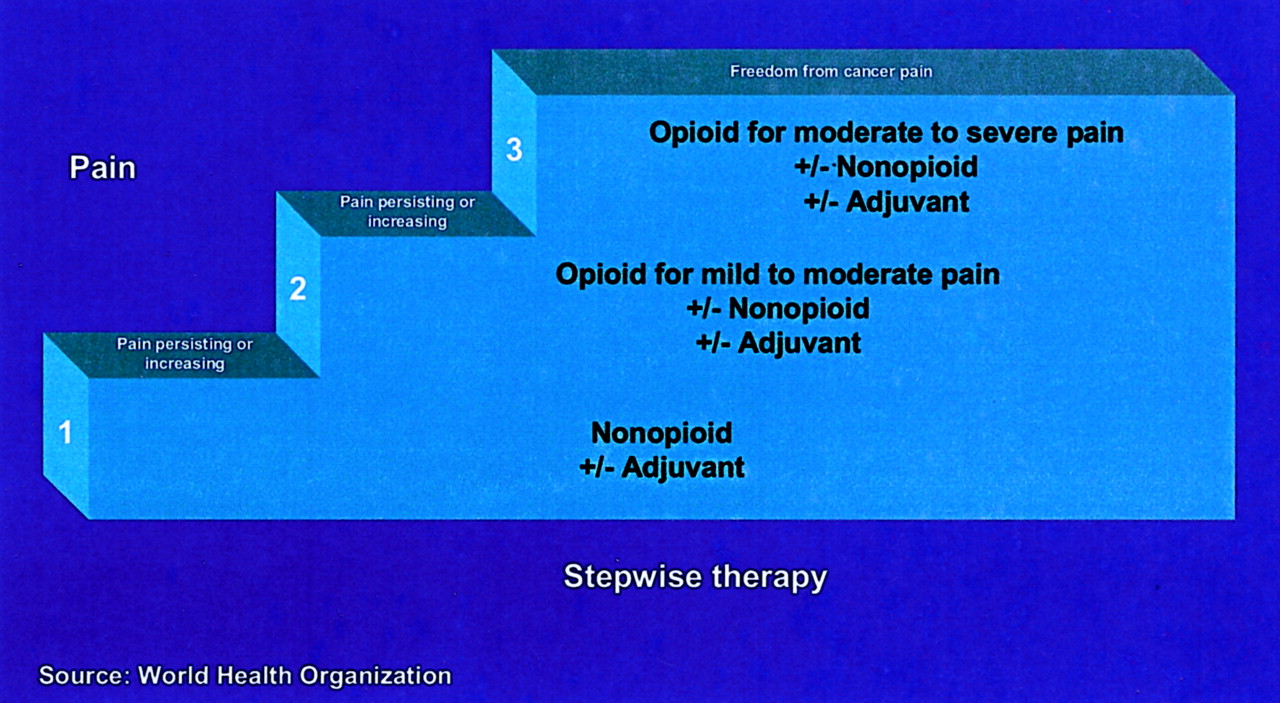
- Figure 2.
WHO analgesic ladder.


Tables
Drug (Brand name) Rx or OTC Usual Starting Dose Maximum Daily Dose Comments Cost/day* Acetaminophen (Tylenol, others) OTC 650 mg q4–6 hours 4000 mg 1000 mg is more effective than 650 mg in some patients <$1.00 Aspirin (various) OTC 650 mg q4–6 hours 4000 mg May not be tolerated as well as some newer NSAIDs. <$1.00 Diflunisal (Dolobid) Rx 1000 mg ×1 then 500 mg q12 hours 1500 mg Derived from salicylic acid. Little antipyretic activity $2.80 Nonacetylated Salicylates Choline magnesium trisalicylate (Trilisate, others) Rx 1500 mg ×1 then 1000 mg q12 hours 3000 mg Effective anti-inflammatory drugs, but less effective analgesics than aspirin. Have minimal antiplatelet effect and do not alter bleeding time. Aspirin cross-sensitivity less likely to occur. $3.00 Salsalate (Disalcid, others) Rx 1500 mg ×1 then 1000 mg q12 hours 3000 mg $2.50 Other NSAIDs: Propionic Acid Fenoprofen (Nalfon, others) Rx 200 mg q4–6 hours 1200 mg 90% eliminated by the kidney. $3.40 Flurbiprofen (Ansaid, others) Rx 50 mg q8–12 hours 300 mg At high doses, monitor closely for side effects. $1.00 Ibuprofen (Rx: Motrin, others; OTC: Advil, Nuprin, others) 400 mg q4–6 hours; OTC use: 200–400 mg q4–6 hours 2400 mg; OTC 1200 mg 200 mg ≈ 650 mg aspirin or APAP. 400 mg ≈ codeine/APAP $1.60 Ketoprofen (Rx: Orudis, others; OTC: Actron, Orudis-KT) 25–50 mg q6–8 hours; OTC use: 12.5–25 mg q4–6 hours 300 mg; OTC 75 mg 12.5 mg ≈ 200 mg ibuprofen; 50 mg superior to codeine/APAP $3.60 Naproxen (Naprosyn, others) Rx 500 mg ×1 then 500 mg q12 hours or 250 mg q6–8 hours 1250 mg first day then 1000 mg 250 mg ≈ 650 mg aspirin with longer duration. 95% eliminated by the kidney. <$1.00 Naproxen sodium (Rx: Anaprox, others; OTC: Aleve, others) 550 mg ×1 then 550 mg q12 hours or 275 mg q6–8 hours; OTC use: 220–440 mg ×1 then 220 mg q8–12 hours 1375 mg first day then 1100 mg; OTC 660 mg 275 mg ≈ 650 mg aspirin with longer duration; OTC 440 mg ≈ 400 mg ibuprofen. 95% eliminated by the kidney. Naproxen sodium may have less dyspepsia than naproxen <$1.00 Oxaprozin (Daypro) Rx 600–1200 mg qd 1800 mg Long serum half-life (42–50 hours) $1.66 Other NSAIDs: Acetic Acid Diclofenac potassium (Cataflam, others) Rx 50 mg q8 hours or 75 mg bid 150 mg May have less dyspepsia than the sodium salt. $1.10 Diclofenac sodium (Voltaren, others; extended-release: Voltaren XR, others) Rx 50 mg q8 hours or 75 mg bid; extended-release 100 mg qd 150 mg; for Voltaren XR 100 mg Also available with misoprostol 200 μg (Arthrotec 50 mg, 75 mg) to decrease GI toxicity. $1.00 Etodolac (Lodine, others; extended-release: Lodine XL) Rx 200–400 mg q6–8 hours; Lodine XL 400 mg qd 1200 mg; for Lodine XL 1000 mg 200 mg ≈ 650 mg aspirin or APAP $2.70 Indomethacin (Indocin, other; sustained release: Indocin SR, others) Rx 25 mg q8–12 hours; sustained release 75 mg qd 200 mg; for Indocin SR 75 mg bid Higher incidence of side effects. Also available in oral suspension. <$1.00 Ketorolac (Toradol) 10 mg q4–6 hours 40 mg 91% eliminated by the kidney. Use lower dose if >65 years or <50kg. Do not use >5 days $3.70 Sulindac (Clinoril, others) Rx 150–200 mg bid 400 mg Have few cases reporting less drug interaction with lithium <$1.00 Tolmetin (Tolectin, others;) Rx 200–600 tid 1800 mg 100% eliminated by the kidney. $1.65 Other NSAIDs: Fenamates Meclofenamate (various) Rx 50–100 mg q4–6 hours 400 mg Comparable with aspirin. Commonly used for dysmenorrhea. Diarrhea is common $1.10 Mefenamic acid (Ponstel) Rx 500 mg ×1 then 250 mg q6 hours 1250 mg Effective in dysmenorrhea. Do not use >1 week $5.20 Other NSAIDs: Naphthylalkanone Nabumetone (Relafen) Rx 1000 mg qd 2000 mg Can be given either qd or bid $2.40 Other NSAIDs: Oxicam Meloxicam (Mobic) Rx 7.5 mg qd 15 mg Dose-dependent COX-2/COX-1 inhibition $2.00 Piroxicam (Feldene, others) Rx 20 mg qd 20 mg Long serum half-life (50 hours). High incidence of side effects, especially in the elderly. <$1.00 COX-2 Inhibitors Celecoxib (Celebrex) Rx Acute pain: 400–600 mg first day, then 200 mg bid 400 mg Contraindicated in sulfa allergy $4.70 Valdecoxib (Bextra) Rx Dysmenorrhea: 20 mg bid 40 mg Approved for osteoarthritis/rheumatoid arthritis and dysmenorrhea only $5.40 Injectable NSAIDs Ketorolac IV/IM (Toradol) Rx <65 years: 60 mg ×1 then 30 mg q6 hours; ≥65 years: 30 mg ×1 then 15 mg q6 hours 120 mg 91% eliminated by the kidney. Use lower dose if >65 or <50kg. Do not use >5 days $7.99 ea dose * Cost/day = cost of usual daily dosage based on price listing at www.drugstore.com on 2003 Oct 21. Generic drugs were used whenever available.
qid, 4 times per day; tid, 3 times per day; bid, twice per day; qd, once per day; q, every.
Drug Examples of Brand Name Usual Adult Dose* Cost† Opioid Analgesic Combination (Controlled Drug Schedule) Codeine/APAP (C-III) Tylenol #2 15/300, Tylenol #3 30/300, Tylenol #4 60/300; Liquid 12/120/5 mL (c-v) 60 mg q 3–4 hours or 1–2 tab q4 hours; 15 mL q 4 hours $7–14/30s$6–10/120 mL Codeine/aspirin (C-III) Empirin #3 30/325, Empirin #4 60/325 60 mg q 3–4 hours or 1–2 tab q 4 hours $5–8/30s Hydrocodone/APAP (C-III) Lorcet-HD 5/500, Lorcet plus 7.5/650, Lorcet 10/650; Lortab 2.5/500, 5/500, 7.5/500; Vicodin 5/500, Vicodin ES 7.5/750, Vicodin HP 10/660; Lortab elixir 2.5/167/5 mL 10 mg q 3–4 hours or 1–2 tab q 3–4 hours $14–25/30s Hydrocodone/ibuprofen (C-III)‡ Vicoprofen 7.5/200 1 tab q 4–6 hours $32.55/30s Oxycodone/APAP (C-II) Percocet 2.5/325, 5/325, 7.5/500, 10/650; Roxicet 5/325, 5/500; Tylox 5/500 10 mg q 3–4 hours $6–24/30s Oxycodone/aspirin (C-II) Percodan-Demi 2.5/325, Percodan 5/325 10 mg q 3–4 hours $7–17/30s Propoxyphene napsylate/APAP (C-IV) Darvocet-N 50 50/325, Darvocet-N 100 100/650 100 mg q 4 hours $9–16/30s Propoxyphene/APAP (C-IV) Wygesic 65/650 1 tab q 4 hours $6–9/30s Other Step 2 Agents Tramadol‡ Ultram 50 mg 50–100 mg q 4–6 hours $25/30s Tramadol/APAP‡ Ultracet 37.5/325 1–2 tab q 4–6 hours $25/30s * The total dose of acetaminophen or aspirin should be <4 g/day.
† Cost based on generic pricing listed in 2001 Drug Topics Redbook.
‡ Not available in generic.
APAP, acetaminophen; q, every.
Drug Dosage Form (Brand Name) Usual Adult Dosage Cost* Immediate-Release Product Morphine IV: 1, 2, 4, 5, 8, 10, 15, 25, 50 mg/mL IV: 2–10 mg $18–30/100s tab; $9–13/100 mL liquid; $15–30/12s supp Tablets: 15, 30 mg (MSIR, generic) SC/IM: 10 mg q4 hours Liquid: 10 mg/5 mL, 20 mg/5 mL, 20 mg/mL, 100 mg/5 mL (Roxanol, others) PO: 10–30 mg q4 hours Suppositories: 5, 10, 20, 30 mg (various) Rectal: 10–20 mg q4 hours Hydromorphone IV: 1, 2, 4, 10 mg/mL (Dilaudid, others) IV/IM/SC: 1–4 q4–6 hours $37–70/100s tab; $22/6s supp Tablets: 1, 2, 3, 4, 8 mg (Dilaudid, others) PO: 2–6 mg q3–4 hours Liquid: 5 mg/5 mL (Dilaudid, others) Rectal: 3 mg q6–8 hours Suppositories: 3 mg (Dilaudid, others) Oxycodone Tablets: 5 mg (Percolone, Roxicodone) PO: 10–30 mg q 4 hours $30–36/100s tab Capsules: 5 mg (OxyIR) Liquid: 5 mg/5 mL (Roxicodone), 20 mg/mL (Roxicodone Intensol, OxyFAST) Meperidine† IV: 10, 25, 50, 75, 100 mg/mL (various) IV/IM/SC: 50–100 mg q3–4 hours $68/100s tab Tablets: 50, 100 mg (Demerol, various) PO: 50–100 mg q3–4 hours Liquid: 50 mg/5 mL (Demerol, various) Sustained-Release Products‡ Morphine Sustained-Release§ SR Tablets: 15, 30, 60, 100, 200 mg (MS Contin, Oramorph SR) Not recommended for initial therapy $90, $171, $334, $511/100s tabs Oxycodone Controlled-Release§ CR Tablets: 10, 20, 40, 80 mg Opioid-naive patients: 10 mg q 12 hours, and titrate $124, $238, $422, $793/100s Fentanyl Transdermal Patch Transdermal Patch: 25, 50, 75, 100 μg/hr (Duragesic) Opioid-naïve patients: 25 μg/hr every 3 days $62, $102, $163, $203/5s Opioids with Long Duration of Action‡ Levorphanol Tablets: 2 mg (Levo-Dromoran) PO: 2–4 mg q 6–8 hours $87/100s Methadone Tablets: 5, 10, 40 mg (Dolophine, others, generic) PO: 5–20 mg Q 6–8 hours $9, $15, $37/100s * Cost based on generic pricing listed in 2001 Drug Topics Redbook.
† Not recommended for cancer pain.
‡ Not recommended for initial therapy.
§ Tablets are not to be chewed or crushed.
Drug (Common Trade Name) Dose (mg) Equianalgesic to 10 mg SC/IV Morphine SC/IV:PO ratio Duration of Action (Hours) SC/IV PO/PR Morphine (MSIR, Roxanol) 10 30* 3:1 3–4 Codeine (with aspirin or APAP) 130 180–200 1.5: 1 3–4 Hydrocodone (in Lortab, Vicodin, others) NA 30 NA 3–4 Hydromorphone (Dilaudid) 1.5 7.5 5:1 3–4 Levorphanol (Levo-Dromoran) 2 4 2:1 6–8 Meperidine (Demerol) 100 300 3:1 3 Methadone (Dolophine, others) 10 for acute 2–4 for chronic 20 for acute 2–4 for chronic 2:1† 6–8‡ Oxycodone (Roxicodone, also in Percocet, Percodan, others) NA 30 NA 3–4 * IV/PO ratio (1:3) is based on chronic dosing. IM/PO ratio of 1:6 for single dose or intermittent dosing.
† Oral administration results in delayed onset and lower peak.
‡ Duration and half-life increase with chronic dosing.
APAP, acetaminophen; IM, intramuscular; PO, by mouth; SC, subcutaneous; IV, intravenous.
Oral 24-hr Morphine (mg/day) Duragesic Dose (μg/hr) 45–134 25 135–224 50 225–314 75 315–404 100 405–494 125 495–584 150 585–674 175 675–764 200 765–854 225 855–944 250 945–1034 275 1035–1124 300 Source: Duragesic package insert.
Class Drug and Dosage Estimated Cost/Dose* Stimulant Laxatives Bisacodyl (Dulcolax, Correctol, others): 5–10 mg orally $0.30–0.60 Senna (Senokot, others): 17.2 mg at bedtime $0.15–0.30 Osmotic Laxatives Lactulose (Cephulac, others): 15–30 mL bid (may be administered orally or rectally) $0.62–1.25 Polyethylene glycol (MiraLax): 17 g/day in 8 oz of water $1.30 Sorbitol 70% solution: 15–30 mL bid (may be administered orally or rectally) $0.25–0.50 Emollient Laxatives Docusate (Colace, others): 200–800 mg/day in 2 divided doses $0.05–0.20 Combination Agents Docusate (50 mg) plus senna (8.6 mg) tablets (Senokot–S, others): 2–4 tablets once or twice daily $0.30–0.60 * Cost is estimated using prices listed at www.drugstore.com (2004 Mar). Generic drugs were used whenever available.
bid, twice daily.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.