
Abstract
Background: Colonoscopy is becoming increasingly necessary for many patients in screening, diagnosing, and treating colorectal problems. Because the majority of rural doctors are family physicians, providing colonoscopy for the enlarging group of patients with valid indications in rural areas is difficult, unless rural family physicians perform the procedure. Subspecialists in academic settings have been responsible for most of the previously reported studies regarding colonoscopy. We have studied the safety and efficacy of the procedure when performed by rural family physicians.
Methods: A total of 200 sequential colonoscopies performed by family physicians in a rural setting were prospectively collected. Outcomes were measured based on current recommendations and benchmarks, including rate of reaching the cecum, time to reach the cecum, time to completion of the study, pathologic lesions found, and complications.
Results: The rate of reaching the cecum was 96.5%, and the average time to the cecum was 15.9 minutes. The average time to study completion was 34.4 minutes. The rate of neoplastic polyps and cancer found was 22.5% and 2.5%, respectively. There were no serious complications.
Conclusions: Adequately trained family physicians can provide safe and technically competent colonoscopy in a rural setting. Their results compare favorably to the currently reported comparative benchmarks from other endoscopists.
Colon cancer is a preventable but potentially fatal disease. In the last 2 decades, research has established that most colon cancers arise from neoplastic polyps within the colon. If these polyps are found early and removed, colon cancer can be prevented. There is currently a growing national movement to screen patients at risk for colon cancer, with a consequential growing need for surveillance of patients with a history of polyps or colon cancer. Many physicians and patients prefer colonoscopy as the “reference standard” screening study for colon polyps and cancer as well as polyp surveillance. Unfortunately, there is a lack of qualified colonoscopists in rural areas. The majority of rural doctors are family physicians. If colonoscopies are to be offered widely in rural areas, family physicians will need to perform them.
We present 200 prospectively collected sequential colonoscopy cases performed by rural family physicians, and we provide a comparison with regard to the quality and safety of the procedure as found by a current review of the literature.1–23 It has been reported that a competent colonoscopist can reach the cecum more than 90% of the time,1,3–6,10–12,15–18,21,22 in a reasonable amount of time.1,5,6,8,16,18,20–22 Colonoscopy can be completed with a minimal amount of risk to the patient3,6,7,10–12,16,18,20,23 and with a satisfactory rate of detection of pathologic lesions.3,8,10,11,12,16,24
Methods
Data were collected at the time of the procedure on 200 consecutive colonoscopies performed at St. Mary’s Hospital in Cottonwood, Idaho. St. Mary’s Hospital is a rural, 14-bed health care facility in north central Idaho that serves the largest county, in terms of area, in the state. This service area includes a patient population of 12,000 to 15,000 people. All colonoscopies completed by family physicians at St. Mary’s Hospital over a 2-year period from December 2000 through January 2002 were included in the study. These cases included both inpatient (urgent) and outpatient (nonurgent) study participants.
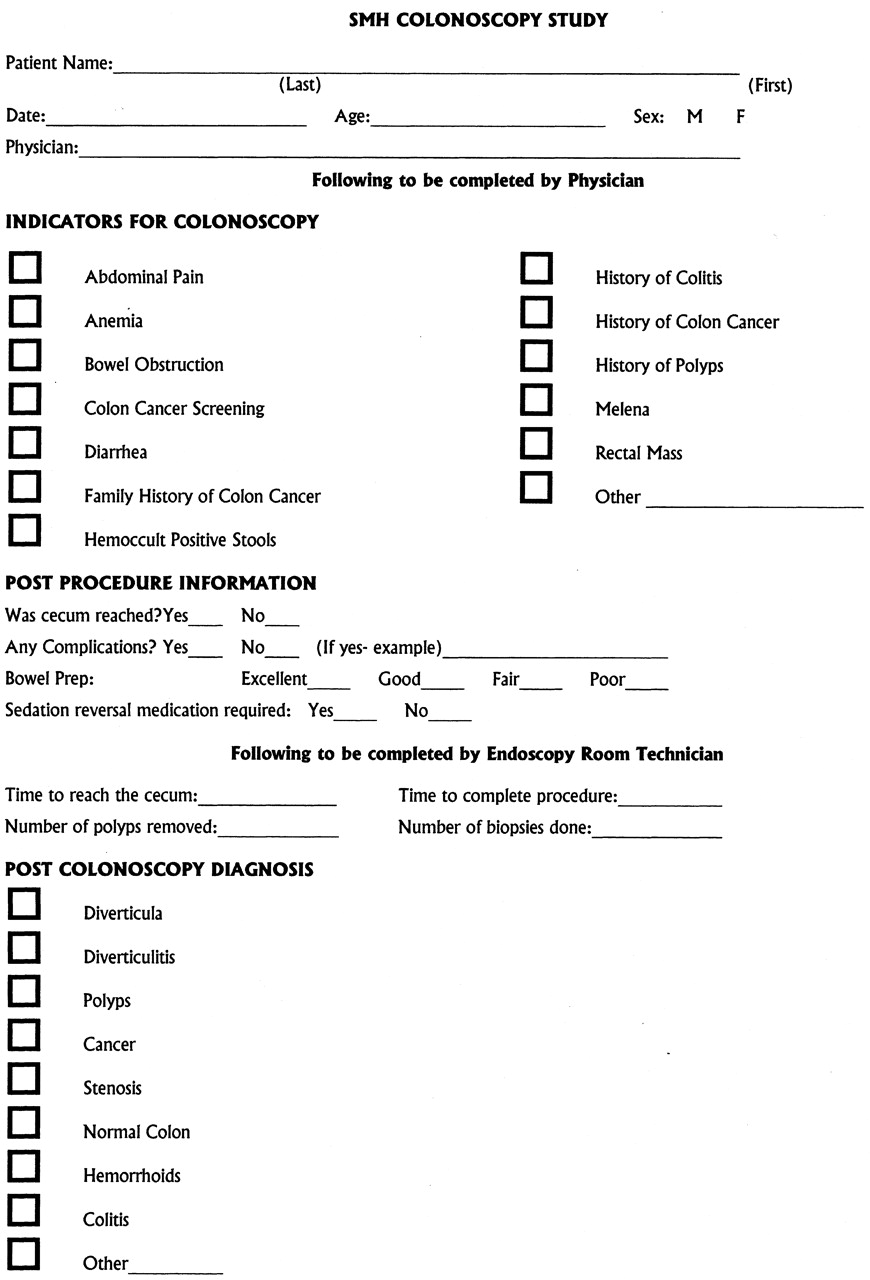
The data were collected prospectively during the study period. A standardized data collection form was completed at the time of each procedure. Figure 1 shows the standardized form used to collect colonoscopy data. The physician completed this form immediately after the colonoscopy (before pathology reports were available), and endoscopy room staff recorded procedure times. Study patients were then called 1 to 3 days after the procedure to review for any problems unless they were inpatients already.
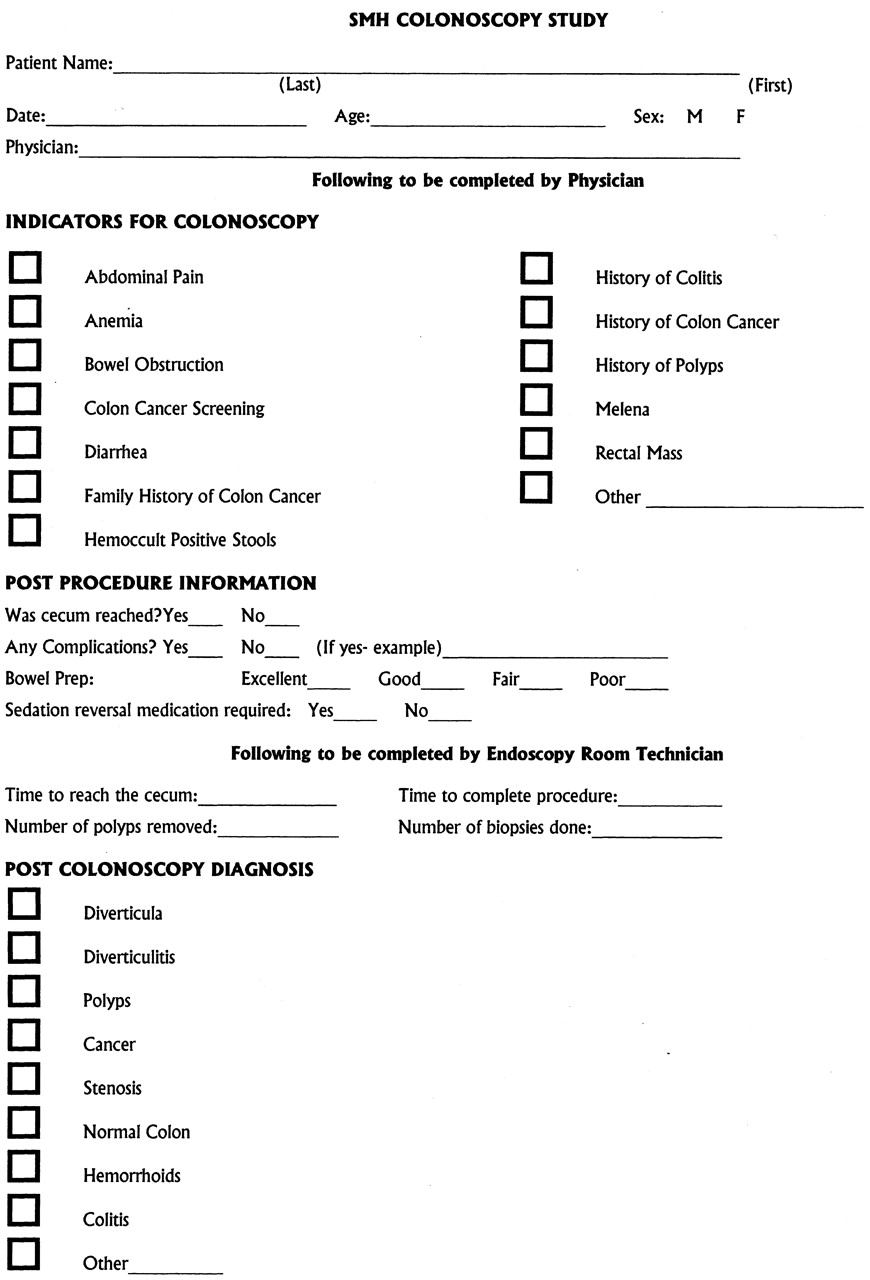
Standardized data collection form.
Pathology reports were collected for all procedures in which tissue specimens were obtained. Only in situations in which the pathologist confirmed biopsy results were polyps of neoplastic origin reported (adenomatous, tubular, or villous) or the case designated as colon cancer. Pathology reports of hyperplastic polyps and other nonmalignant findings were excluded from the analysis. Microsoft Access (Microsoft Corp., Redmond, WA) was the database used for storage and analysis of the data. Analysis of the data included only the calculation of totals (sums) and percentages, using all the cases included in the study. No statistical calculations were required or performed. Data were analyzed by category, including demographics, procedure indication, time to cecum, time to completion of colonoscopy, complications, and findings. After data collection, outcome results from this descriptive study were compared with others reported in the literature.
All procedures were completed by 1 of 4 rural family physicians. The 3 younger physicians had been trained to do colonoscopy in their residencies. A younger physician proctored the oldest physician (who had been doing flexible sigmoidoscopy) until he was proficient with colonoscopy.
The colonoscopies were all performed in a dedicated hospital endoscopy room at St. Mary’s Hospital. In all cases presented in this report, Certified Registered Nurse Anesthetists provided intravenous conscious sedation. It is noted that in other settings, other trained personnel could provide this service. Intravenous sedation used included a combination of midazolam, fentanyl, and propofol. Continuous cardiorespiratory monitoring was done during each procedure. An Olympus video colonoscope, model CFQ140L, was used for all procedures.
Results
Two hundred consecutive sequential colonoscopy procedures were performed over a 2-year period at St. Mary’s Hospital from December 2000 through January 2002 by 4 family physicians. Of the 200 patients, 91 were women and 109 were men. The age range of patients was from 16 to 90 years, with an average patient age of 62 years. The number of colonoscopies completed per physician varied from 23 to 108. Table 1 shows the estimated number of colonoscopies and years of experience performing colonoscopy by a physician before beginning the study. The most frequent indication for colonoscopy was rectal bleeding. Some patients had multiple indications for colonoscopy, whereas others were for colon cancer screening only. Twelve patients had procedures completed as inpatients for urgent reasons (ie, acute gastrointestinal bleeding). Table 2 shows the most common indications for colonoscopy.
Estimated Number of Colonoscopies and the Total Years Physicians Had Been Performing Colonoscopy before Beginning the Study
Most Common Indications for 200 Colonoscopies (Some Cases Had Multiple Indications)
The success rate for reaching the cecum was found to vary among physicians from 91 to 100%. The average rate for reaching the cecum overall was 96.5% (193 of 200) as shown in Table 3. Of the cases in which the cecum was not reached, 2 of 7 (29%) were the result of an obstructing colon cancer, whereas 4 of 7 (57%) were caused by a tortuous colon, and 1 was secondary to an anastomosis stenosis.
Rate to Reach the Cecum
The average time to reach the cecum per physician varied from 6.5 to 23.8 minutes and is shown in Table 4. The overall average time to reach the cecum was 15.9 minutes. The physician with the most experience had the shortest average time to the cecum, whereas the physician with the least experience had the longest. The overall average time for completion of the procedure was 34.4 minutes, including biopsies and polypectomies.
During the study, 45 of 200 (22.5%) cases were found to have neoplastic polyps that were confirmed by pathological examination. Table 5 demonstrates the frequency of neoplastic polyps found based on the most frequent preprocedure indications. Five of 200 (2.5%) patients had confirmed colon cancer. The most common preprocedure diagnosis, for patients subsequently found to have colon cancer, was hemoccult-positive stools [3 of 35 (8.5%)]. The 2 other patients with colon cancer had a preprocedure diagnosis of anemia or rectal bleeding.
Average Time to Cecum and Procedure Completion by Physician
Frequency of Neoplastic Polyps Based on Most Common Procedure Indications
Complications were considered to be adverse events that required intervention and occurred during the procedure or after, if related to the procedure. Complications included use of reversal agents with sedation, cardiorespiratory problems with sedation, bowel perforation, hospital admission, emergency department visits, and bleeding requiring transfusion that may have been related to the procedure. A review of the patients’ charts 2 years after completion of the study was completed to look for any possible delayed complications related to the procedure or missed colon cancers. There was 1 case of sedation-related bradycardia that required a single dose of atropine. One patient was admitted to the hospital for abdominal pain for observation overnight but required no intervention. One patient was admitted to the hospital after colonoscopy for observation for several hours because of other medical problems, the length of procedure, and the number of polyps removed. This patient required no intervention. One patient required placement of a rectal tube to relieve retained air within the colon, and symptoms resolved. There were no bowel perforations. No cases required sedation reversal medications.
Discussion
This study demonstrates that the quality of colonoscopy performed by adequately trained rural family physicians compares favorably with benchmarks reported in the literature.1–4 Although benchmarks have been poorly defined in the past, standards are now becoming more apparent. The literature suggests that the colonoscopist should be able to reach the cecum more than 90% of the time (Table 6). They should be able to perform a colonoscopy in a reasonable amount of time (Tables 7 and8). They are required to find and diagnose all significant pathologic lesions. Finally, they must be able to complete the procedure with minimal risk of complications and patient discomfort.
Review of Reported Rates of Reaching the Cecum More Than 90% of the Time
Review of Reported Time to Reach the Cecum
Review of Reported Time to Complete Colonoscopy
The reported success rate for reaching the cecum has, in the past, varied from 57% to more than 95%.3 Our success rate to reach the cecum was 96.5%. Our rate is similar to that of other published studies shown in Table 6. The majority of studies reported in the last 10 years confirm that skilled endoscopists can reach the cecum more than 90% of the time. However, when considering endoscopists in training, the rate of successful cecal intubation is usually lower than 90%.1,3,5,8,14,17,19 The 4 physicians in our study all had cecal intubation rates greater than 90%, suggesting that they meet the most widely studied standard in achieving technical competence in colonoscopy.
Confirmation of reaching the cecum can sometimes be a difficult task. All colonoscopies in our study were either videotaped or photographs were taken of cecal anatomy for confirmation, but these cases were not reviewed by outside staff. One study has considered the photograph documentation of cecal landmarks as confirmation of a complete colonoscopy.25 They found that it was difficult for reviewers to consistently agree on whether adequate visual documentation had been obtained. Since completion of our study, there have been no missed colon cancers reported in the study group.
The procedure time was divided into 2 primary measurements: (1) time to reach the cecum and (2) time to procedure completion. We found that our average time to the cecum was 15.9 minutes. However, there were cases in the study group in which polyps were removed before reaching the cecum; this would obviously lead to an increase in the time to reach the cecum. Further analysis was not performed on these cases.
Table 7 shows the time reported to reach the cecum in recent studies. It has been stated that a “reasonable standard” would be cecal intubation within 15 minutes or less.1 The 4 physicians in the current study showed a large amount of variation in their average time to reach the cecum (6.5 to 23.8 minutes). This seemed to be related to the number of previous procedures completed before beginning the study. A similar variation is seen when one compares the time to procedure completion among these same physicians (16.3 to 51.1 minutes). Table 8 shows recently reported studies that measured total procedure times for colonoscopy. The reported studies also show a considerable amount of variation in reported average times (22.7 to 34.7 minutes).
Various factors affect the amount of time required to reach the cecum and complete the colonoscopy procedure (including biopsies and polypectomies). Factors affecting these outcome measurements include physician experience, patient anatomy, quality of bowel preparation, pathology encountered, and reporting differences. For example, the study with the shortest reported time to reach the cecum subtracted the time consumed with polyp removal before reaching the cecum.22 At this time, more research is required to clarify these variables comparing colonoscopists and their procedure time.
Our study group included a heterogeneous collection of subjects. Patients were included regardless of their indication for colonoscopy. The indications ranged from asymptomatic screening to surveillance follow-up for polyps or prior colon cancer. Among this diverse patient population, we found a prevalence of neoplastic polyps of 22.5% and a prevalence of colon cancer of 2.5%. These findings are consistent with what has been reported previously.24
The study group included a wide variety of patients based on age, indications (both diagnostic and therapeutic) and complicating medical conditions. The group also included both an inpatient (urgent) and outpatient (nonurgent) population. Some patients were believed to be too “high risk” and were referred to a larger medical center with subspecialist management. However, the number of patients who were not offered colonoscopy by the family physicians was not followed. Despite this, there were no serious complications in the study group. One adverse cardiopulmonary event (1 of 200, 0.5%) required intervention. There were no colon perforations. Our rate of procedure- related morbidity was consistent with morbidity reported by others.6,7 The reported rate of mortality as a result of colonoscopy is greater than 1 in 5000, and major morbidity is approximately 0.4%.6,7 The rate of colon perforation is reported to vary from 0.14 to 0.65% for diagnostic procedures and 0.15 to 3.0% for therapeutic colonoscopy (including polypectomy).23
The primary weakness of the study is the relatively small sample size; however, we continue to collect sample data prospectively and look forward to reporting this in the future. It is possible that patient complications that occurred after the day of the procedure could have been missed if the patient presented to another hospital for evaluation and treatment. However, this is unlikely because of the rural locality of the study hospital and the distance to the next largest medical facility. In addition, this patient study group is part of a rural primary care 5-clinic system with ongoing longitudinal follow-up that uses central data management.
Conclusion
As the number of indications for the use of colonoscopy increase, rural patients face mounting geographic and distance-related obstacles to obtaining the endoscopy services that they need. This study provides an appraisal of the quality of 200 consecutive colonoscopies provided by 4 rural family physicians with various degrees of experience for a heterogeneous group of patients. Outcomes were measured and compared with other published results. We found that well-trained rural family physicians could safely provide diagnostic and therapeutic colonoscopy for their patients.
Further research regarding quality measures for colonoscopy and setting “standards” regarding compliance with these measures is needed to allow objective comparison between colonoscopists. Research in this area will advance the quality of colonoscopy provided to all our patients, both urban and rural.
Acknowledgments
We thank Cheri Holthaus and Pat Forsman, of St. Mary’s Hospital, who assisted greatly with data input and management.
- Received for publication March 6, 2004.
- Revision received March 6, 2004.




{kind=link}