
Abstract
Objective: Point-of-care testing (POCT) has been used in the United States for several decades to diagnose and monitor acute and chronic medical conditions. The aim of this study is to assess the use of POCT and perceived benefits of and concerns regarding POCT among US family physicians.
Methods: A total of 405 US family physicians responded to an electronic survey about their use of POCT for diagnosing and monitoring illnesses and for reducing referrals for specialty care. Respondents were also asked about the frequency of, benefits of, and concerns regarding the use of POCT.
Results: The top 10 conditions for which physicians reported using POCT for diagnosis are diabetes mellitus, urinary tract infections, strep throat, influenza, pregnancy, anemia, infectious mononucleosis, anticoagulation, acute cardiac conditions, and lipid disorders. More than half of the respondents use or would use >15 kinds of POCTs at least weekly. The perceived benefits of POCT included immediately available results and physician/patient satisfaction; perceived concerns included the accuracy and cost of the tests.
Conclusions: Findings show that a variety of point-of-care tests are used by US family physicians for immediate diagnosis and monitoring. With continuing technical improvements and decreasing costs, it is highly likely that POCT use will increase dramatically.
Point-of-care testing (POCT), sometimes referred to as near-patient or bedside testing, is defined as testing done at the site of patient care with rapid turnaround of results that enables immediate diagnosis and treatment plans.1 POCT in physician offices has been used for decades in the United States to diagnose acute conditions such as pregnancy, urinary tract infection, and streptococcal pharyngitis. POCT has recently been used to diagnose and monitor chronic medical conditions such as diabetes mellitus2⇓⇓–5 and to monitor the international normalized ratio (INR) of patients receiving warfarin therapy.6,7
Interest in POCT is increasing because of technological advances that enable smaller and simpler analytic devices that can provide measurements to diagnose and monitor conditions at the bedside and in physician offices at lower costs. Furthermore, POCT can improve patients' satisfaction with chronic disease management, especially in cases of type 2 diabetes mellitus and dyslipidemia, when results are immediately available and provide “teachable moments” during patient–physician encounters.8
Because of increasing interest among physicians and patients in implementing POCT in physician offices, and because manufacturers of point-of-care tests need to know what tests are valued by physicians, an international survey of primary care physicians was conducted in 5 countries.9 This report provides a more in depth report of US physicians' current and desired future POCT use and their opinions about the impact of health care reform on POCT.
Methods
This report uses the US data from a cross-sectional survey of primary care physicians in Australia, Belgium, the Netherlands, the United Kingdom, and the United States. A detailed description of the study methods of the international study, including survey development, is available elsewhere.9
Survey
The survey asked primary care physicians to identify up to 5 health conditions for which POCT might be helpful in making diagnoses, regardless of whether the tests were currently available. Respondents were also asked to identify up to 5 health conditions for which POCT might be helpful in monitoring or managing the condition, and up to 5 health conditions for which POCT might be helpful in reducing referrals. For each of these questions, respondents had the option to indicate that they did not believe POCT would be helpful. Respondents were then presented with the list of point-of-care tests and asked to indicate whether each test was currently available in their office and if they use it. For tests that respondents indicated were not currently available to them, physicians were asked to indicate whether they would use them, indicating desired use. Respondents indicating current or desired use were then asked to indicate how frequently they currently use or would use the test. Participants also responded to questions about the possible impact of health care or health care policy changes on POCT use.
The survey also collected information on the location of physicians' practices (urban, rural or suburban), years of practice, as well as their age and sex.
Participants and Data Collection
The target sample size for US physicians was 383. This would allow relatively narrow confidence intervals for the point estimates for POCT use.
Data were collected in 3 phases. The survey request was initially sent to a random selection of 2000 active American Academy Family Practice members as well as 552 members of the American Academy Family Practice National Research Network. A total of 101 family physicians completed the survey in September 2013. Because of the low response, MDLinx, a commercial physician polling service, was contacted. The survey request was sent to 3000 regionally representative family physicians who are members of the MDLinx panel, and 298 complete surveys were received from these physicians, each of whom received $20 for completing the survey. State family physician research networks in Oklahoma and Oregon were contacted as well, and 6 of these physicians completed the survey for a total of 405 participants.
Statistical Analyses
Data were analyzed using SPSS (version 22; IBM/SPSS, Inc., Chicago, IL). The International Classification of Primary Care was used to categorize the responses to open-ended questions about conditions for which physicians would like to use POCT. Coding was performed by 1 person (FA), and any ambiguities were resolved by a physician coauthor (AJS). Descriptive statistics were used to display the frequency for each condition. They were also generated for tests currently used or desired by all respondents, as well as frequency of tests. Responses to open-ended questions about changes in health care policy were coded by the main author (AJS).
Results
A total of 405 physicians responded from among the 5553 physicians who were sent the E-mail invitation, giving a response rate of 7%. Of respondents, 71% were male and 29% were female; 47% practiced in an urban location, 25.2% in a suburban location, 21.2% in a semirural location, and 5.9% in a rural location.
Table 1 displays the top 10 conditions for which respondents indicated that POCT could help make a diagnosis. Diabetes mellitus was the most frequently cited condition, followed by urinary tract infection and strep throat.
Top 10 Conditions for Which a Point-of Care Test Could Help Make a Diagnosis
Table 2 displays the top 10 conditions for which respondents indicated that POCT could help to monitor or manage the condition. Again, diabetes mellitus was the most frequently listed condition, followed by anticoagulation, lipid disorder, and anemia.
Top 10 Conditions for Which a Point-of Care Test Could Help Monitor or Manage
Table 3 displays the top 10 conditions for which respondents indicated that POCT would help to reduce referrals for specialty care or hospital admission. Acute cardiac condition, heart failure, and pulmonary embolism were the top 3 most frequently listed conditions.
Conditions for Which a Point-of Care Test Would Help Reduce Referrals for Specialty Care or Hospital Admission
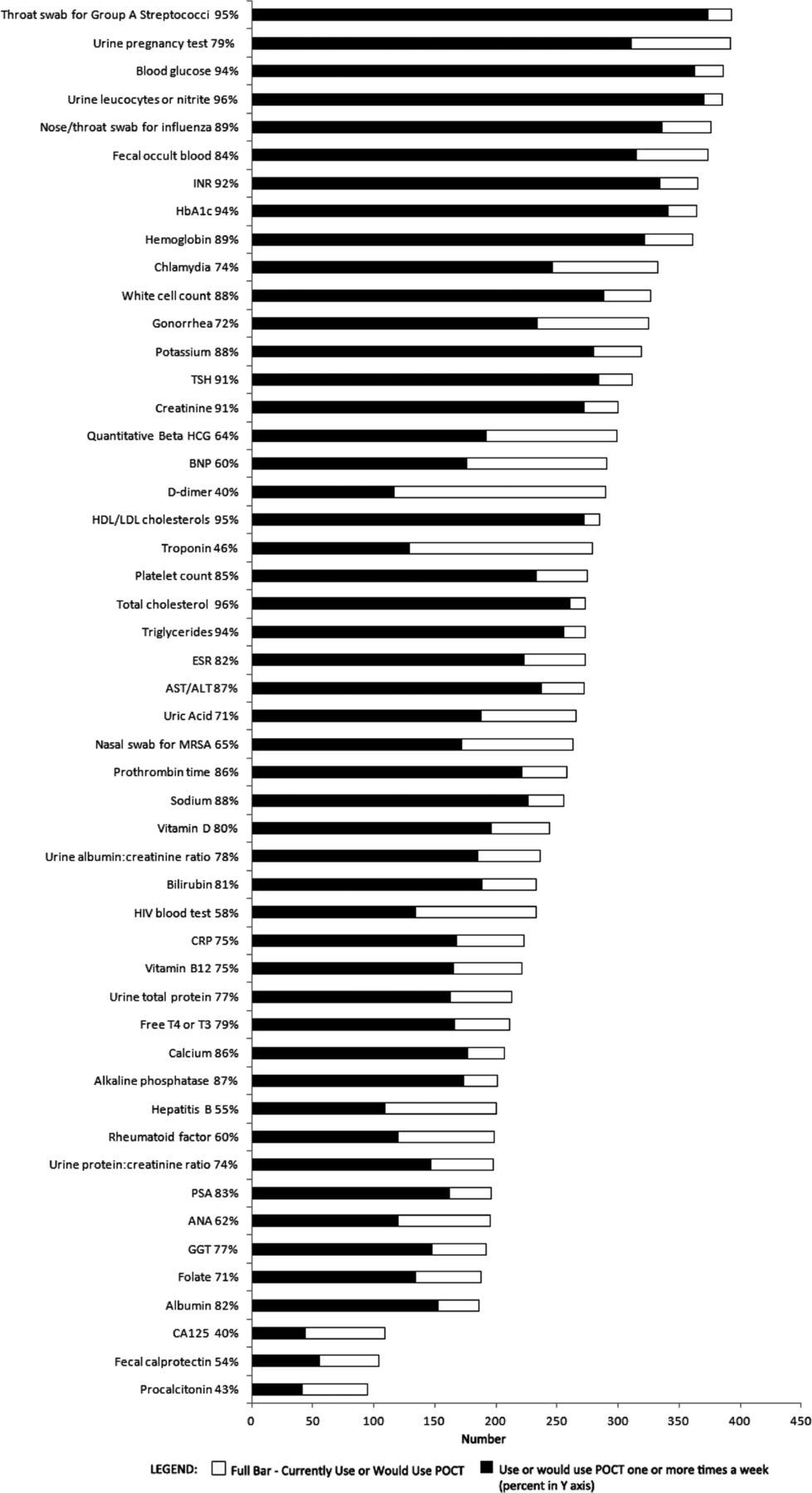
Figure 1 displays point-of-care tests in descending order of use or potential use. The percentages indicate the proportion of respondents who use or would use each point-of-care test ≥1 time/week, among those reporting current or desired use for each test. More than 80% of the physicians who responded to the survey indicated current or desired use of a throat swab for the group A streptococci test, a urine pregnancy test, blood glucose and HbA1c tests, urine leukocyte or nitrite test, a nose/throat swab for influenza, fecal occult blood test, INR test, hemoglobin test, chlamydia test, blood white cell count, and gonorrhea test. The frequency of current or desired use was also high for these tests: between 72% and 96% of those who use or would use these tests reported that they use or would use them ≥1 time/week.

The numbers of respondents who use or would use the point-of-care testing ≥1 time a week (black bar) among those reporting current or desired use (full bar). The percentages indicate the proportion of respondents. ALT, alanine aminotransferase; ANA, antinuclear antibody; AST, aspartate aminotransferase; BNP, brain natriuretic peptide; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; GGT, gamma-glutamyl; hCG, human chorionic gonadotropin; HDL, high-density lipoprotein; INR, international normalized ratio; LDL, low-density lipoprotein; MRSA, methicillin-resistant Staphylococcus aureus; PSA, prostate-specific antigen; TSH, thyrotropin-releasing hormone.
All 405 primary care physicians responded to the question, “Do you think current changes in US health care or policy are likely to have any impact on the use of POCTs? If so, please explain.” Of the respondents, 63% (n = 258) expressed the belief that POCT use will be affected by current changes in health care or policy; 23% (n = 94) believed that POCT use would not be affected, and 14% (n = 56) were unsure.
Among those who believed that health care or policy changes would affect POCT use (n = 258), 36% (n = 92) expect that POCT usage would increase. Select responses to this question are presented in Table 4. Of those who believed that health care or policy changes would affect POCT use, 44% (n = 114) expected POCT usage to decrease. Twenty percent (52 of 258), expect health care or policy changes to have a mixed effect on POCT use.
Sample Comments about the Potential Impact of Health Care Policy Changes on the Use of Point-of-Care Testing
A total of 317 physicians responded to the survey item, “Please share any other comments, including benefits and concerns about POCT.” Of these physician, 120 (38%) identified benefits, 87 (27%) identified concerns, and 17 (5%) identified both benefits and concerns. Table 5 provides some sample responses to this question.
Sample Comments about Benefits of and Concerns about Point-of-Care Testing
Discussion
POCT has traditionally been used to diagnose acute conditions in outpatient care settings and to diagnose pregnancy. All the top conditions for which POCT could help make a diagnosis, as identified by physicians in this study, are acute conditions (except diabetes mellitus). Our study shows that diabetes mellitus is the most frequent condition for which primary care physicians currently report making a diagnosis using POCT; this aligns with the introduction of hemoglobin A1c (HbA1c) as a tool for the diagnosis of diabetes mellitus. With the increasing epidemic of obesity and type 2 diabetes mellitus—not only in the United States, but also in Asia and Oceania—the availability of POCT for HbA1c, in addition to blood glucose, is very helpful in diagnosing new-onset diabetes mellitus and in monitoring treatment response. Fasting is not required for HbA1c, which is an advantage over using the fasting blood glucose measure. Now that testing of lipid concentrations does not require fasting10 (except for patients with markedly elevated triglycerides), the 3 major coronary artery disease risk factors that can be controlled with treatment (glucose, lipids, blood pressure), can be monitored during office visits, both giving immediate feedback to patients and allowing immediate treatment changes to be made.
To our knowledge, this is the first US study to elicit primary care physicians' opinions regarding the use of and desire for POCT among a national sample of physicians, detailing the usefulness of these tests for diagnosis and monitoring and for reducing referrals. A limitation of this study is that the survey measured physicians' self-reported use and opinions of POCT, rather than objectively measuring their behavior. Whether the referral rates would actually decrease, for example, could only be determined by measuring actual referrals, preferably in a randomized trial. A second limitation is the low response rate, though the written comments enrich the survey results. The response rate for the same survey among family physicians in the 4 other countries where the survey was administered varied from 10% to 68%.9 Responses regarding the use of point-of-care urine pregnancy, urine leukocyte or nitrite, and blood glucose tests were similar among family physicians from the United States and the other countries. However, US physicians tend to use more point-of-care fecal occult blood tests, throat swabs for group A streptococci, nasal swabs for influenza, and HbA1c tests.
The attitude of US physicians toward the anticipated impact of US health policy change on POCT is mixed. More physicians predicted decreased use than increased use. This may reflect the overall pessimistic attitude of physicians about the health policy changes implemented by the Affordable Care Act and its implications and meaningful use requirements, which have been burdensome for many primary care physicians. Nonetheless, US physicians cited more benefits than concerns about POCT use; 43% mentioned benefits as opposed to 32% who mentioned concerns. The cited benefits agree with prior studies that demonstrated decreased turnaround time for results leading to increased patient and physician satisfaction.
Conclusion
Many physicians reported they use or would use POCT now and in the future, suggesting a real opportunity for continued expansion of POCT technology. If point-of-care tests are highly reliable, easy to use, and inexpensive, it is highly likely their use will increase dramatically, leading to better diagnosis of acute and chronic medical conditions, better management of chronic medical conditions such as diabetes mellitus, and improved physician and patient satisfaction. POCT may also decrease referrals for specialty care and to emergency departments, but this hypothesis needs to be tested.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication August 6, 2015.
- Revision received December 15, 2015.
- Accepted for publication January 4, 2016.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Utilisation and trends of laboratory testing and point-of-care testing in primary care in Germany: an analysis of claims data
- C-reactive protein cut-offs used for acute respiratory infections in Danish general practice
- Impact of point-of-care panel tests in ambulatory care: a systematic review and meta-analysis
- XW-100: First FDA CLIA-Waived CBC Analyzer Designed for Physician Office Use
- Impact of point-of-care C reactive protein in ambulatory care: a systematic review and meta-analysis
- Social Determinants of Health and Beyond: Information to Help Family Physicians Improve Patient Care