
Abstract
Upper gastrointestinal bleeding is an uncommon but potentially serious, life-threatening condition in children. Rapid assessment, stabilization, and resuscitation should precede all diagnostic modalities in unstable children. The diagnostic approach includes history, examination, laboratory evaluation, endoscopic procedures, and imaging studies. The clinician needs to determine carefully whether any blood or possible blood reported by a child or adult represents true upper gastrointestinal bleeding because most children with true upper gastrointestinal bleeding require admission to a pediatric intensive care unit. After the diagnosis is established, the physician should start a proton pump inhibitor or histamine 2 receptor antagonist in children with upper gastrointestinal bleeding. Consideration should also be given to the initiation of vasoactive drugs in all children in whom variceal bleeding is suspected. An endoscopy should be performed once the child is hemodynamically stable.
Upper gastrointestinal bleeding (UGIB) is an uncommon but potentially serious and life-threatening clinical condition in children. Anatomically, the upper gastrointestinal (GI) tract includes the esophagus to the ligament of Treitz; therefore UGIB includes bleeding that originates throughout this region. Common signs and symptoms at presentation include hematemesis (73%), melena (21%), and coffee-ground emesis (6%); however, patients may also experience epigastric pain, abdominal tenderness, or dizziness.1⇓–3
The worldwide mortality rate for UGIB in children can range from 5% to 21%, which reflects the diverse populations that experience conditions associated with UGIB.4,5 In the United States mortality is on the lower end of the spectrum as a result of improved pediatric intensive care, advances in diagnosis and treatment, as well as in the stabilization and management of critically ill patients. Mortality can be decreased by early identification of UGIB, and improved morbidity and mortality are most often the result of a multidisciplinary approach to care.3 Among children admitted to pediatric intensive care units (PICUs), those with UGIB require more red blood cell transfusions, have longer hospital stays, and have a longer duration of mechanical ventilation.6
Literature Search
PubMed was searched in Clinical Queries using the key search terms children or infants, gastrointestinal bleeding, and gastrointestinal hemorrhage, pathogenesis, diagnosis, and treatment. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. We also searched Clinical Evidence, the Cochrane database, Essential Evidence Plus, the National Center for Biotechnology Information at the US National Library of Medicine, the National Guideline Clearinghouse, and DynaMed. Our initial search date was November 5, 2012, with follow-up searches preformed in December 2012, May 2013, and February 2014.
Epidemiology
In a case-crossover study conducted in France, the incidence of UGIB in children was 1 to 2 in 10,000 per year.7 This study showed a female-to-male ratio of 1.2:1, and symptoms of hematemesis were present in 96.6%, melena in 14.1%, and hemorrhagic shock in 2.8%.7 Among the population in this study, 11.3% had a personal history of ulcer or prior UGIB, 5.7% had portal hypertension, and 8.5% had a relevant medical history, for example, a coagulation disorder or rheumatoid purpura.7 A total of 20 patients (11.3%) in this study required transfusion.7 The incidence of significant UGIB in children admitted to the PICU has been reported to be 0.4% to 1.6%.8 A prospective comparative study conducted in a PICU in a tertiary care, university-based facility in the United States found a 25% prevalence of UGIB.5 The overall mortality of patients in this study was 4.8%, with a significantly higher mortality seen in patients with UGIB than in those without (16% vs 1.3%; P = .0001).5 A prospective Canadian study conducted in a PICU within a university hospital, detected UGIB in 63 of 984 children (6.4%), but only 0.4% had a clinically significant outcome, for example, hypotension, death, or transfusion occurring within 24 hours after the bleeding episode.9 In this study 43% were female and their mean age was 5.3 years.9 The highest frequency of developing UGIB (69.8%) occurred within the first 72 hours of admission to the PICU.9
Causes
The causes of UGIB can be categorized by age groups. In newborns the predominant causes include coagulation disorders such as vitamin K deficiency, cow milk intolerance, gastritis from stress, sepsis, and trauma from the placement of nasogastric tubes.10 From 1 month to 1 year of age, the most prevalent causes are caustic ingestions, duplication cysts, foreign body ingestion, stress esophagitis, medication-induced bleeding (eg, nonsteroidal anti-inflammatory drug [NSAID] use), and peptic ulcer bleeding.10 From 1 to 5 years of age, causes include erosive esophagitis, gastritis, caustic ingestions, peptic ulcer bleeding, varices, and vomiting-induced bleeding, for example, from a Mallory-Weiss tear.10 From ages 5 to 18 years, bleeding can arise from coagulation disorders, gastritis, Dieulafoy lesions (an anomalous artery located in the digestive tract), erosive esophagitis, peptic ulcer disease, caustic ingestions, and vomiting-induced bleeding.10 Crohn's disease is an uncommon cause of UGIB in children and adolescents.11,12 Certain foods may create confusion for children and parents by mimicking the appearance of blood in vomitus (eg, red food coloring, fruit-flavored drinks, fruit juices, and beets) or by mimicking the appearance of melena in stools (eg, iron, grape juice, spinach, or blueberries).11,12 All suspicious findings consistent with blood should be investigated further.
Globally, the etiology of UGIB differs significantly based on variations in patient population and the presence of comorbid conditions.1 In the Middle East and Asia, the causes of UGIB include peptic ulcer bleeding (24%), varices secondary to viral hepatitis (23%), erosive esophagitis (0.2%), and vomiting-induced hematemesis (0.2%).1 In North and South America, peptic ulcer bleeding (44%), varices (11%), vomiting-induced hematemesis (1.2%), and erosive esophagitis (0.6%) comprise the majority of UGIB cases.1
Risk Factors
Risk factors for UGIB vary. NSAID use and Helicobacter pylori infection should be considered in children with severe UGIB. The observed risk of UGIB with NSAIDs is 7.2 per 100,000, based on a study of 55,785 children.13 The risk of developing UGIB with NSAID use is greater in the 2-month-old to 7-year-old age group (odds ratio [OR], 14.1) versus the 8- to 16-year-old age group (OR, 3.4).7 H. pylori has been found in up to 49% (41 of 84) of children presenting with UGIB.14 This infection represents an important risk factor, especially in children with hereditary hemorrhagic disorders such as hemophilia15 (Table 1). Other risk factors include peptic ulcer disease, portal hypertension or varices, and bleeding disorders.3 Children who require mechanical ventilation during the course of their hospitalization have a higher incidence of UGIB if they also experience a high pressure ventilator setting (relative risk, 3.73) or organ failure (relative risk, 2.85).20 Other risk factors include trauma (OR, 20.9), shock (OR, 17.4), and operative procedures >3 hours long (OR, 3.6).5
Associated Conditions
Multiple disorders can contribute to the development of an UGIB in pediatric patients. Hematologic disorders, such as hemophilia A and B and Von Willebrand disease, predispose patients to UGIB secondary to the increased risk of bleeding mucosal membranes.15 Conditions such as biliary atresia, portal vein thrombosis, primary sclerosing cholangitis, autoimmune hepatitis, Budd-Chiari syndrome, and cystic fibrosis predispose patients to UGIB through the development of portal hypertension, which can lead to the formation of varices, a known cause of UGIB.21
Screening and Prevention
There are no guideline-based screening or prevention recommendations. However, screening endoscopy is recommended for patients with conditions that have a high incidence of portal hypertension in an effort to identify variceal formation as early as possible.22 Endoscopic findings of red markings or gastric varices are of concern for the presence or future development of UGIB.3 Children who have been diagnosed with esophageal varices, red markings, or gastric varices on initial screening endoscopy should undergo endoscopic sclerotherapy or band ligation to prevent hemorrhage.22 In addition, the use of β-blockers in at-risk children is recommended as prophylaxis for variceal bleeding.23 Children in a PICU should be considered for prophylaxis with histamine 2 receptor antagonists or proton pump inhibitors.24
Diagnosis
There are no randomized controlled trials, Cochrane reviews, or systematic reviews of the diagnostic approach in children with UGIB. The diagnostic approach is mostly extrapolated from studies of adults; the key points are an extensive history and examination, laboratory evaluations, and diagnostic procedures.
Differential Diagnosis
The differential diagnosis for UGIB includes causes for lower GI bleeding (LGIB), non-GI sources, ingested maternal blood, or food sources imitating hematemesis or melena. Causes of LGIB include conditions such as Crohn's disease, ulcerative colitis, hemorrhoids, anal fissures, and Meckel diverticulum. Non-GI sources of bleeding include epistaxis or hemoptysis that may present with symptoms similar to those of UGIB, such as hematemesis, melena, and positive occult blood tests (Table 2). Maternal sources include ingestion of blood during delivery or from cracked nipples during breastfeeding; infants who ingest maternal blood may present with hematemesis or melena.10
History
Children with a history of concurrent major illness that require PICU care, such as sepsis and respiratory failure, may present with stress gastritis or stress ulcers.3 Indications for possible variceal bleeding include a history of autoimmune hepatitis, Budd-Chiari syndrome, cystic fibrosis, biliary atresia, portal vein thrombosis, or primary sclerosing cholangitis.22 Family history should be assessed for inheritable diseases that may increase risk for UGIB, for example, liver disease, any history of requirements for clotting factor replacement, hemophilia A, hemophilia B, and Von Willebrand disease.15
Defining the amount of bleeding and any associated symptoms is important. If the patient is able to subjectively report symptoms, he or she should be assessed for abdominal pain, dizziness, shortness of breath, and palpitations. Signs and symptoms that increase suspicion of UGIB include abdominal or chest pain, coffee ground–like emesis, black tarry stools, bright red blood from the rectum, or hematemesis.3 The stool color may be helpful to differentiate UGIB from LGIB. Maroon stools or frank blood from the rectum may signal rapid UGIB.25 In children significant blood loss may occur before tachycardia, hypotension, or tachypnea are observed; for example, slow bleeding may result in a loss of 13% of total blood volume with no change in hemodynamic status.25 Furthermore, a loss of palmar crease with wrist hyperextension may indicate a >50% loss of blood volume.25
A comprehensive review of medications should be performed, with a special focus on those medications that may increase the risk of UGIB. These include aspirin, NSAIDs, corticosteroids, and selective serotonin reuptake inhibitors (SSRIs).3 NSAIDs increase the risk of UGIB by damaging gastric mucosa and promoting tissue friability.26 The greatest risk of developing gastric complications typically occurs within 30 days of initiating NSAID therapy.26 SSRIs inhibit platelet aggregation, and the concurrent use of NSAIDs and SSRIs further increases the risk for UGIB.27 In addition, corticosteroid use in neonates has been associated with increased mortality from GI hemorrhage.28 One study found high-dose dexamethasone used in the treatment of ventilator-dependent premature infants was associated with major complications, such as perforated gastric ulcers, duodenal ulcers, and upper GI hemorrhage.28 That 5-year review found a 66% mortality rate among children who received high-dose dexamethasone and subsequently developed a GI complication.28
Physical Examination
Airway, breathing, and circulation should be assessed to evaluate hemodynamic stability. Vital signs should be monitored for tachycardia, tachypnea, hypotension, orthostatic hypotension, and capillary refill (Tables 3 and 4). Tachycardia is the most sensitive indicator for blood loss in children.8 General presentation should be noted, including confusion, irritability, and respiratory distress. Ecchymosis may signal a poorly controlled bleeding disorder or trauma. Pallor may indicate severe blood loss but may not be present in an acute UGIB. The abdomen should be assessed for guarding, epigastric or rebound tenderness, surgical scars, hepatomegaly, right upper quadrant tenderness, or other signs or sequelae of chronic liver disease.11 The evaluation should also include a rectal examination to identify any hemorrhoids or fissures that may indicate a lower GI source of bleeding. A stool sample should be obtained for occult blood testing (eg, hemoccult).11
Diagnostic Testing
Blood should be obtained to measure hemoglobin, hematocrit, blood urea nitrogen, creatinine, platelet count, prothrombin and partial thromboplastin times, international normalized ratio, liver enzymes (eg, aspartate transaminase and alanine aminotransferase), and type and crossmatch8 (Table 5). In newborns with suspected UGIB, an Apt test can differentiate neonatal blood from maternal blood.29 A blood urea nitrogen—to–creatinine ratio >30 may be helpful to distinguish UGIB from LGIB (specificity, 98%; sensitivity, 69%; likelihood ratio, +34.4 and −0.32, respectively).30 Placing a nasogastric tube for gastric lavage can improve the accuracy of endoscopy.11 In addition, gastric aspirate can be assessed for occult blood using a Gastroccult (Beckman Coulter, Inc., Palo Alto, CA).32 Stool specimens should be obtained to evaluate the presence of heme using hemoccult testing; however, hemoccult is not accurate in testing for blood in gastric aspirate because of the pH of gastric contents.11,12 Undercooked meats and raw fruits or vegetables may create false-positive hemoccult results; therefore a positive hemoccult result warrants investigation.11,12
Urgent endoscopy, which is performed <12 hours after admission, is indicated for bleeding that requires transfusion or for hemodynamic instability; otherwise, endoscopy can be performed within the first 24 hours of admission8 (Tables 6 and 7). The reported efficacy of endoscopy for controlling UGIB is approximately 90%.34 There are no randomized controlled trials or systematic reviews of follow-up endoscopy in children with significant UGIB. Based on adult studies, repeat endoscopy in children with life-threatening UGIB should be considered within 48 to 72 hours after the initial endoscopy.34 In children with severe peptic ulcer bleeding, follow-up endoscopy may be considered within 4 to 6 weeks to assess ulcer healing.8
Treatment
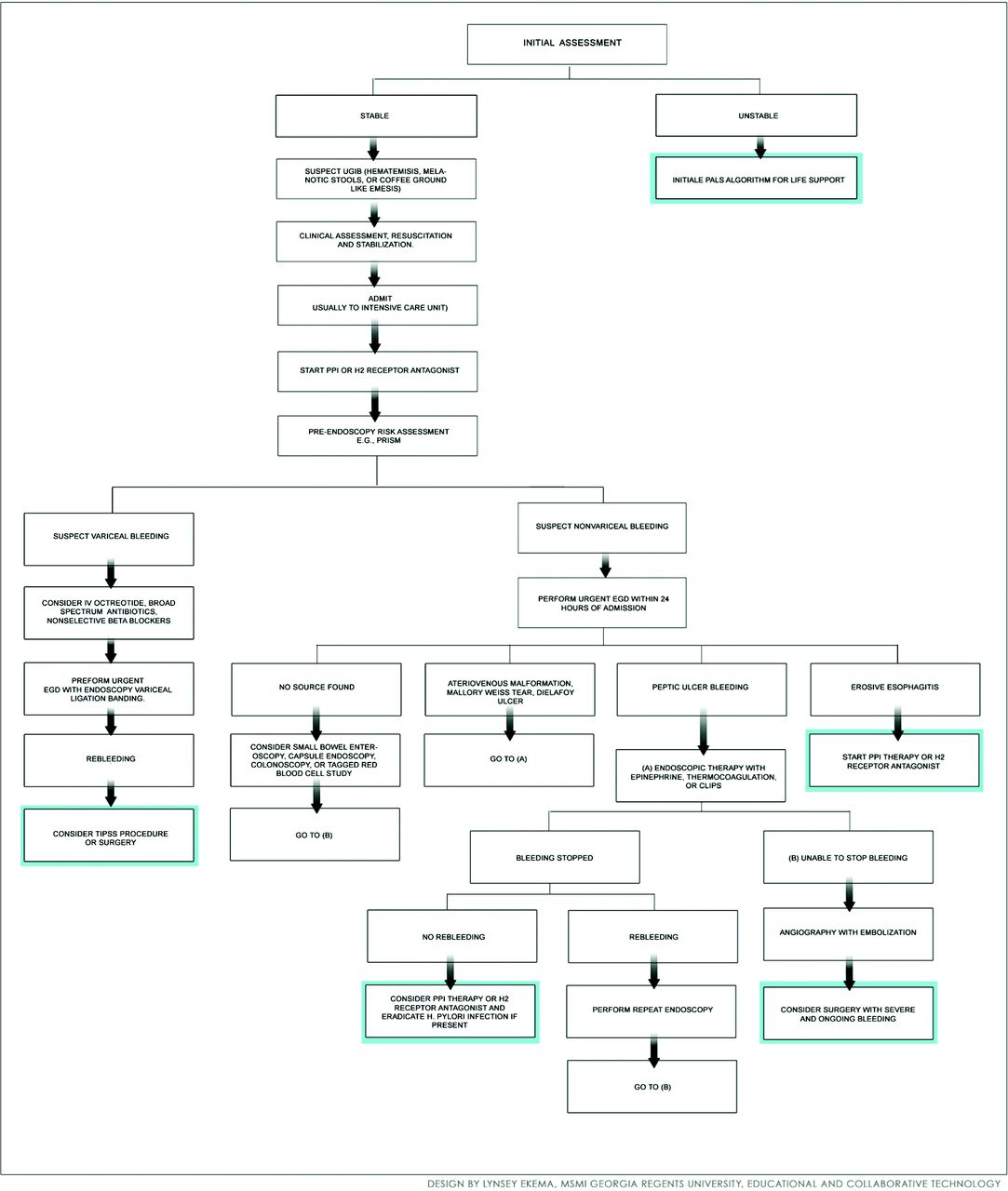
There are no randomized controlled trials or systematic reviews of the therapeutic approach to children with UGIB. Although many pediatric patients present with UGIB that is not hemodynamically significant, rapid assessment, stabilization, and resuscitation should precede diagnostic evaluation in unstable children. This includes assessment of the airway, breathing, and circulation.8 Patients with active bleeding that leads to hemodynamic compromise require intravenous access for fluid resuscitation and transfusion, as well as cardiopulmonary and urine output monitoring; they may also require intubation and mechanical ventilation for airway protection.8 Patients requiring emergent measures for survival should be transferred to a PICU (Figure 1). The pediatric physiology-based score for mortality (PRISM) can be used to assess the risk of mortality by taking clinical parameters and laboratory values into consideration.29 A score >10 (OR, 13.4) has been shown to be clinically significant for elevated mortality in the pediatric population.36

Algorithm for the approach to treating a child with upper gastrointestinal bleeding. EGD, esophagogastroduodenoscopy; H2, histamine 2; IV, intravenous; PALS, pediatric advanced life support; PPI, proton pump inhibitor; PRISM, pediatric physiology-based score for mortality.
Blood transfusion is appropriate for unstable patients and those with hemoglobin ≤8 g/dL.8 The amount of blood transfused should be determined according to age and weight.8 Children with active bleeding and coagulopathy should be considered for transfusion with fresh frozen plasma; those with thrombocytopenia should also be considered for platelet replacement, particularly when platelet count is <30,000.8 Considering starting a proton pump inhibitor, for example, omeprazole, in all children with UGIB is reasonable.8,24 Vasoactive drugs (eg, octreotide or vasopressin, broad-spectrum antibiotics, and nonselective β-blockers) can be added in children who are suspected of having variceal bleeding8 (Tables 8 and 9). Octreotide is preferred over vasopressin because it has improved efficacy and fewer side effects.34 Cytoprotective agents such as sucralfate and misoprostol have no role in the treatment of clinically significant UGIB in children.
A multidisciplinary team in a tertiary care center may be necessary to evaluate and manage children with UGIB. Consultation with pediatric intensivists, gastroenterologists, anesthesiologists, and surgeons may be required for patients with life-threatening bleeding.3 Endoscopic treatments include the application of clips, coagulation, banding, injection, sclerotherapy, and the use of tissue adhesives.8 A pediatric interventional radiologist or other specialist is needed if angiography is indicated when endoscopic therapy is unsuccessful.34 Children with bleeding that is not controlled with endoscopic or angiographic interventions should be evaluated for surgery34 (Figure 1).
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication May 15, 2014.
- Revision received October 9, 2014.
- Accepted for publication October 14, 2014.




{kind=link}