
Article Figures & Data
Figures
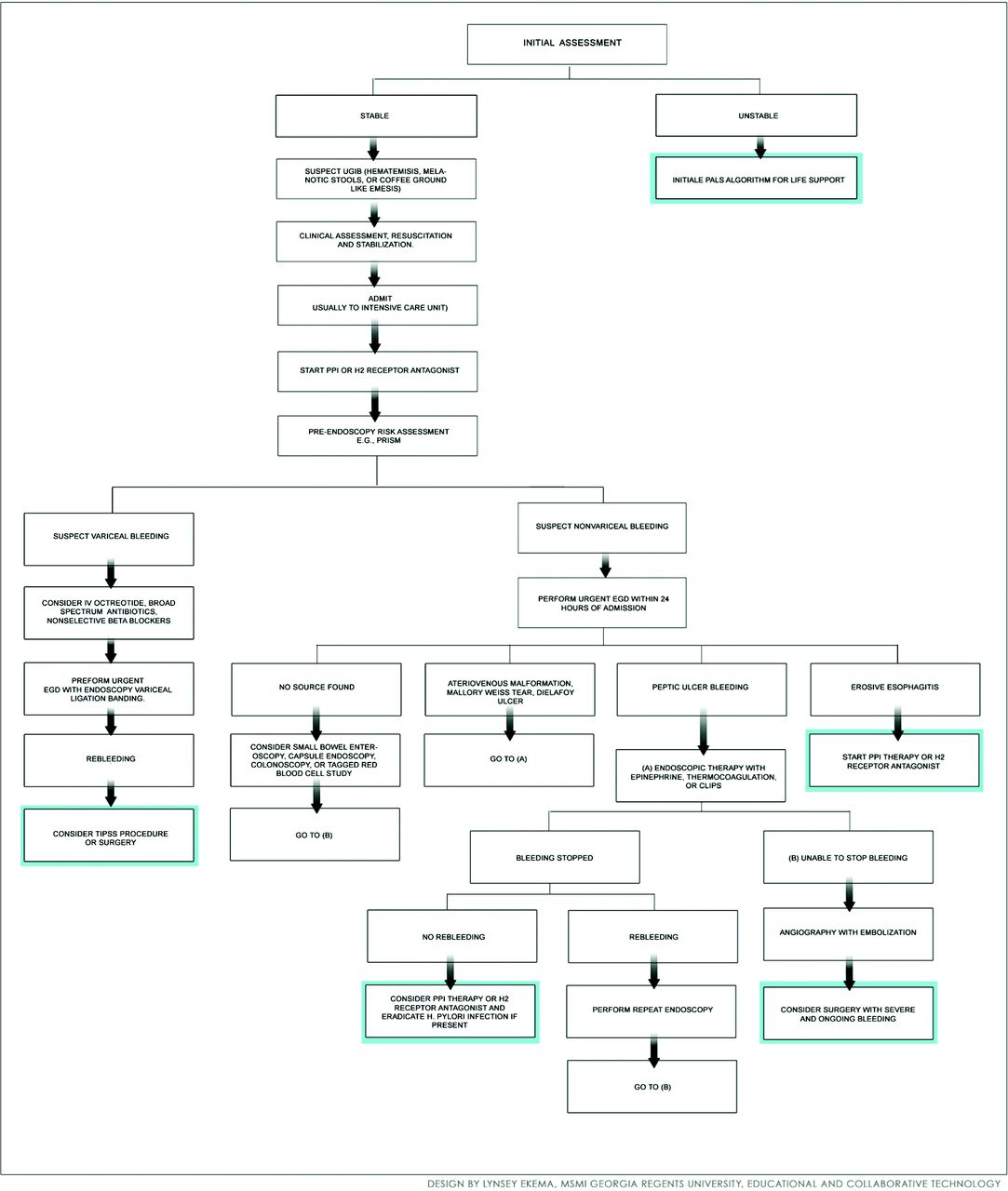
- Figure 1.
Algorithm for the approach to treating a child with upper gastrointestinal bleeding. EGD, esophagogastroduodenoscopy; H2, histamine 2; IV, intravenous; PALS, pediatric advanced life support; PPI, proton pump inhibitor; PRISM, pediatric physiology-based score for mortality.

Tables
Test Endoscopic versus Nonendoscopic Normal Result Comment Culture Endoscopic No growth Expensive and not widely available Fecal antigen test Nonendoscopic No antigen detected Useful before and after therapy; identifies active H. pylori Histologic biopsy Endoscopic No H. pylori identified Highly sensitive and specific Polymerase chain reaction Endoscopic No H. pylori identified Not widely available Quantitative and qualitative antibody testing Nonendoscopic Negative Not recommended after therapy Rapid urease test Endoscopic Negative Sensitivity reduced in patients after treatment Urea breath test with 13C and 14C Nonendoscopic Negative Useful before and after therapy Age Group Etiology Neonate Swallowed maternal blood Gastritis Necrotizing enterocolitis Coagulopathy in the presence of infection Congenital coagulation deficiency Esophagitis Vascular malformation Hemorrhagic disease of the newborn Idiopathic 1 Month-1 year Peptic ulceration Curling ulcer Duplication cyst Foreign body Gastric or esophageal varices Vascular malformation Bowel obstruction Epistaxis Hemoptysis Reflux esophagitis Stress gastritis Medication-induced gastritis (eg, NSAIDs or aspirin use) Caustic ingestion 1–5 Years Peptic ulceration Stress gastritis Medication-induced gastritis (eg, NSAIDs or aspirin use) Varices Epistaxis Hemoptysis Mallory-Weiss tear Gastroesophageal reflux Caustic ingestion Bowel obstruction Vasculitis Crohn disease Hemophilia 5–18 Years Varices Peptic ulceration Coagulation disorders Immune thrombocytopenic purpura Chemotherapy Crohn disease H. pylori gastritis Gastroesophageal reflux Mallory-Weiss tear Caustic ingestion NSAID, nonsteroidal anti-inflammatory drug.
Age Heart Rate (beats/min) Respiratory Rate (breaths/min) Newborn 120–160 30–60 1–6 Months 120–150 30–50 7–12 Months 110–140 25–40 1–3 Years 90–130 20–30 4–5 Years 85–120 20–25 6–12 Years 70–100 16–22 13–18 Years 60–80 12–18 - Table 5. Laboratory Tests in the Workup of Upper Gastrointestinal Bleeding in Children1,29–31
Test Description Normal Results Comments Complete blood count Peripheral whole-blood sample for hemoglobin, hematocrit, and platelets Age Values in Males (g/dL) Values in Females (g/dL) Requirement for transfusion is based on a patient's underlying illness and overall clinical presentation. Ranges may vary by institution or laboratory. Newborn 13–22 13–22 1–24 Months 9.5–14 9.5–14 2–10 Years 11.5–14.5 11.5–14.5 10–17 Years 12.5–16.1 12–15 Adults 13.5–18 12.5–16 Hemoglobin: Age Values in Males (%) Values in Females (%) Newborn 45–67 45–67 1–2 Months 31–55 31–55 2–3 Months 28–42 28–42 3–6 Months 29–41 29–41 6–24 Months 33–39 33–39 2–10 Years 34–45 34–45 10–17 Years 37–49 37–49 Adult 41–53 36–46 Hematocrit: Age Values in Males (g/dL) Values in Females (g/dL) Newborn to adult 140–450 × 109/L 140–450 × 109/L Platelets: Chemistry profile Age (Years) Values in Males (U/L) Values in Females (U/L) Elevated liver enzymes may indicate underlying liver disease. 0–5 35–140 20–93 6–3 20–60 20–93 4–6 15–50 16–61 7–9 14–40 15–40 10–11 10–60 10–40 12–15 15–40 5–30 Aspartate transaminase: Age Values in Males (U/L) Values in Females (U/L) 1–7 Days 20–54 21–54 8–30 Days 24–54 22–46 1–3 Months 27–54 26–61 4–6 Months 27–54 26–61 7–12 Months 26–59 26–55 1–3 Years 19–59 24–59 4–6 Years 24–49 24–49 10–11 Years 24–49 24–44 12–13 Years 24–68 24–44 14–15 Years 24–59 19–44 16–19 Years 24–54 19–49 Alanine aminotransferase: Age Values in Males (U/L) Values in Females (U/L) 1–30 Days 16–450 16–450 1–3 Months 16–267 16–267 3–5 Months 16–167 16–167 5–8 Months 8–84 8–84 9 Months to 17 years 5–55 5–55 >17 Years 15–85 5–55 γ-Glutamyl-transferase: Age Values in Males (mg/dL) Values in Females (mg/dL) 1 Month to adult 0.2–1.2 0.2–1.2 Total bilirubin: Age Values in Males (mg/dL) Values in Females (mg/dL) A BUN-to-creatinine ratio >30 has excellent specificity (98%) and good sensitivity (68.8%) for UGIB. 0–3 Days 0.2–1 0.2–1 4 Days to 2 years 0.2–0.5 0.2–0.6 2–4 Years 0.3–0.6 0.2–0.7 5–7 Years 0.2–0.7 0.2–0.8 8–10 Years 0.3–0.8 0.3–0.9 11–12 Years 0.3–0.9 0.3–1 13–17 Years 0.3–1.1 0.3–1.2 >17 Years 0.3–1.1 0.5–1.3 Creatinine: Age Values in Males (mg/dL) Values in Females (mg/dL) 0 Days to adult 6–17 6–17 BUN: Coagulation studies Venous sample from citrated tube for PT/INR, PTT PT: 11–15 sec INR: 1
PTT: 25–35 secProlonged PT/INR or PTT may indicate preexisting coagulopathy, liver dysfunction, or acute illness such as sepsis or disseminated intravascular coagulation. BUN, blood urea nitrogen; INR, international normalized ratio; PT, prothrombin time; PTT, partial thromboplastin time; UGIB, upper gastrointestinal bleeding.
- Table 6. Ancillary Tests in the Workup of Upper Gastrointestinal Bleeding in Children1,12,29,31,33
Test Description Normal Result Comments Angiography Arterial contrast study No extravascular extravasation of dye Has an overall good diagnostic rate of 64% but has better diagnostic accuracy in acute UGIB (71%) compared with chronic or recurrent UGIB (55%). Apt-Downing test Stool specimen from neonate Negative Important to distinguish between maternal and neonatal blood. Endoscopy Fiber-optic visualization of esophageal, gastric, and duodenal mucosa No bleeding sites noted; no varices Urgent endoscopy is indicated for bleeding requiring transfusion or hemodynamic instability; otherwise endoscopy can be performed within the first 24 hours of admission. Gastric aspirate Aspirate from nasogastric tube No blood detected Place nasogastric tube for gastric lavage to improve the accuracy of endoscopy. Consider testing gastric aspirate for occult blood using Gastrocult (Beckman Coulter, Inc., Palo Alto, CA). Stool for occult/frank blood (eg, hemoccult) Stool specimen from rectal examination Negative Alpha guaiaconic acid reacts with hydrogen peroxide in the presence of heme and produces a blue quinone compound. This denotes a positive test. UGIB, upper gastrointestinal bleeding.
Recommendation SORT† Reference Consider repeat esophagogastroduodenoscopy in children with either ongoing UGIB or rebleeding C 28 Distinguish between variceal and nonvariceal bleeding C 8 Initiate proton pump inhibitors or histamine 2 receptor antagonist in children with suspected UGIB C 8 Stabilize children with UGIB before diagnostic testing C 8 Complete urgent esophagogastroduodenoscopy as the diagnostic procedure of choice in children with suspected UGIB C 28 ↵† Strength of recommendation taxonomy (SORT) taken from ref. 47.
UGIB, upper gastrointestinal bleeding.
- Table 8. Pharmacologic Therapies in the Treatment of Upper Gastrointestinal Bleeding11,37–40
Name Dosage Indication Contraindication Comments Fluid resuscitation Lactated Ringers or normal saline: 20 mL/kg boluses for <5 min, for total of 80 mL/kg in the first 20 minutes; in patients with cardiac insufficiency, dose 5–10 mL/kg bolus Hemodynamic instability Congestive heart failure Obtain 2 large-bore IV lines.
Place a Foley catheter to monitor urine output.
If poor response, use crystalloid solutions; consider colloid solutions, such as albumin or plasma, and place intraosseous access immediately.Proton pump inhibitors Omeprazole: 1 mg/kg/24 hr by mouth in 1 or 2 divided doses or IV once daily; reported effective range: 0.2–3.5 mg/kg/24 hours Duodenal or gastric ulcer; stress gastritis
Prophylaxis is an off-label indicationDrug hypersensitivity Children 1–6 years old may require higher doses because of enhanced drug clearance.
PPIs have a longer duration of action than H2 receptor antagonists.
Limited safety and efficacy information in children.
Duration of therapy is unknown.H2 receptor antagonist Ranitidine:
Oral: 2–4 mg/kg BID
IV or IM: 2–4 mg/kg/day divided and administered every 6–8 hours
Maximum dose: 50 mg every 6–8 hoursDuodenal or gastric ulcer; stress gastritis
Prophylaxis is an off-label indicationNo absolute contraindications Duration of therapy is unknown. Vasoactive drug Octreotide: 1 μg/kg IV bolus, followed by infusion 1to 2 μg/kg/hour Variceal bleeding is an off-label indication No absolute contraindications No randomized controlled trials on use in children β-Blockers Propranolol:
Oral: 0.5–2 mg/kg/day in 2–4 divided doses, with the goal of reducing heart rate to 75% of baselinePortal hypertension and esophageal varices are an off-label indications Asthma, atrioventricular block, bradycardia, cardiogenic shock, sick sinus syndrome A meta-analysis found that combining endoscopic therapy and β-blockers reduced overall rebleeding more than endoscopic therapy alone or β-blocker use alone in patients with cirrhosis and bleeding esophageal varices. BID, twice a day; H2, histamine 2; IM, intramuscular; IV, intravenous; PPI, proton pump inhibitor.
Name Description Indications Complications Injection therapy Injection of solutions including hypertonic saline with epinephrine, normal saline with epinephrine, thrombin in normal saline, and ethanol Variceal and nonvariceal bleeding Tachycardia, cardiac arrhythmias, hypertension Thermocoagulation Heater probe; monopolar, bipolar, and multipolar coagulators Variceal and nonvariceal bleeding Heat-related mucosal injury, bleeding, or perforation
May have delayed hemorrhage from site of therapy for up to 4 weeksLaser photocoagulation Argon and neodymium:yttrium-aluminum-garnet lasers Variceal and nonvariceal bleeding Very expensive equipment; not widely used outside of specialized endoscopy centers Hemostatic clips Endoscopically placed clips that are deployed at the site of the bleed Variceal and nonvariceal bleeding Bleeding and perforation; clips can migrate off site of bleed, although rarely Endoscopic band ligation Use of elastic bands on bleeding lesion Variceal bleeding and Dieulafoy lesions Postprocedural pain, ulceration, secondary hemorrhage
Retrospective study stated that 27% of patients had rebleeding after band ligation and 1% had esophageal perforationAdhesive closure with N-butyl-cyanoacrylate Injection of tissue adhesive Variceal bleeding, especially for gastric varices Rebleeding, sepsis, arterial embolization (rare) Transjugular intrahepatic portosystemic shunt Tract created within the liver using radiographic guidance to connect 2 veins Biliary atresia, variceal bleeding Limited data and experience in children Surgical shunt placement Attachment of autologous or synthetic vein to vein Bleeding is uncontrolled by therapeutic endoscopy and angiography Loss of shunt patency, repeat procedures Balloon tamponade Balloon inflated at the site of bleeding Uncontrolled UGIB Limited experience in children; should not be used for more than 24 hours UGIB, upper gastrointestinal bleeding.




{kind=link}