
Abstract
Objective: The objective of this study was to describe French primary care physicians' beliefs about cardiovascular disease (CVD) risk factors and best practices for managing CVD.
Methods: This study comprised a purposive convenience sample of 656 primary care physicians in France, recruited from contacts made through the French Society of General Medicine. We compiled the physicians' responses to free text questions taken from an Internet-based survey and analyzed them using a qualitative approach. Physician's responses were inductively analyzed using content analysis. Responses were thematically coded, tabulated, and computed for frequencies. Overall themes and verbatim examples are presented in this article.
Results: The French physicians in our study are generally happy with their country's health care system and cite equity as the primary reason. Interestingly, along with food and lifestyle differences, they also cite equity of their health system as the reason for the lower CVD death rate in France, Japan, and Israel compared with the United States. The physicians believe that they are successful at managing CVD risk factors by emphasizing aspects of the doctor–patient relationship, including spending more time with patients and focusing on education.
Conclusions: Physicians who are on the front line of care and management offer a fresh perspective on best practices for CVD prevention and management. The equity of the French health care system supports a “culture of care” in France that might lead to better outcomes for CVD risk factor patients than in the United States.
- Cardiovascular Abnormalities
- Cross-Cultural Comparison
- Delivery of Health Care
- France
- Physician Patient Relationship
- Quality of Health Care
Cardiovascular disease (CVD) is the leading cause of death globally, accounting for 17.3 million deaths annually.1 Rates of death caused by CVD are lower in France than they are in the United States despite that the distribution of traditional CVD risk factors such as hypertension, diabetes, and smoking is surprisingly similar in France and the United States.2⇓⇓⇓⇓–7 French CVD mortality rates are 35% lower for men and 32% lower for women compared with American rates.1 The reason for this difference in mortality rates has not been fully explained. A recent survey of French physicians suggests that there may be a culture of care for CVD risk factor management in France that could support better patient outcomes.8
A healthy diet and moderate wine consumption are often cited as the primary reasons for France's low incidence of CVD mortality.9⇓–11 Indeed, cultural differences in lifestyles and underlying social, environmental, and economic factors have been shown to have a strong influence on health outcomes.12,13 The average French person exercises more, eats more fruits and vegetables, and works less than an average American.14⇓⇓⇓–18 Furthermore, food is central to French culture and French dietary habits include sit-down dinners with family and smaller portion sizes.10 However, that the French may follow healthier dietary and lifestyle habits than the typical American and have lower rates of obesity may not entirely account for the lower CVD mortality in France.
Considerable differences exist between health care systems and physician practice behavior in the United States and France that could contribute to France's lower CVD mortality.19,20 In 2000, the French health care system was ranked the best in the world versus the US system, which ranked 37th.21 Surprisingly, the French spend on health care roughly half of the money that the United States spends.2 The latest figures show health expenditure per capita in France is 49% lower than in the United States.1 Most French citizens are fully covered under a national health care system, whereas according to the US Census Bureau, 50.7 million Americans, an all-time high, are uninsured.22 Universal coverage in France results in less disparity, and research has proposed that the French health care system may allow physicians and patients more flexibility to adopt professional and culturally pertinent approaches to the management of CVD risk factors.8 These practices include patient-centered care such as building doctor–patient relationships and using electronic medical records (EMRs), which have documented positive effects on improving the process of care and, more recently, on clinical outcomes.23⇓⇓⇓–27 A cross-cultural comparative study focusing on the opinions and practices of French and US physicians found considerable differences between the United States and France.8 The study focused on the microsystem of the office, which includes patients, clinicians, and cultural processes.28 French physicians reported that they focus more of their treatment efforts on lifestyle modification rather than medication management, see their patients more frequently and for longer visit times, use EMRs more often, and have guidelines more readily available to them than American physicians.8
These processes of care and their contribution to the management of CVD in particular have not been explored adequately and could provide insight into a culture of care practiced by French physicians that may contribute to better cardiovascular health in France.29 Physicians are on the front line of patient care, yet few if any studies have been conducted that describe their beliefs about CVD and the best ways to prevent and treat CVD. Physician's beliefs and opinions about CVD risk factor management offer a fresh perspective on CVD prevention and management.
Methods
Design and Setting
Informal interviews with a convenience sample of 25 primary care doctors in the United States, France, Japan, and Israel were conducted to gather background information about how physicians manage CVD risk factors in the outpatient setting in their respective countries. An online survey was created based on the informal interviews. The resulting survey used a mixed methods design of quantitative and qualitative data, including 45 multiple choice questions and 3 “free text” questions.30 The inclusion of free text questions provided qualitative data from which to draw themes. Reported here are the results of the French physicians' responses to the free text questions. Because qualitative data can elucidate and provide further explanation of quantitative data, in certain cases we will reference the physician's multiple choice responses to compare them with their free text responses.31
Recruitment and Sampling
Participants were sampled purposively to include primary care physicians, most of whom were family and general practitioners. Purposive sampling targets participants based on preselected criteria relevant to the particular research questions.30 The French physicians were contacted via a convenience sampling method through the French Society of General Medicine, one of the main organizations of family physicians in France, whose membership includes 1200 practicing physicians from across the country. The survey was E-mailed to all members of the French Society of General Medicine. A total of 656 French physicians returned the survey. Eighty-eight percent of responding physicians were between the ages of 35 and 64 years, with an average age of 50 years. The vast majority of respondents (97%) were family or general practitioners.
Ethical Approval
The study was approved by the Institutional Review Boards of Wright State University and the University of Georgia. An informational letter about the project accompanied the email survey. As an incentive, physicians received three hours of continuing medical education credit for completing the survey. Physician consent was secured through participation in the study.
Data Collection
The physicians were asked their opinion about the reason for lower CVD death rates in France, Japan, and Israel than in the United States, the quality of health care in their country, and reasons that they believe that they are successful managing patients with CVD risk factors. The participants typed their responses directly into the web-based survey, and these responses were collated into a spreadsheet for analysis.
Data Analysis
Answers to the free text survey questions were coded into response categories by the research team, which was led by a cultural anthropologist (COBC) with expertise in qualitative analysis. The codes were generated using word repetition and key words in context methods to identify repeated words and themes.32 A code book was developed based on key words and themes, which were discussed by members of the research team, and refinements and changes were made. Two native French speakers coded the physicians' responses. The responses were kept in their original language during the coding process to decrease the likelihood that meaning would be lost or changed during the process of translation.30 To assure consistency in code assignment, a test of intercoder reliability (between the 2 coders) was performed using a sample of responses from each of the 3 survey questions to ensure that the coders were interpreting the data and assigning codes in a similar manner. Two reliability tests were performed between the coders, with an intercoder reliability score of 90% or greater for each test, which is an adequate level of intercoder reliability.33 Because many responses contained several themes, coders could assign multiple codes rather than only one for each response, per the method of Carey.34 During the data analysis, the research team met regularly to discuss the range of answers and any new codes that were generated when emergent themes were discovered. When new themes emerged, the team discussed the new proposed code and either rejected it or adopted it into their coding process. The team determined that assigning up to 3 codes per response was sufficient to cover the range of topics included in physician's responses. Since the creation of the codes was part of the analysis, the final code book for each question is presented in Table 1.
Results
Differences in CVD Death Rates
When responding to the statement, “The cardiovascular death rate is 20% to 25% lower in France, Japan and Israel versus the United States because…,” 53% of the physicians cited food, diet, and portion sizes as the most important factor in the difference in CVD death rates (see Table 2). One physician stated that lower CVD “seems related to overall eating habits in our country [France], reinforced by media campaigns.” Physicians stated that in France, food portions are reasonable, nutritious, more diversified, and have fewer calories and less sugar than the American diet. French physicians also mentioned cultural aspects of the French diet, stating that “in France we are still protected from junk food.” Meals with family and the Mediterranean diet, which emphasizes fruits, vegetables, and lean protein, are valued by the French overall. Physicians repeatedly used the word “balanced” when describing the French diet.
Second to food and diet, 22% of physicians cited greater equity of health care in France, Japan, and Israel than in the United States as a reason for lower CVD death rates. The code “equity” referred to fairness of the health system as well as coverage. One doctor stated, “Patients have better access to the medical system, which allows for prevention, including disadvantaged populations who are most affected.” Another physician commented, “Social protection allows better management of risk factors.” Several physicians stated that equity also referred to the cost of healthy food in the United States and that the low-income people living in the United States could not afford a healthy, balanced diet.
Twelve percent of physicians mentioned lifestyle as an important factor in higher CVD death rates in the United States. For this study's purposes, “lifestyle” included both stress and intensity of living. One physician noted that in France, “lifestyle [dietary, physical activity] is the opposite of what I witnessed during a trip to the [United States].” Interestingly, lifestyle was often linked to diet by the doctors. One explained the lifestyle/food connection like this: “People [in the United States] are so stressed they eat more food more often.” Other physicians simply stated that the French have a “better quality of life,” with less stress, and have more “healthy balanced living” than their US counterparts.
Opinions about the Health System
When responding to the statement, “Health care in my country is generally good or not good because…,” 71% of the physicians answered that health care in their country is good. The physicians most often cited health care equity, full coverage of medical expenses and medication, and comprehensive care as reasons that the French system generally is good. One doctor stated, “Access to care is still possible for all and free”; another said, “Everyone has access to care regardless of income, and critical care is equivalent for all.” One doctor commented that, “It is good in the field of management of [CVD] because with virtually free health care we can take time to give advice, review and repeat recommendations, and explain the influence of factors like weight and other therapeutic interventions for each patient.”
Successful Practices for Managing CVD
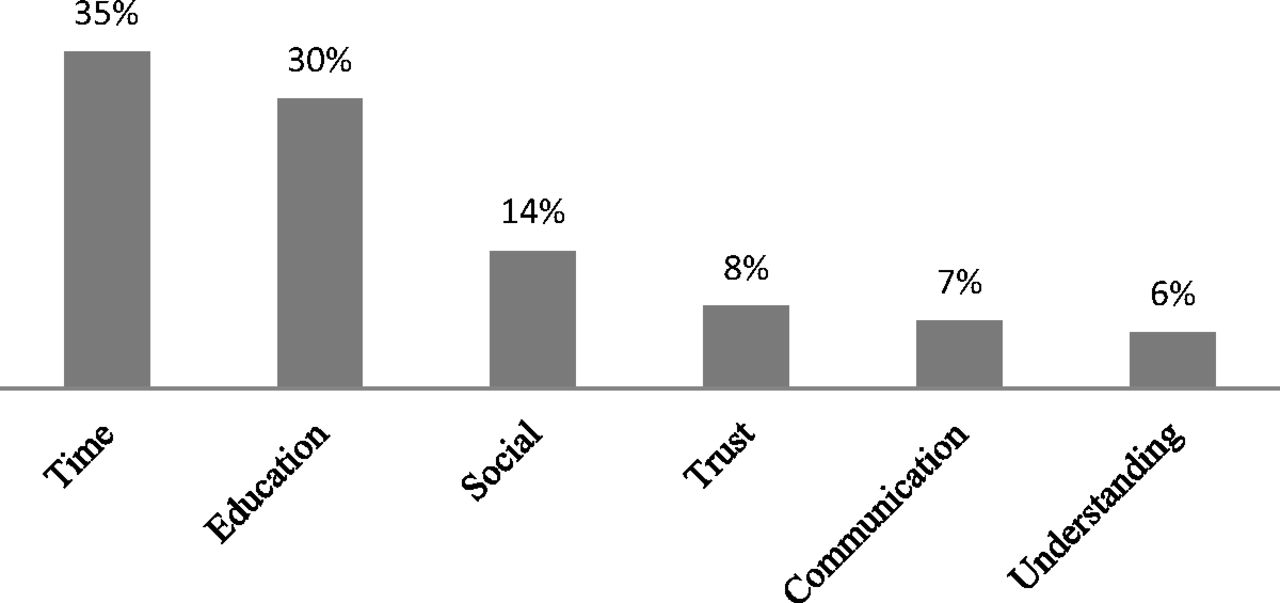
When responding to the statement, “I believe I am successful at managing patients with CVD risk factors because…,” 51% of physician's answers concerned the doctor–patient relationship. The subthemes included in the doctor–patient relationship (see Table 3 and Figure 1) were trust, communication, understanding, education, social, and time aspects of the visit. Physicians named “time” and “education” as the most important of these items. The “time” code included statements about the length of time that the doctor and patient have been in the relationship and the amount of time spent with a patient during an office visit. These 2 aspects of time were combined because physicians generally referred to “time spent with patients” in their responses without differentiating between consultation time, frequency, or continuity of care. The “education” code included explanation of the biology or diagnosis of a disease to the patient and treatment explanations and suggestions. One physician stated, “[I] take the time to explain,” and several of the physicians' comments stressed the importance of the time they spent on educational diagnoses. Another physician claimed, “I am convinced that educating patients with cardiovascular risk is the foundation for the preservation or improvement of their health.” One said that they use visuals that explain and educate the patient about the pathophysiology and other technical knowledge. Another physician referred to their “power of persuasion” when spending time educating a patient. Time adjustments for particular patients were seen as important as well. One physician attributed their success to “longer consultation time with patients at high risk.”

Key subthemes in the doctor–patient relationship.
“Social” aspects of the doctor–patient relationship were commented on by the physicians. The social code includes that the doctor is aware of patients' family, financial, work, and life goals and cultural context. The physicians referred to this as “contextual knowledge” of the patient's life. One physician stated that “the direct relationship and good knowledge of the patient, his confidence, and loyalty” were the most important factors of their success. Another explained, “Listening to the patient's wishes, his life goals” is important to their success in treating CVD. Another physician stated the importance of a “personalized approach to address the problems of each patient by listening, explaining, negotiating.” One physician contended that one of their strengths is “the ability to vary the treatment of hypertension, according to the patient's personality, his attitude, and his compliance.”
Trust, which includes bilateral respect and shared responsibility, was commonly commented on by doctors. One physician stated that “patients' confidence in their [General Practitioner]” is important. Another claimed that “confidence, faith, and empowerment” are all important factors in treatment success.
“Communication” and “understanding” were important parts of the doctor–patient relationship as well. Communication includes nonverbal and verbal communication as well as listening. Understanding is seen as mutual between doctor and patient. One physician stated that it is necessary to provide “simple explanations and clarifications.” Another physician stated that they “listen carefully to life goals and constraints and [invest] time in the explanations of the nature of the condition.” One physician adapts communication styles to the patient, for example, by using agricultural imagery to explain hard to understand health concepts to a farmer.
Other key aspects of their success at managing patients with CVD risk factors include doctor knowledge (16%), motivation (14%), and use of guidelines or recommendations (14%). Doctor knowledge includes continuing medical education, medical meetings, literature, peer group learning, postgraduate training, and clinical guidelines. Motivation includes the personal conviction, persistence, and commitment of the doctor. Examples of motivation given by the physicians include strong personal involvement and commitment, setting benchmarks, and personal interest in changing patient behavior. One physician described this as a “strong personal commitment to preventive medicine.” Physicians described the importance of guidelines in terms of physician knowledge about them and in general the existence of and compliance with official recommendations to assist with treating patients according to their disease and age and to assist with setting systematic goals for therapy.
Discussion
Physicians cited the healthier food and diet of the French as the most important reason for CVD disparities. However, nearly one quarter of the doctors also cited equity—specifically discussing France's equitable system and the United States' inequitable system—as a key reason for the United States' higher CVD mortality. Equity in France is reflected in universal coverage and low patient costs. Often these differences in equity and coverage are overshadowed by the food, diet, and lifestyle arguments to explain France's lower CVD rates, even though health care coverage and quality of care play a key role in CVD outcomes. For example, adequate patient coverage and access to care allow physicians to better manage CVD risk factors through close monitoring and provide them with more opportunities to educate and equip the patient with preventive tools.
Another key difference between the US and French health care systems is France's use of tools that lessen the administrative burden on physicians. Indeed, French doctors report spending more time in patient care than American doctors, who report spending more time on administrative activities.8 The French carte vitale maintains the patient's information in one place and facilitates the communication with the health insurance companies. EMRs are used to store and monitor patients' clinical data but together with the carte vitale, they also are able to send the payment fee to the health insurance companies without any paperwork. These tools may allow French doctors more time to spend with patients dealing with important issues, such as listening to their concerns or educating them about CVD prevention.
Physicians cite the use of guidelines as a successful practice for managing CVD risk factors. French physicians have guidelines available to them in the examination room when seeing patients, which could promote their consultation during a patient examination.8 Knowledge about guidelines and expertise and training were cited by doctors as an important factor in their success with patients as well. The fact that doctors regularly update themselves on new clinical guidelines and seek out peer group learning opportunities may be closely linked to their own motivation. The personal conviction and tenacity that they cite in their responses is an important component of their self-reported success. That 71% of the physicians in our study reported that the health care system in France is good may augment their motivation in practice.
The 2 things that the physicians liked most about the French health care system are equity and comprehensive care, including financial coverage and support for patients. Perhaps it is these features of the health care system that allow French physicians to build and maintain an ongoing long-term relationship with their patients, which in turn may allow for more preventive care and the early diagnosis of CVD risk factors.14 Patient-centered communication and continuity of care lead to increased trust between physicians and patients.35 The French physicians in this study emphasize social aspects of the doctor–patient relationship, including time, trust, and education as being the most important factors in their success with managing patients with CVD risk factors. It is the social information about their patients, such as a patient's personality or motivation, that allows doctors to “tailor” treatment to their patient's individual goals or needs. Furthermore, the issue of time (both continuity of care and visit length) is important in establishing and maintaining patient-centered care and developing the physician–patient relationship based on the principle of trust.36⇓⇓–39
Figure 2 depicts several French best practice points for CVD risk factor management as identified by the physicians in this study. These include doctor–patient relationship, motivation of the doctor, doctor knowledge, use of guidelines, use of EMRs, and focus on prevention/healthy lifestyle. Together, these key practices comprise a culture of care in France.

Best practices comprising a “culture of care” for French cardiovascular risk factor management. EMR = electronic medical records.
The question remains, Could these best practices of the culture of care in France be adopted in the United States? Social aspects of the doctor–patient relationship, including time, trust, and education, are valued in US medicine but the American system does not allow doctors to focus on it fully, especially because the typical office visit has increasingly more items competing for the attention of the physician.39,40 Limited time for office visits would require physicians in the United States to reallocate their time to emphasize preventive lifestyle modifications. Using EMRs and practice guidelines could facilitate this process by improving process outcomes and lessening administrative tasks, resulting in increased time for physicians to focus on education, lifestyle modification, and social aspects of the doctor–patient relationship.
Strengths and Limitations of the Research
Physicians in this study were drawn from the French Society of General Medicine membership lists, which include 1200 physicians. Therefore, membership is a limiting factor in how they were selected to respond to the survey. The data reflects physician self-reports of behavior, which may not accurately reflect true behavior.41 Qualitative analysis of text responses represents the beliefs and opinions of our sample but does not represent the beliefs and opinions of all practicing primary care physicians in France. An observational study is needed to validate the survey results. The goal of this research was to provide a descriptive account of physician beliefs and opinions, and as such, we do not attempt to correlate reported practices with better outcomes in France. However, through this descriptive account we have identified French practices in CVD management that can serve as a starting point for future research efforts.
Conclusions
It is clear that physicians agree with current research that the American diet and portion size are primary contributors to the United States' higher rates of CVD. However, this study has moved beyond the prevailing themes to uncover attributes of the culture of French cardiovascular care that need to be explored further. Many questions remain, including, Could French physician's emphasis on lifestyle management and patient-focused care rather than on medication management account for their success? Is the French physician's willingness to focus on the doctor–patient relationship because of patient continuity, which increases trust and comfort when discussing sensitive issues, or are there other cultural differences in the way that physicians are trained in France that differ from the training of US physicians? Will the transition to EMRs in the United States provide process improvements that will allow American physicians to shift their focus away from administrative concerns and more toward patient-centered care? and, Ultimately, could the adoption of practices of the French culture of care improve CVD outcomes in the United States? As health care reform in the United States is implemented, physicians will be faced with new challenges of how to manage a tidal wave of newly insured patients. The ability to respond to these challenges by adopting systems changes could have profound effects on the culture of CVD care in the United States.
Notes
This article was externally peer reviewed.
Funding: Foundation funding was provided by Mr. Oscar Boonshoft.
Conflict of interest: none declared.
- Received for publication January 20, 2012.
- Revision received January 23, 2012.
- Accepted for publication January 27, 2012.




{kind=link}
{kind=link}