
Abstract
Patients with type 2 diabetes mellitus are usually treated initially with oral antidiabetic agents, but as the disease progresses, most patients eventually require insulin to maintain glucose control. Optimal insulin therapy should mimic the normal physiologic secretion of insulin and minimize the risk of hypoglycemia. This article discusses the role of insulin therapy in patients with type 2 diabetes, emphasizing long-acting insulin agents designed to approximate physiologic basal insulin secretion and provide control over fasting plasma glucose. Clinical trials of recently developed long-acting insulins are reviewed herein, with emphasis on studies that combined basal insulin with oral agents or with short-acting insulins in a basal-bolus approach. The normal physiologic pattern of insulin secretion by pancreatic β cells consists of a sustained basal insulin level throughout the day, superimposed after meals by relatively large bursts of insulin that slowly decay over 2 to 3 hours (bolus insulin). Basal support with long-acting insulin is a key component of basal-bolus therapy for patients with diabetes who require insulin with or without the addition of oral agents. Newer long-acting agents such as insulin glargine provide a steadier and more reliable level of basal insulin coverage and may have significant advantages over traditional long-acting insulins as part of a basal-bolus treatment strategy.
Understanding the pathophysiology of type 2 diabetes mellitus and determining optimal management strategies are critical health care priorities because of the high morbidity and mortality associated with the disease.1 The treatment goal for all patients with diabetes is to prevent its short- and long-term complications. The microvascular complications traditionally associated with long-term diabetes are retinopathy, nephropathy, and neuropathy. However, macrovascular complications (eg, coronary heart disease, stroke, myocardial infarction) are the major cause of disability and death in diabetes patients.2 Although data on the effect of glucose control on macrovascular complications remain equivocal, results from the United Kingdom Prospective Diabetes Study Group (UKPDS) showed that tight control of blood glucose in patients with type 2 diabetes was associated with a 25% reduction in development of all microvascular complications combined.3 Although no data exist in patients with type 2 diabetes, the Diabetes Control and Complications Trial also showed, with intensive glucose control, a significant decrease in the progression of microvascular complications.5
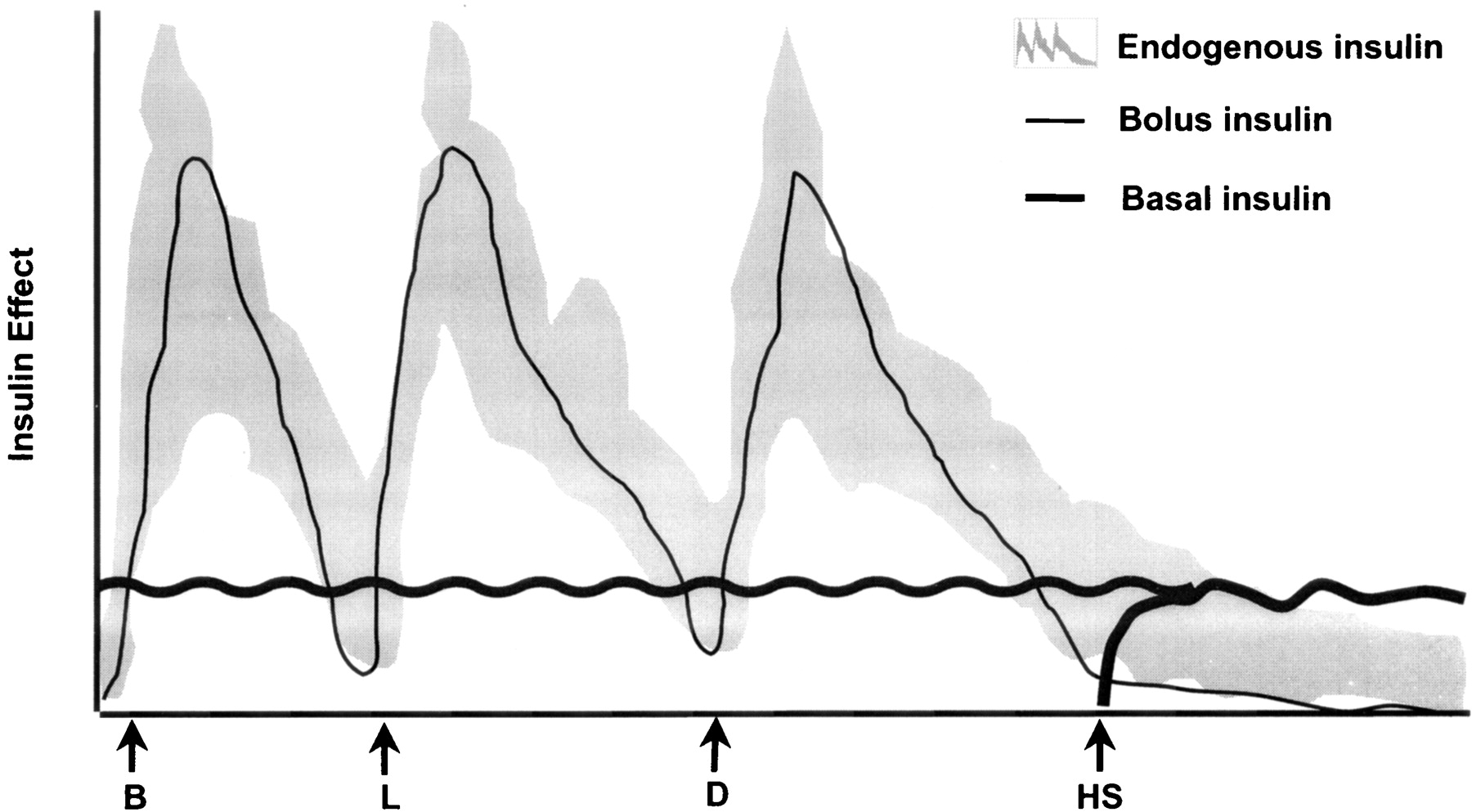
Treatment mimicking the normal physiologic pattern of insulin secretion may be an optimal way to achieve tight blood glucose control in patients with diabetes. The key features of the physiologic pattern of insulin secretion by β cells are a meal-stimulated peak in insulin secretion that slowly decays over 2 to 3 hours and a sustained basal level that remains constant throughout the day (Figure 1). 6 These 2 components of physiologic insulin secretion are called bolus (food-related) and basal (non–food-related) secretion.6 Adequate basal insulin secretion is essential for glucose regulation in both the liver and the peripheral insulin target tissues (muscle and adipose tissue). Basal insulin secretion plays a key role in modulating endogenous glucose production from the liver, which is highly sensitive to small changes in insulin levels. The insulin rise that follows the ingestion of food stimulates glucose uptake in peripheral tissues and suppresses endogenous glucose production. These actions of insulin maintain plasma glucose levels within a fairly narrow range.7

Idealized pattern of insulin secretion for a healthy individual who has consumed 3 standard meals: breakfast (B), lunch (L), and dinner (D). HS, bedtime.6
Pathophysiology of Type 2 Diabetes
Type 2 diabetes results from an imbalance between insulin sensitivity in peripheral tissues and the liver and insulin secretion from pancreatic β cells. In the presence of insulin resistance (a reduction in the body’s ability to respond to insulin), the pancreas must synthesize more insulin to metabolize a given amount of glucose. Early in the disease, patients with type 2 diabetes have altered insulin secretory capacity. This secretory defect progresses over time, resulting in insufficient insulin production to maintain blood glucose control. Although the pathophysiology of this process has not been fully elucidated, hyperglycemia seems to have a toxic effect on β-cell function and may result in dedifferentiation of β cells8 or in apoptosis without a compensatory increase in β-cell proliferation.9 The loss of β cells and the resulting relative insulin deficiency leads to glucose intolerance and, finally, to overt diabetes.10
Targets for Glucose Control
The American Diabetes Association (ADA) has developed guidelines for managing patients with type 2 diabetes. The ADA Standards of Medical Care for Patients With Diabetes treatment goals for glycemic control are glycohemoglobin (hemoglobin A1c [HbA1C]), <7%; fasting plasma glucose (FPG), 90 to 130 mg/dL; and postprandial plasma glucose (PPG) <180 mg/dL.11 It may be important to control both FPG and PPG levels in patients with type 2 diabetes. Elevated FPG has been linked to mortality risk, and recent results suggest that PPG may also be closely correlated with the development and progression of disease complications.12
Oral Antidiabetic Therapy
Patients with type 2 diabetes are often treated first with diet and exercise. If glycemic control declines, pharmacological therapy with an oral agent (a sulfonylurea, metformin, a thiazolidinedione, an α-glucosidase inhibitor, or a non-sulfonylurea secretagogue) is typically initiated. If monotherapy fails, a second oral agent may be added. If glycemic control is not maintained with 2 agents, a third oral agent may be included.13,14 In time, however, oral agents fail to maintain glycemic control in most patients with type 2 diabetes.14 The progressive loss of β cells eventually requires the addition of exogenous insulin to maintain control. Results from the UKPDS indicate that 53% of patients initially assigned to treatment with a sulfonylurea required insulin therapy within 6 years of follow-up.15,16
Combination Therapy with Insulin
In many patients with type 2 diabetes, insulin is first used in combination with oral therapy. A number of insulin treatment regimens have been used in this setting, including neutral protamine Hagedorn (NPH) insulin and ultralente insulin (Ultralente; Eli Lilly and Company, Indianapolis, IN) administered at bedtime or twice daily, or a long-acting human insulin analog (eg, insulin glargine [Lantus; Aventis Pharmaceuticals, Inc, Bridgewater, NJ]) administered once daily.17 Recent data from clinical trials that studied the effects of adding insulin to oral therapy for patients with type 2 diabetes indicate that bedtime long-acting insulin injection significantly improved glycemic control.18–20The addition of insulin to the treatment of a patient for whom one or more oral agents have been unsuccessful typically produces a larger, more rapid reduction in HbA1C compared with the addition of another oral agent.21
Basal-Bolus Insulin Therapy
Ideal insulin regimens in patients with type 2 diabetes approximate the normal physiologic pattern of insulin secretion (Figure 1).6 The function of basal insulin in these regimens is to sustain plasma glucose control for approximately 24 hours. The first step in initiating basal-bolus therapy is to establish a dosing regimen based on the patient’s insulin needs, determined by physiologic glucose disposal characteristics (ie, glucose and HbA1C levels), as well as exercise and eating habits. These starting doses are then adjusted depending on the results of self–blood glucose-monitoring (SBGM). The timing of SBGM generally includes both fasting and postprandial glucose measurements, especially when treatment is first started and when therapeutic regimens are changed. Frequent SBGM helps patients identify problems with glycemic control and respond to these problems rapidly.6 Many different insulin combinations can be used for basal-bolus treatment, and their characteristics, advantages, and limitations are considered in the following sections.
Insulin Preparations
A wide range of insulin preparations has been used to treat patients with type 1 and type 2 diabetes. These include short-acting insulins (regular, lispro [Humalog; Eli Lilly and Company], and aspart insulin [NovoLog; Novo Nordisk Pharmaceuticals, Inc, Princeton, NJ]), insulins with an intermediate duration of action (NPH insulin and lente insulin [Lente; Eli Lilly and Company]), and long-acting insulins (ultralente insulin and insulin glargine).
Short-Acting Insulins
Short-acting insulins are used primarily to approximate the normal physiologic responses to meal consumption (ie, the bolus of insulin secretion). Short-acting insulins used for bolus therapy include regular, lispro, and aspart insulins (Table 1). Lispro and aspart are monomeric insulin analogs that are more rapidly absorbed and thus have a more rapid onset of action than regular insulin (5 to 15 minutes for lispro and aspart, respectively, relative to 30 to 60 minutes for regular insulin). In addition, monomeric insulin analogs have less interpatient variability and a decreased risk of hypoglycemia.6,22–26
Intermediate- and Long-Acting Insulins
Although short-acting insulin analogs have largely overcome the limitations of regular insulin for controlling postprandial hyperglycemia by reducing interpatient variability and risk of hypoglycemia, developing safe and effective longer-acting insulin analogs that approximate basal insulin secretion has been more challenging. Insulin preparations with intermediate durations of action, lente insulin and NPH insulin typically require twice-daily injection to achieve required basal insulin levels over 24 hours. These agents have relatively gradual onsets of action, with peak effects occurring between 4 and 8 hours after administration, but their pharmacokinetic and pharmacodynamic profiles exhibit substantial intrapatient and interpatient variability. The prolonged peak effects of these insulins may also overlap with those of short-acting preparations, resulting in hypoglycemia, particularly at night. Ultralente insulin has a longer duration of action than either lente insulin or NPH insulin. However, this preparation has also been associated with large day-to-day variability (<20 to >24 hours) and erratic peaks that may result in unpredictable hypoglycemia.6 The high variability in action of these longer-acting insulin preparations is generally believed to result from variability in the concentration of insulin in the suspension injected by the patient and from poor diffusion and absorption by capillaries at the injection sites.27 The limitations of these longer-acting insulin preparations have prompted the development of new insulin analogs that are much more effective in mimicking physiologic basal insulin secretion. The only currently available long-acting analog is insulin glargine.
Insulin Glargine
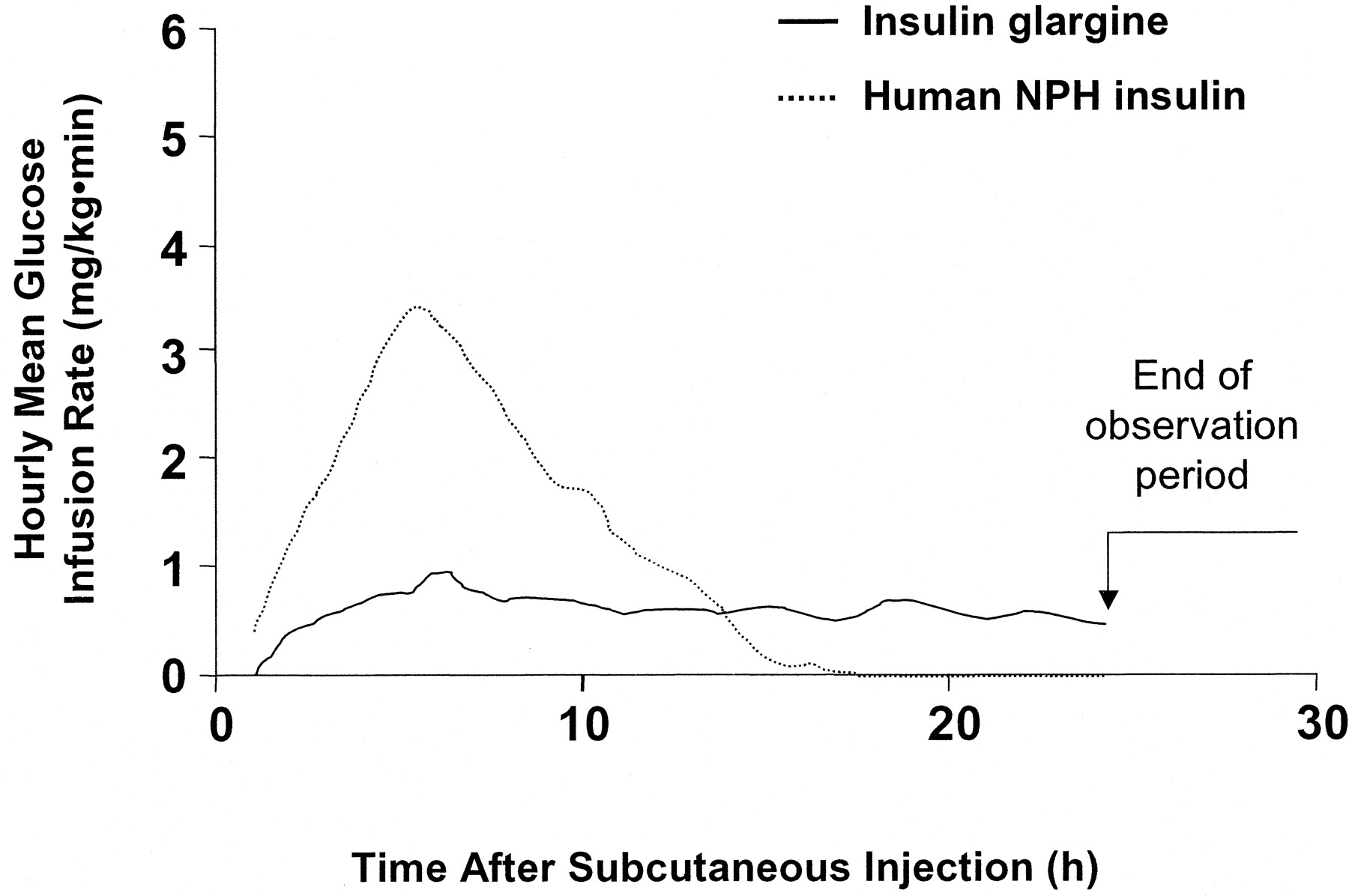
Insulin glargine is an extended-action insulin analog and was created by the recombinant DNA modification of human insulin. Alterations in the insulin molecule raise the isoelectric point and cause insulin glargine to precipitate at the injection site, thus slowing absorption. The pharmacodynamic profile of insulin glargine is characterized by the lack of a pronounced peak and a duration of action of approximately 24 hours (Figure 2, Table 1).6,24,28

Time-activity profiles (hourly mean values) of insulin glargine and NPH insulin in patients with type 2 diabetes.24
In controlled clinical trials, insulin glargine was compared with NPH insulin for improving glycemic control when combined with either oral therapy in patients with type 2 diabetes or with insulin lispro in patients with type 1 diabetes. In 426 patients with type 2 diabetes and poor glycemic control on oral drugs alone, Yki-Järvinen et al compared bedtime insulin glargine and NPH insulin, each with continued oral therapy. Both insulins significantly improved glycemic control (HbA1C and FPG) over 1 year of follow-up. There was significantly less nocturnal hypoglycemia with insulin glargine than with NPH insulin (9.9% vs 24.0%).19
Rosenstock et al conducted a similar comparison of insulin glargine and NPH insulin in 518 patients with type 2 diabetes. Both insulins significantly improved glycemic control, but insulin glargine was associated with a lower risk of nighttime hypoglycemia than was NPH insulin (26.5% vs 35.5%). Patients treated with insulin glargine in this study also experienced significantly less weight gain than did those treated with NPH insulin.29 The HOE 901/2004 Study Investigators Group reported similar results in a study that compared NPH insulin and insulin glargine, with and without zinc, in 204 patients with type 2 diabetes whose glucose levels were not controlled with oral therapy. Zinc was added as a hexamer-stabilizing agent to delay onset and further increase the duration of action of insulin glargine. All treatments were equally and significantly effective in lowering FPG, but nocturnal hypoglycemia occurred in only 7.3% of patients who received insulin glargine compared with 19.1% of those treated with NPH insulin.30
In 2003, Riddle et al20 compared insulin glargine and NPH insulin in achieving HbA1C concentrations of <7% when added to oral therapy in patients with type 2 diabetes. This randomized, open-label, parallel-group, 24-week multicenter trial included 756 overweight men and women with type 2 diabetes and poor glycemic control (HbA1C >7.5%) despite therapy with 1 or 2 oral agents. Insulin therapy was monitored and titrated weekly using a forced titration algorithm. There were no significant between-group differences in FPG (insulin glargine, 117 mg/dL; NPH insulin, 120 mg/dL) and HbA1C (insulin glargine, 6.96%; NPH insulin, 6.97%). However, the rate of documented nocturnal hypoglycemia (FPG ≤72 mg/dL) was significantly lower with insulin glargine than with NPH insulin (33.2% vs 26.7%) (P < .05).20
Overcoming Barriers to Insulin Therapy
Some major barriers—logistics and education regarding insulin injection, patient fears of hypoglycemia, and concerns about possible weight gain—must be overcome when transitioning patients with type 2 diabetes to combination oral treatment and insulin therapy.31 Patient education is particularly important in overcoming resistance to insulin therapy. Treatment with a single dose of a long-acting insulin analog can help reduce the complexity of insulin therapy and decrease the risk of hypoglycemia and weight gain seen with NPH insulin. Although there may be treatment-related weight gain with insulin therapy in patients with type 2 diabetes, cardiovascular risk factors such as serum lipid profiles typically remain unchanged or are improved.32 In addition, no published data link exogenous insulin therapy with clinical cardiovascular disease. Lakka et al33 reported that endogenous hyperinsulinemia has only a modest association with increased cardiovascular mortality in middle-aged men and that this relationship results mainly from comorbid obesity, hypertension, and dyslipidemia.33
Conclusions
Insulin therapy is playing an increasingly important role in the management of patients with type 2 diabetes. Insulin therapy is a viable option for patients insufficiently controlled on one or more oral agents and should be considered early in the treatment algorithm. Optimal therapy should mimic the normal physiologic secretion of insulin, with minimal risk of hypoglycemia or other side effects. Treatment with a long-acting basal insulin that possesses favorable pharmacokinetic and pharmacodynamic properties can be an integral part of the insulin treatment strategy for patients with type 2 diabetes.
Strength of Recommendation (SORT)
The majority of patients with type 2 diabetes eventually require addition of insulin to achieve glycemic targets (SORT A).15,34 Addition of basal insulin to existing oral therapy is an effective means for achieving glycemic control (SORT B).20 New long- and short-acting insulin analogs may result in more predictable and effective insulin replacement (SORT C).
Notes
This work was supported by grants from Aventis (to MNF, MAB) and Novo Nordisk (to MAB).
- Received for publication January 4, 2005.
- Revision received January 4, 2005.




{kind=link}
{kind=link}