
Abstract
Objective: Lung cancer screening (LCS) implementation has been challenging for community and rural primary care settings. One contributing factor may be that the randomized clinical trials (RCTs) that form the evidence base are guided by explanatory methods not reflective of primary care settings. This study applied the PRagmatic Explanatory Continuum Indicator Summary (PRECIS - 2) tool to determine the pragmatism of LCS RCTs envisioned through a decentralized, primary care lens.
Methods: LCS RCTs were identified from efficacy meta-analyses, and the VA Demonstration Project was chosen as a nonrandomized multi-center comparator case. Two independent raters evaluated PRECIS-2 domains for each trial. Ratings were completed on a 5-point scale, where 1 indicated completely explanatory and 5 indicated completely pragmatic. Mean PRECIS-2 scores were calculated for each study and each domain. Descriptive information from raters’ comments was used to describe differences between the most pragmatic and most explanatory RCTs.
Results: Eleven RCTs and the VA Demonstration Project were evaluated. Mean PRECIS-2 scores for each study ranged from 2.12 to 3.33, with the DLSCT rated the most explanatory and the Lung Screening Study and ITALUNG studies rated the most pragmatic. Six domains had a mean score <3, indicating more explanatory (eligibility, recruitment, setting, organization, staff flexibility, follow-up). The remaining 3 domains had mean scores >3, indicating more pragmatic (adherence, outcome, analysis).
Discussion: This approach of evaluating each study from a primary care lens demonstrated that LCS RCTs trended toward a more explanatory nature, incorporating considerable support and infrastructure that extend beyond the capacity of typical primary care settings in the US.
- Cancer Screening
- Early Detection of Cancer
- Implementation Science
- Lung Cancer
- Pragmatism
- Preventive Health
- Primary Health Care
Introduction
Lung cancer screening (LCS) with low-dose CT (LDCT) has unparalleled potential to transform lung cancer outcomes and improve survival among high-risk individuals. When performed annually, LDCT reduced lung cancer specific mortality by approximately 20% relative to standard chest radiography.1,2 Unfortunately, translation from clinical trial to real-world practice has been onerous and slow, hindered by multilevel barriers. Ten years after receiving a grade B recommendation by the US Preventive Services Task Force,3 rates of LCS among eligible individuals have only reached 5.8% nationally4 and sustained annual participation is extremely low at 22%,5 starkly lower than >90% rates reported in large efficacy trials.1,6
The Centers for Medicare and Medicaid Services (CMS) mandated several LCS process requirements7 that have impacted implementation in community, rural, and low-resource settings.8,9 To meet these logistic requirements, organizational structures of LCS programs predominantly fall into 1 of 3 types: centralized, decentralized, or hybrid.10 In a centralized model, the entire screening process, from identifying eligible individuals through a shared decision making visit, referral for LDCT, and results reporting and follow-up, is conducted by the program with limited primary care involvement. These types of programs typically have navigators or coordinators to facilitate the LCS process.10 In a decentralized structure (the most common form of primary care in the US), the program only performs the LDCT and interpretation, with all other components completed by primary care/ordering clinician.10 Hybrid programs use aspects of both centralized and decentralized programs.10 Centralized program structure has been associated with improved adherence to LDCT follow-up recommendations and may help minimize racial disparities.11,12 Unfortunately, centralization may be unrealistic for rural and low-resource settings with limited personnel and financial means.
Often the first-point of contact in the health care system, primary care has an important and increasing role in cancer screening and early detection.13 Specific to LCS, the role of primary care is vitally important because clinicians must refer patients for LCS, and clinician recommendation is a leading factor for why individuals undergo LCS.14 Common barriers for LCS in primary care include difficulty identifying eligible individuals, uncertainty of eligibility guidelines, and time constraints with competing health priorities.15,16 Given both USPSTF and CMS guidelines are largely based on efficacy results of large randomized controlled trials (RCTs),3,7 it is no surprise that processes required to received reimbursement for services are not particularly pragmatic in nature, leading to challenges with real-world application for primary care. To strengthen this evolving role, more emphasis must be placed on understanding how to support primary care’s role in LCS.17
While it was vitally important to test the efficacy of LCS under ideal circumstances with RCTs, it is also essential to test the effects of LCS in usual care settings. Pragmatic clinical trials test interventions under real-world conditions to determine whether results generalize to a broader range of delivery settings and populations, emphasizing external validity.18,19 This contrasts with efficacy-focused trials, also termed explanatory trials, that exert greater control over trial variables, delivery settings, and populations to test whether an intervention works under ideal conditions, placing a greater emphasis on internal validity.18,19 The design of the clinical trial is determined by the desired outcome, although clinical trials are rarely exclusively explanatory or pragmatic.19 The Pragmatic Explanatory Continuum Indicator Summary (PRECIS-2) tool was developed by multiple invested partners, including clinical trialists, clinicians, policy makers and the public, to guide trial planning and use appropriate procedures and measures.19 For example, if the research question asks whether the intervention studied will be effective across a breadth of settings and populations, then it should choose a study design that is more pragmatic than explanatory.19
Given the challenges implementing LCS in primary care to date,15,16 the study goal was to determine whether existing LCS RCTs were more explanatory or pragmatic for primary care clinics, according to the PRECIS-2 tool. The premise was that identifying elements of trials that are more pragmatic may yield lessons for improving LCS implementation in primary care. Although the PRECIS and PRECIS-2 tools were initially developed for planning trials, they have also been used to assess the level of pragmatism of published trials.20⇓–22 Our specific aim was to use the PRECIS-2 tool to rate LCS RCTs that compared LDCT to a control arm, as envisioned through a decentralized, primary care lens. This perspective is important because this is a common model of LCS delivery in the United States, particularly in rural areas, and primary care has reported the most challenges and barriers to LCS implementation.8,9,15,16
Methods
Selection of Studies Chosen for Rating
RCTs included in this study were identified from recent meta-analyses focused on evaluating the efficacy of LDCT screening on lung cancer and/or all-cause mortality,23⇓–25 including studies that offered a detailed randomization process and study procedures. Excluded studies lacked published data for the commonly reported PRECIS-2 domains of population, setting, outcomes, and analysis. Given the population health focus, the VA Demonstration Project (VADP) was selected as a non-RCT multi-center comparator case that initiated screening following the publication of National Lung Screening Trial (NLST) results.26
Assumptions of LCS within Primary Care
PRECIS-2 was developed as a rating scale to assess the degree to which a trial is more explanatory or pragmatic across 9 domains: 1) eligibility, 2) recruitment, 3) setting, 4) organization, 5) flexibility of delivery, 6) flexibility of adherence, 7) follow-up, 8) primary outcome, and 9) primary analysis.19 Each domain has relevance and contributes to the overall PRECIS-2 score. To rate the PRECIS-2 domains in a standardized fashion, raters need clarification of what a “usual-care setting” is able to accomplish, as described by Luoma et al20 Based on our decentralized primary care perspective, the research team of primary care clinicians, LCS experts, and health services researchers reached consensus on the assumptions, shown in Figure 1, of usual primary care capacity to guide PRECIS-2 ratings.27,28

Assumptions of “usual care setting” for a decentralized, primary care perspective: Assumptions are based on the prevailing primary care infrastructure at the time of the rating process in 2022.27,28 Abbreviations: LDCT, low-dose CT; LCS, Lung cancer screening; CMS, Centers for Medicare and Medicaid Services.

Comparison of least and most pragmatic trials illustrated on the PRECIS-2 wheel: The Lung Screening Study and the ITALUNG trial were the most pragmatic studies, while the Danish Lung trial was the least pragmatic. The organization domain was unratable for the Danish Lung trial due to inadequate information available in manuscripts to complete a rating. Abbreviation: PRECIS, PRagmatic Explanatory Continuum Indicator Summary.
Development of Rating Checklist and Data Collection
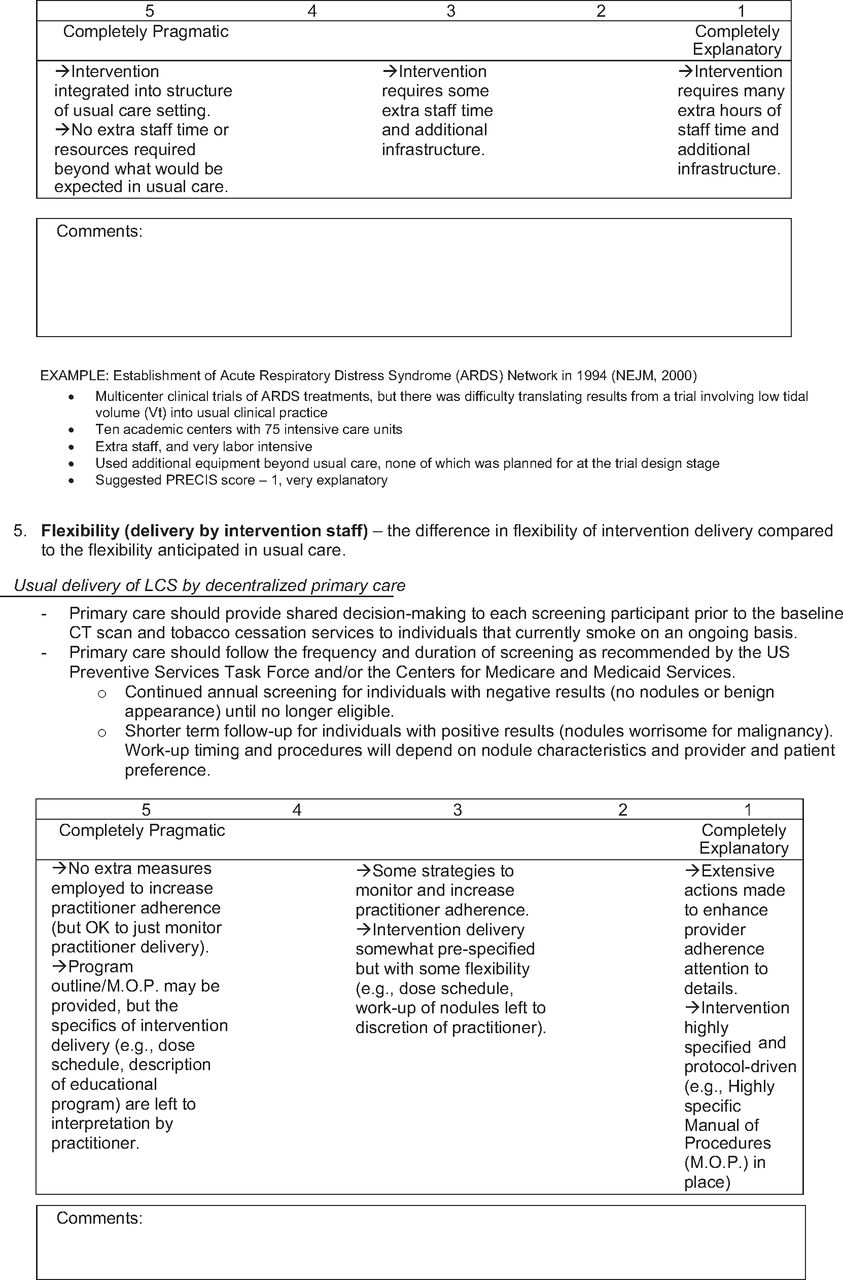
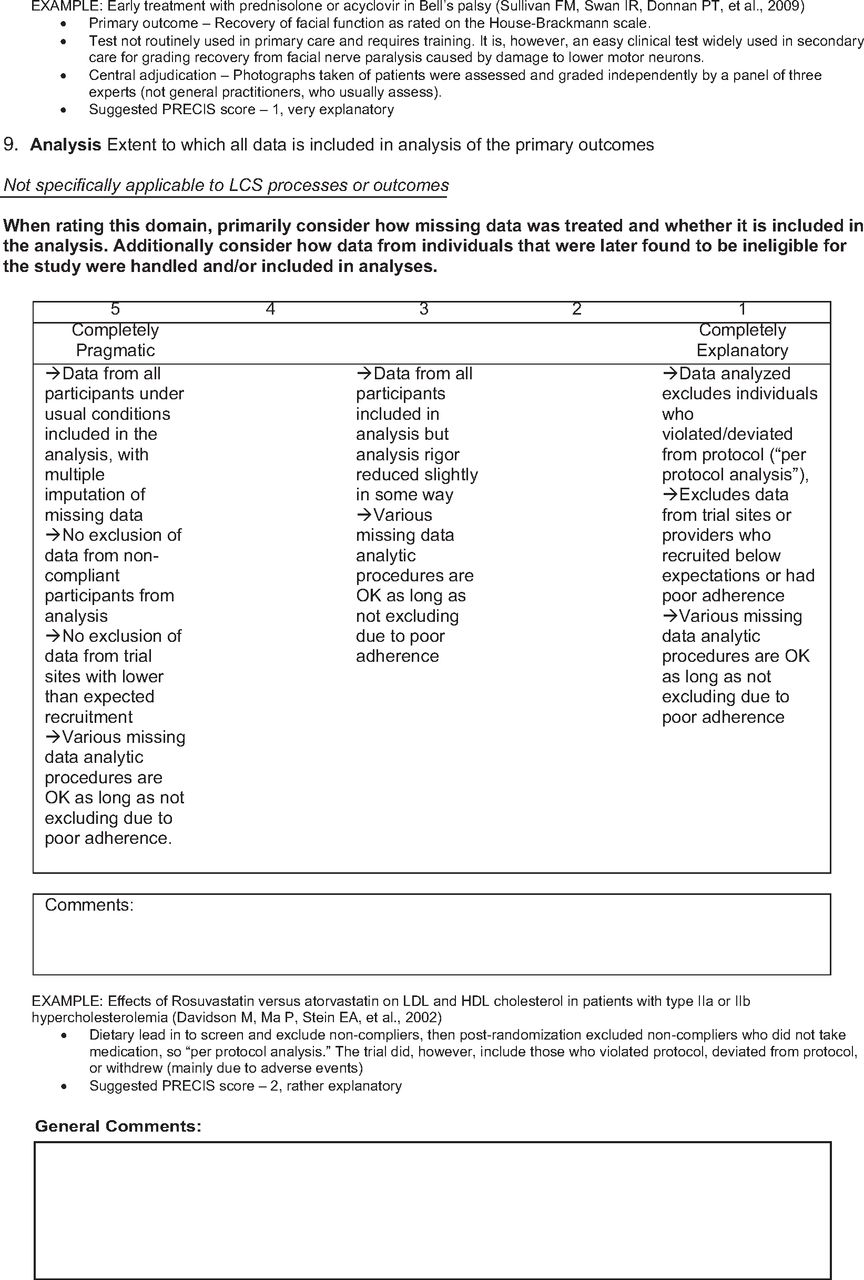
Each RCT meeting eligibility criteria was rated across all 9 PRECIS-2 domains on a 5-point Likert scale, where 1 indicated completely explanatory, 3 indicated equally explanatory and pragmatic, and 5 indicated completely pragmatic. A complete description of the PRECIS-2 tool and domains are available elsewhere.19 We adapted a rating tool used to evaluate PRECIS-2 in a prior review.20 This tool included relevant LCS information for each PRECIS-2 domain to consider about a decentralized primary care approach, according to the 3 assumptions of LCS within primary care (Figure 1). The aspects of each PRECIS-2 domain that make it more pragmatic or explanatory are briefly described in Table 1, with the complete rating tool included as Appendix 1.
Description and Rating Anchors for Each PRECIS-2 Domain*
The PRECIS-2 tool has been shown to have good interrater reliability and face validity,29 and consistent with prior use of PRECIS-2 for retrospective RCT analysis, 2 raters independently rated each included RCT and a third rater was used for arbitration, if necessary.20⇓–22 Raters had expertise in implementation science, primary care practice, and lung cancer screening. To standardize PRECIS-2 ratings, an initial rater calibration phase was used, as described by others.20,21 During calibration, the tool was tested with 2 randomly selected RCTs by 2 raters that subsequently rated all trials (SZ and MM), and scores were then discussed and clarified with the greater study team before rating additional studies. Two raters (SZ and MM) then independently rated 2 or 3 studies at a time and participated in routine consensus meetings to discuss ratings and agree on a single score for each PRECIS-2 domain for each study. A third rater (EAH) arbitrated ratings as necessary through additional consensus meetings to discuss ratings and supporting text.
Data Analysis
Characteristics of trials included in this investigation were analyzed descriptively to provide information on each RCT study design, eligibility criteria, and descriptions of LDCT and control arms. For each study, the mean PRECIS-2 composite and a mean PRECIS-2 domain score average was calculated. We qualitatively compared characteristics of trials with composite scores and domain scores that were highly pragmatic and highly explanatory. Descriptive information from raters’ comments was used to describe differences between the most pragmatic and most explanatory RCTs. This study is IRB exempt since it uses data available in published manuscripts.
Results
Selection of Studies
Recent meta-analyses identified 12 LCS RCTs that met the eligibility criterion of comparing LDCT to a comparator arm.23⇓–25 Of these 12 RCTs, 1 was excluded30 due to insufficient published data to complete the PRECIS-2 ratings. Inclusion of the non-RCT comparator case (VADP26) left 12 studies available for review.1,2,26,31⇓⇓⇓⇓⇓⇓⇓–39 To better inform PRECIS-2 ratings, additional manuscripts containing information about study procedures were used when available (e-Table 1).
Characteristics of Included Studies
Characteristics of each study are presented in Table 2. Most studies (67%) were conducted in Europe, compared LDCT screening to no screening in the comparator arm, and completed screenings at multiple locations. Study procedures were predominantly completed at specialized hospitals affiliated with academic, research, or cancer centers. All studies included a minimum baseline and 1 annual LDCT screening in the comparator arm, except for the Chinese AME Thoracic Surgery Collaborative Group31 that incorporated a baseline and 1 biennial LDCT. The Multicentric Italian Lung Detection (MILD)38 study randomized to 2 separate intervention arms, 1 annual screening and 1 biennial screening. In addition, the Dutch-Belgian Randomized Lung Cancer Screening Trial (NELSON)2 lengthened the frequency of screening over the study to intervals of 1 year, 2 years, and 2 and a half years (LDCTs performed at baseline, years 1, 3, and 5.5).
Characteristics of the Studies Included in the PRECIS-2 Ratings
PRECIS-2 Ratings
The composite PRECIS-2 score for each study ranged from 2.12 to 3.33 (Table 2). The VADP26 was rated as 3.00, similar in its ratings to other RCTs, despite its aim to enroll a more geographically diverse set of hospitals. Figure 2 illustrates the differences in each PRECIS-2 domain between the most explanatory trial, the Danish Lung Cancer Screening Trial (DLCST)34 (mean PRECIS-2 score 2.12 (Standard Deviation (SD) ±0.83)) and the 2 most pragmatic trials, the Lung Screening Study (LSS)36 (mean PRECIS-2 score 3.33 (±0.50)) and the ITALUNG study35 (mean PRECIS-2 score 3.33 (±0.87)). Descriptive information and rationale for each domain of these 3 studies are presented in Table 3. The Danish Lung trial was rated as highly explanatory for several PRECIS-2 domains, including stricter exclusion criteria, infeasible primary care recruitment strategies, screening completion at a single center, and diagnostic follow-up that was highly protocol-driven. The LSS was rated as highly pragmatic in several PRECIS-2 domains, due to broader eligibility criteria that resembles current CMS guidelines, recruitment and study procedures completed across several sites, and primary care discretion for diagnostic follow-up of positive results. ITALUNG also had broader inclusion criteria, utilized multiple screening centers, and involved primary care in the recruitment and support for study participants, increasing adherence, as would be the case in clinical practice.
Comparison and Rationale for PRECIS-2 Ratings of Least and Most Pragmatic Randomized Controlled Trials
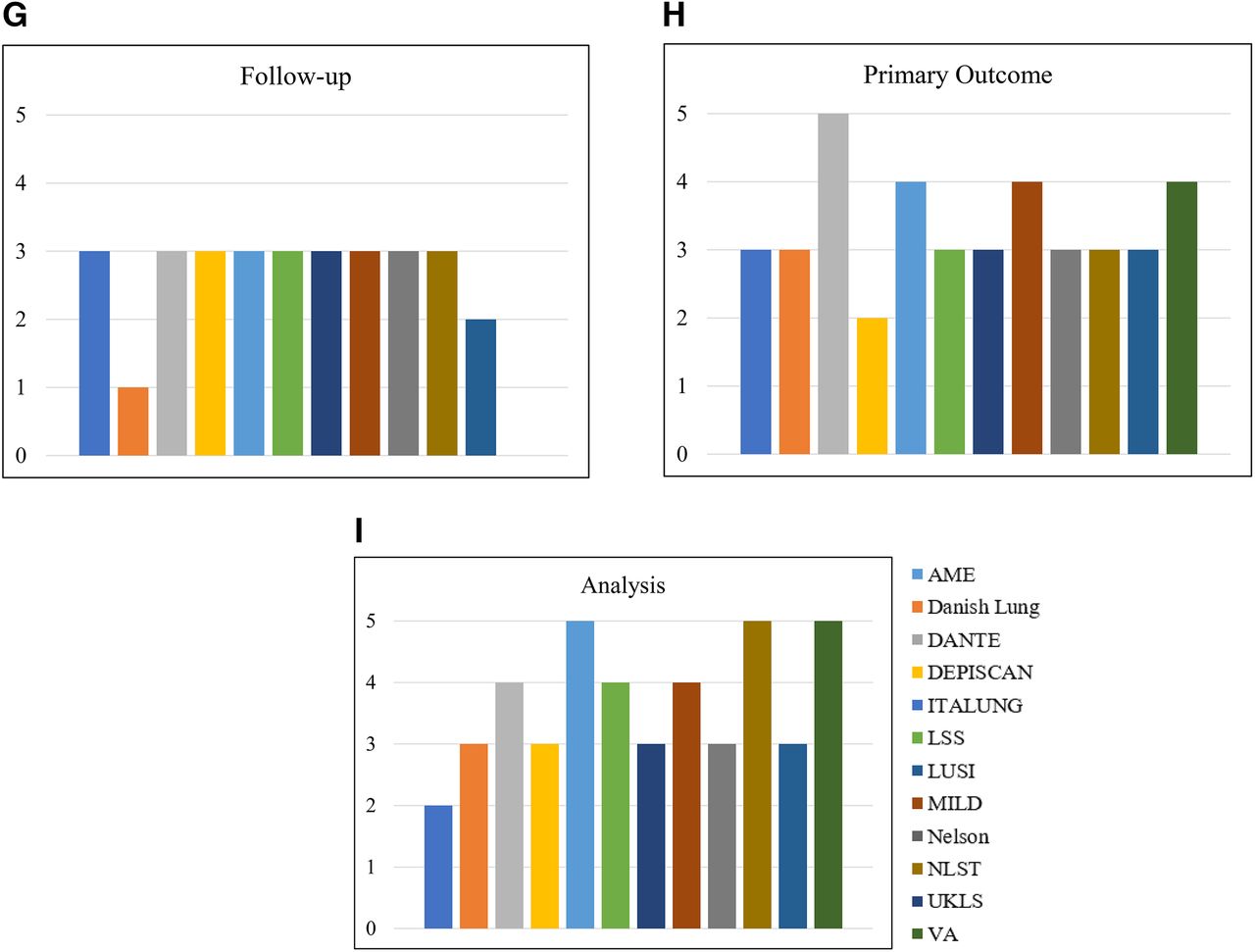
Composite mean PRECIS-2 scores for each domain for all eleven RCTs are illustrated on the PRECIS-2 wheel in Figure 3 (as a non-RCT the VADP26 was excluded). Six domains had a mean score <3, indicating more explanatory, including eligibility (mean score = 2.91 (±0.83)), recruitment (mean score = 2.54 (±0.69)), setting (mean score = 2.50 (±0.97)), organization (mean score = 2.86 (±0.69)), staff flexibility (mean score = 2.62 (±2.92)), and follow-up (mean score = 2.72 (±0.65)). The remaining 3 domains had mean scores >3, indicating they were more pragmatic in nature, including adherence (mean score = 3.18 (±0.40)), outcome (mean score = 3.27 (±0.79)), and analysis (mean score = 3.54 (±0.9)). The spread of PRECIS-2 for each domain across the 12 studies are included in e-Figure 1; a 5 rating (completely pragmatic) was specified only 4 times across all 12 studies, once for primary outcome (DANTE study32) and 3 times for analysis (ITALUNG,35 NLST,1 and VADP26 studies). Similarly, a 1 rating (completely explanatory) was given 5 times, twice each in the setting (German Lung Cancer Screening Intervention Trial37 and MILD38 studies) and flexibility for delivery by staff (DLCST34 and VA26 studies) domains and once in the follow-up domain (DLCST34). Four PRECIS-2 domains (setting, organization, flexibility (adherence), and follow-up) could not be rated for several studies due to limited information available in study manuscripts (Table 4). Disagreements between pragmatic score (>3) and explanatory scores (<3) or determining if at least 1 domain was unratable occurred for 33% of studies, and consensus was generally achieved between SZ and MM; arbitration by a third reviewer (EAH) was needed for 17% of domains across all 12 studies (Table 4).

Composite ratings of PRECIS-2 domains: Composite ratings were calculated by averaging the domain score for each randomized controlled trial. If a domain was unratable the score was averaged over the number of studies with available rating data. Abbreviation: PRECIS, PRagmatic Explanatory Continuum Indicator Summary.
Mean Scores, Number of un-Ratable Domains, Number of Domains Requiring Consensus and Arbitration*
Discussion
The PRECIS-2 tool19 facilitated retrospective evaluation of eleven LCS RCTs and the VADP to evaluate trials on the explanatory to pragmatic continuum, with the goal of identifying pragmatic aspects that could help improve and sustain future primary care implementation. Through this assessment, results revealed the overall mean PRECIS-2 score for each published RCT and the VADP tended to be middle of the road at approximately 2.0 to 3.0 but leaned more toward explanatory than pragmatic. This approach of evaluating each study from a primary care lens demonstrated that these studies included considerable supports and infrastructure that were not very pragmatic – and thus likely go beyond the capacity of typical primary care teams in the US.
These findings broaden the body of knowledge that provide insight on how best to support and guide collaborative partnerships between primary care and LCS programs. Similar to the domains that our analysis scored as most “explanatory” (and less pragmatic/real-world) in this study (eg, recruitment, setting, organization, staff flexibility, and follow-up), relate to others’ work (qualitative interview studies) that found primary care clinician or physician lack adequate workflows for candidate identification, referrals, shared decision making, ordering, results follow-up, and providing educational and outreach opportunities.40,41 Importantly, primary care clinicians are at the forefront of LCS adoption,15 and using implementation frameworks and cocreation approaches42 where primary care champions and practices can work with LCS programs in different contexts to develop and test alternate clinic workflows and other implementation strategies to support clinician teams will serve to improve screening in diverse health care settings.
Certain PRECIS-2 domains tended to be more explanatory and less “real-world” than others. This sheds light on areas that future trials could consider to enhance external validity and inform implementation. For example, the DLCST34 was rated completely explanatory in the flexibility (delivery by staff) and follow-up domains due to the rigidity of the study protocol for diagnostic pulmonary nodule work-up and the lack of primary care involvement. On the contrary, both the LSS36 and ITALUNG35 involved primary care for recruitment and support of study procedures and were rated as more pragmatic. Another notable reason Danish Lung34 was rated more explanatory was restricted study eligibility by excluding individuals that had quit smoking before the age of 50, making the study population much narrower than current CMS eligibility.7
Evidence prompting the US to move LCS into clinical practice was primarily based on the NLST and subsequently adjusted following publication of the NELSON trial, that detected a 20% and 24% (for men) relative reduction in lung cancer mortality, respectively.1,2 Thus, it is particularly important to consider areas that were more explanatory for these trials, as they highlight discrepancies between approach in the trial, the general populations served, and the supports available in primary care settings. Specifically, study clinicians often managed the diagnostic referral and work-up process for high-risk nodules. The NLST had a mean PRECIS-2 rating of 3.11 and NELSON was slightly more explanatory with a mean rating of 2.78. NLST has been the largest RCT to date with the highest number of screening centers (53,454 individuals participated at 33 centers)1 contributing to the pragmatism and generalizability of the study; however, NLST enrolled a population that is younger, healthier, and less racially/ethnically diverse than the greater LCS-eligible population.43 Other explanatory elements of the NLST included a set protocol for pulmonary nodule management with limited primary care involvement across the organization, flexibility (staff), and flexibility (adherence) domains. The second largest study (NELSON; n = 15,792) included individuals screened at 4 centers; however, only 17% of the enrolled population were women,2 highlighting one study weakness since the incidence of lung cancer is increasing in women across Europe.44 NELSON also had minimal primary care involvement for the diagnostic referral process for high-risk nodules.
Across all RCTs, the 2 least pragmatic PRECIS-2 domains were setting (mean score = 2.50) and recruitment path (mean score = 2.54), while the 2 most pragmatic domains were primary outcome and analysis, with mean scores of 3.27 and 3.54, respectively. Most (9/11 RCTs1,2,32,34⇓⇓⇓⇓–39 and the VADP26) conducted study procedures at specialized centers affiliated with academic, research, or cancer centers and limited the involvement of primary care, decreasing the pragmatism of the setting domain. Recruitment for European studies was completed primarily through broad advertising, which bypassed the need to identify eligible individuals in a primary care setting. The majority (8/11) of RCT primary outcomes were focused on the efficacy of LDCT to detect early-stage cancer and reduce mortality,1,2,31,32,34,35,37,38 while the remaining RCTs focused on outcomes relevant for feasibility of a larger trial,33,36,39 such as ease of recruitment and cost-effectiveness. Primary analysis was the most pragmatic domain; none of the studies excluded data from analyses due to poor adherence and all identified missing data. Importantly, the 2 most pragmatic domains are not components of contextual factors that influence implementation and sustainability for primary care.45
It is also informative to consider how determinants of implementation relate to these findings. The Practical, Robust Implementation and Sustainability Model (PRISM) specifies key contextual factors that influence implementation outcomes, such as reach to patients and adoption/sustainment by clinics, as specified in the RE-AIM framework.45 This approach is relevant to current endeavors to scale LCS, as shown by the efforts of the American College of Chest Physicians and the American Thoracic Society to develop a collaborative implementation guide for high-quality lung cancer screening based on the RE-AIM implementation framework.46 Aligning these findings with PRISM allows researchers to consider how domains rated more explanatory by PRECIS-2 associate with known implementation challenges.45 PRISM determinants of implementation success include: perceptions of LCS by staff/patients, characteristics of staff/patients; policy/funding environment, and the clinic implementation and sustainability infrastructure which may be considered as the supports needed to deliver LCS from patient identification to follow-up of LDCT findings. In this PRECIS-2 analysis, the least pragmatic domain (setting) reflects the characteristics of clinics in PRISM and reveals a large gap between the setting of trials (academic and research) and the variety of settings represented by primary care. The eligibility domain reflects the characteristics of LCS participants from PRISM, also revealing the difference between trial participants and individuals eligible per recommended guidelines, with particular underrepresentation of women and nonwhite participants.2,32 PRISM also posits that intervention implementation and sustainability is influenced by organizational infrastructure as reflected by recruitment, organization, and both flexibility domains in this analysis. With limited primary care involvement across many RCTs, these domains had mean PRECIS-2 ratings between 2.54 – 3.18, indicating trials are not wholly representative of usual primary care.
This PRECIS-2 analysis provided an innovative approach to describe the pragmatism of RCTs that form the LCS evidence base, and to the best of our knowledge, is the first application of an implementation framework to rate generalizability. This is important because these critical trials that have directly contributed to policy formation in the US and worldwide1,2 were planned and defined as efficacy trials, emphasizing internal validity with limited priority allocated external validity and pragmatic outcomes. Despite this important perspective, assumptions and perspectives regarding fee-for-service primary care settings for these ratings is also a limitation, as it does not wholly encompass LCS implementation completed through centralized or hybrid program structures in the US or implementation of LCS in other countries. PRECIS-2 ratings from a centralized structure lens in the US would likely be rated as more pragmatic, particularly for organizational infrastructure elements. Importantly, only 3 of the studies included in this analysis were conducted in the US, and differences in country health care infrastructure, workforce, and data systems will affect how other countries implement LCS. Differences in contextual factors could also result in how PRECIS-2 domains would be rated in diverse implementation environments. Another study limitation involved the modest number of trials available for evaluation; and of these, all were feasibility and efficacy trials, limiting the breadth of data available for this analysis. Finally, this analysis used 2 raters to independently rate each RCT; while this is consistent with others’ use of PRECIS-2 to retrospectively rate studies,20⇓–22 additional raters may have limited the need for arbitration across some domains.
In summary, this analysis found components of LCS RCTs and the VADP have a balance of explanatory and pragmatic elements when evaluated through a decentralized, primary care lens. Aspects of the trials that were rated most pragmatic, the primary outcome and analysis domains, are not directly related to intervention characteristics or strategies that influence implementation.45 These findings suggest a need to further study feasible implementation strategies to build capacity within primary care clinics to implement LCS, with attention to the PRECIS-2 domains that were more explanatory, particularly the recruitment and organization aspects that align with components of PRISM that influence successful implementation and sustainment of interventions in clinical settings. This is particularly important for low-resource and community LCS programs that often have even more limited staff/system supports than “typical” primary care.15,16 Future research and funding should prioritize pragmatic clinical trials to develop and test implementation strategies developed in partnership with primary care clinicians, teams, and communities. Cocreation of implementation approaches42 with primary care may enhance the overall LCS adoption and reach, ultimately increasing participation and transforming survivorship.
Complete List of Manuscripts Provided to Raters for Each Included Study

*Spread of PRECIS-2 ratings over each domain. a) eligibility criteria, b) recruitment path, c) setting, d) organization, e) flexibility (delivery by staff), f) flexibility (adherence), g) follow-up, h) primary outcome, g) analysis. *If a domain was classified as unratable the study column is left empty on each chart. Abbreviation: PRECIS, PRagmatic Explanatory Continuum Indicator Summary.

e-Figure 1. Continued

Appendix 1







Acknowledgments
E.A.H. is the guarantor of the paper and assumes full responsibility for the integrity of the submission, from inception to published article. E.A.H. takes responsibility for the integrity of the data and the accuracy of the data analysis. A.G.H and J.L.S. made substantial contributions to study conception, design, data interpretation, and writing of the manuscript. S.Z. and M.M. made substantial contributions to the study design, data collection, and writing of the manuscript. All authors read and approved the final manuscript.
Notes
This article was externally peer reviewed.
This is the Ahead of Print version of the article.
Funding: This research was supported by the National Cancer Institute Predoctoral to Postdoctoral Fellow Transition Award (K00CA564409) and by NIH/NCATS Colorado CTSA Grant Number UL1 TR002535. Content is the authors’ sole responsibility and does not necessarily represent official NIH views.
Conflict of interest: Dr. Hirsch reports grants from NIH/National Cancer Institute and non-financial support from NIH/National Center for Advancing Translational Sciences, during the conduct of the study. Dr. Studts reports personal fees from Johnson & Johnson and Genentech, outside the submitted work; and Dr. Studts volunteers on the Scientific Leadership Board of GO2 for Lung Cancer and the American Cancer Society National Lung Cancer Roundtable. Dr. Studts receives grant funding from National Cancer Institute, the Bristol Myers Squibb Foundation, the American Cancer Society, the Patient-Centered Outcomes Research Institute, the Colorado Department of Public Health and Environment, and the Centers for Disease Control and Prevention, outside the submitted work. Dr. Zane, Ms. McCreight, and Dr. Huebschmann have no conflicts of interest to disclose.
To see this article online, please go to: http://jabfm.org/content/00/00/000.full.
- Received for publication April 3, 2024.
- Revision received August 16, 2024.
- Accepted for publication August 26, 2024.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}