
Abstract
Suffering is often a part of the illness experience, and relieving it is a fundamental obligation of medicine. Distress, injury, disease, and loss generate suffering when they threaten meaning in the patient’s personal narrative. Family physicians have exceptional opportunities and responsibilities to manage suffering through long-term continuity relationships, demonstrating empathy, and building trust over time and across problems. We propose a new Comprehensive Clinical Model of Suffering (CCMS) founded on the family medicine approach to whole-patient care. Comprehending that suffering can involve every aspect of a patient’s life, the CCMS is constructed on 4 axes and 8 domains that form a “Review of Suffering” to help clinicians recognize and manage patient suffering. Applied to clinical care, the CCMS can guide observation and empathetic questioning. Applied to teaching, it can provide a framework for discussions of complex and challenging patients. Barriers to applying the CCMS in practice include clinician training, time with patients, and competing demands. However, by structuring the clinical assessment of suffering, the CCMS may increase the efficiency and effectiveness of clinical encounters and improve patient care and outcomes. The application of the CCMS to patient care, clinical training, and research will require further evaluation.
- Behavioral Medicine
- Disease Management
- Chronic Disease
- Clinical Medicine
- Communication
- Comprehensive Health Care
- Continuity of Patient Care
- Empathy
- End of Life Care
- Family Medicine
- Medical Ethics
- Palliative Care
- Patient-Centered Care
- Primary Health Care
- Suffering
- Quality of Life
Introduction
The relief of suffering is medicine’s ancient calling, primary goal, and the core of its ethics.1⇓–3 Yet, despite the centrality of suffering to medicine’s mission, there is little agreement about its definition and no bioethical consensus as to what it is.4,5
In his foundational work on suffering in medicine, Eric Cassell defined suffering as “the state of severe distress associated with events that threaten the intactness of the person.”6 According to Cassell, suffering is a personal, individual, subjective experience in which a person is distressed, feels a threat to personal intactness, is aware of a past and future, and ascribes meaning.6,7 Cassell’s model has dominated the dialogue about suffering for two generations but has been critiqued for being too stringent, logically inconsistent, and abstractly removed from clinical practice.8⇓⇓⇓⇓–13
At least in part because of this confusion, suffering and its relief are not a major focus of current medical education and clinical care.14⇓–16 It receives some attention in medical literature and medical school preclinical humanities curricula.16⇓⇓⇓⇓⇓⇓⇓⇓⇓–26 But patient suffering is rarely mentioned in clinical environments20,23 despite the distress it causes clinicians21 and the unfortunate potential for medical interventions to exacerbate rather than relieve it.27,28
Given its importance to medicine, its practitioners, and patients, a practical model of suffering is needed to apply to patient care and clinical environments. Drawing from literature across academic disciplines and helping professions, from interdisciplinary discussions with knowledgeable participants, and from clinical and teaching experience, we offer a Comprehensive Clinical Model of Suffering.
Understanding Suffering
Suffering is personal, individual, related to threats to the integrity of self, and experienced by the whole person, not just the body.6,29⇓⇓⇓–33 It is a physical, biopsychosocial, existential, and spiritual phenomenon.34⇓⇓–37 Sufferers face losses, or threats of loss, associated with the deterioration of the body and the disintegration of self, values, belief systems, and connections to the world.38 They feel isolated, hopeless, and helpless.
Suffering is an inevitable aspect of human existence and belongs to life “as much as fate and death.”39,40 Its intensity ranges from distress to agony.6,29,41 Though unremitting pain may be a source, suffering differs from pain. It is existential angst related to a sense that one can no longer be the person one has known oneself to be.31
The disruption of previously held ways of relating to the world can thrust the sufferer into an abyss of meaninglessness.30 Whether an illness causes suffering “depends on the whole texture of meanings and values intrinsic to a particular patient’s unique life narrative.”42 Family members, loved ones, caregivers, and clinicians can likewise suffer because a patient’s condition has meanings and values linked to their own life narratives.43
Meaning in life differs from person to person and from moment to moment.44 Thus, suffering can only be understood as a lived experience involving a singularly personal tale related to meaning and value in one’s life.45,46 To comprehend the sufferer, one must explore their story of suffering.
Suffering and the Promise of Family Medicine
Understanding another person’s suffering requires deep knowledge of their unique individuality.47 Contemporary medicine often fractionates patient care by diagnosis, age, gender, disease, organ system, and treatment method. Subspecialists providing episodic care may have less opportunity to gain the personal insight necessary to fully grasp patient suffering.
Family physicians—specialists in comprehensive continuity care for patients and families—are optimally positioned to detect and manage suffering. Comprehensive care is the management of “any health problem at any given stage of a patient’s life cycle”48 and involves “person-focused (not disease-oriented) care over time.”49 Comprehensive continuity care extends across the lifespan and includes the full spectrum of illness, loss, crisis, and death.
Family medicine carries the implicit commitment of the doctor to be present for the patient.50,51 Even when referring problems for subspecialty management, family physicians continue to follow their patients to witness their illness experience and suffering and to help ameliorate patient distress.51,52
Continuity begets a familiarity that helps the physician see the patient beyond the disease process. Through continuity, family doctors can counter some of the pressures of contemporary medicine,53 explore the patient’s story of suffering,16 and provide the type of care patients identify with ideal physicians54 who help them manage their suffering.
Diagnosing the disease identifies the pathologic processes in the body and may clarify treatment options to effect a cure, halt or slow its progression, or soothe accompanying symptoms. Caring for the patient, however, requires attention to their lived experience of illness in their personal psychological and social context.46
To provide more meaningful care, clinicians must go beyond diagnosis, symptoms, and treatments to validate the patient’s experience of illness and help the patient navigate toward wellness.55,56 To guide these efforts, we propose a model of suffering that encompasses these complexities yet is readily applicable to patient care.
Developing a Model of Patient Suffering
Based on a broad review of literature across disciplines, our team employed a narrative integrative scholarship of synthesis approach57 to develop a model of suffering that would be practically applicable to patient care in the primary care setting. Our team represents extensive involvement in academic family medicine, clinical practice, clinical teaching, behavioral science in family medicine, patient-doctor communication, primary care research, interdisciplinary education and practice, personal experience of suffering and caregiving, and scholarship on empathy, compassion, suffering, and healing.
We moved in an iterative process from literature review to graphical modeling to schematically capture the nature of suffering and care as informed by our experience and the principles of family medicine: comprehensive, continuous, patient-oriented, whole-person, and relationship-based. We identified 4 axes and 8 dimensions to summarize a parsimonious model of suffering in the illness experience of the whole patient. Throughout the process, we invited review and comment from colleagues, expert clinicians, teachers, and scholars, to assure the model included the major components of patient suffering and was clinically applicable to primary care.
The Comprehensive Clinical Model of Suffering
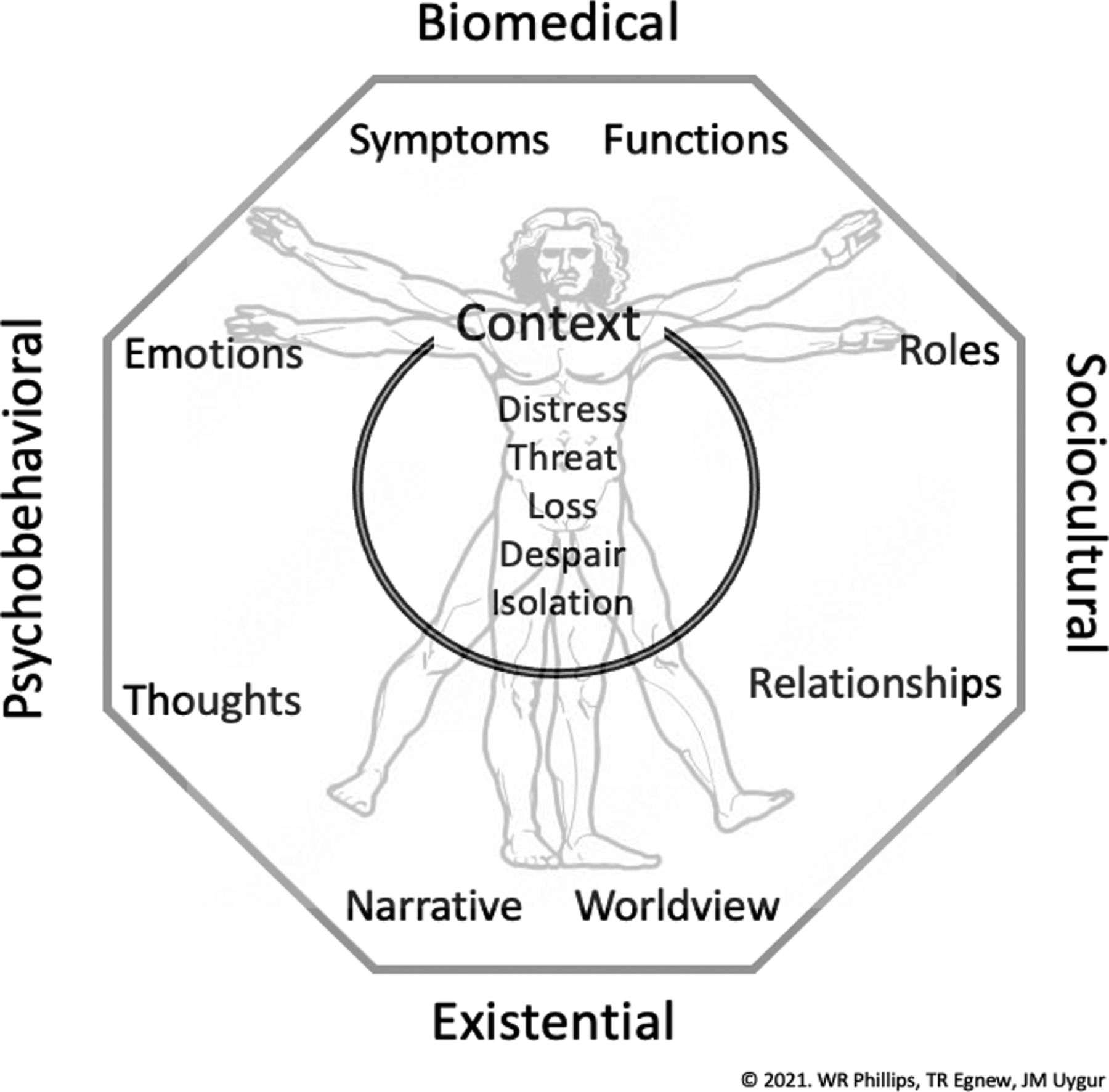
Illness is more than disease, care is more than diagnosis and treatment, and suffering involves every aspect of a patient’s life. Figure 1 graphically reflects the complexity of suffering summarized by the Comprehensive Clinical Model of Suffering (CCMS).

The Comprehensive Clinical Model of Suffering.
Patients usually consult their doctor for symptoms, problems, or needs they understand to be biomedical. Some encounters lead to precise diagnoses and specific treatments. However, particularly in comprehensive primary care, the patient’s “presenting complaint” often serves as an entry point to a longer story of a complex web of troubles, fears, losses, and suffering.
Conditions with clear biomedical pathophysiology impact other aspects of the patient’s life. Illness affects functions that are taken for granted when the patient is well.58 Socioculturally, these include important roles and relationships in the patient’s life. Psychobehaviorally, distressing thoughts and emotions develop as patients respond to the limitations and threats they encounter.
The CCMS places the patient at the center of a rich context that embraces the scope and breadth of the experience of suffering. It is constructed on 4 axes: biomedical, sociocultural, psychobehavioral, and existential. These axes encompass 8 domains: symptoms, functions, roles, relationships, emotions, thoughts, narrative, and worldview. Each dimension includes losses or threats of loss that can contribute to suffering (Table 1).
Matrix of Axes and Domains of Suffering with Clinical Examples
The biomedical axis is placed at the top, not because it is most important, but because it is the usual initial focus of the physician and expectation of the patient. The other axes reflect the depth and breadth of suffering that may be more important to some patients.36,59⇓–61
At the center of the model are the common patient experiences of suffering: distress, threat, loss, despair, and isolation. Surrounding the patient and shaping their unique experience of suffering is the patient’s perception of context. Laryngitis likely has a different meaning for a computer programmer working online than for a diva performing at La Scala.
We present the CCMS as a potential tool to help clinicians systematically investigate, organize, and understand the patient’s experience. We hope it can assist care teams to identify, discuss, and manage patient suffering collaboratively. Clinical testing and further research will be needed to assess its effectiveness to improve patient care and outcomes.
The Model at Work
The CCMS offers a potentially practical tool to improve patient care, guide clinical teaching and learning, and inform future research on suffering and holistic healing.
In patient care, the CCMS might guide close observation and empathetic questioning to help clinicians and caregivers consider the general axes and specific domains of suffering. Every patient is unique, and each illness is a multi-dimensional experience.The model can aid navigation through this complexity by providing a menu of potential elements of suffering that clinicians may choose to explore in their discussions with patients. Identifying sources may help patients recognize implicit and ineffable aspects of their suffering. Explicitly discussing these tacit experiences may diminish their power.55,56
The 8 domains of suffering comprise a “Review of Suffering” (RoS) that complements the “Review of Systems” memorized by every medical student. Clinicians could use this new RoS to systematically consider each domain and how it might contribute to the patient’s narrative, distress, and suffering.
In clinical practice, understanding the patient’s view of self and the impact of their illness are the foundations of patient-centered care and create a starting point to facilitate holistic healing. A structured RoS can generate dialog, avoid blind spots, deepen clinical assessment, promote trust and empower doctor-patient communication. This may be particularly important in complex or otherwise challenging cases. The CCMS can help clinicians organize essential and often difficult discussions about suffering with patients, family members, caregivers, and clinical teams. It can also provide a structure for the documentation of suffering in the medical record.14,25
In clinical teaching, the CCMS could help attendings and trainees name and display dimensions of suffering and map the connections between them to enrich didactic teaching, bedside consultations, and case discussion conferences. The RoS might help learners interweave scientific medicine with humanism by connecting their assessments of patients with the bigger picture of illness and care25 while increasing their insight into their own feelings, stimulating their empathy, and broadening their perspectives of the role of the physician. Providing a practical clinical model can encourage teachers and learners to engage more actively and accurately with patients as whole persons. Systematic use of the CCMS to assess knowledge and skills about suffering in the same way we document other core clinical competencies could help establish suffering in both the formal and hidden curricula.23
In research, the CCMS provides a schema for identifying key domains and axes of patient suffering that can aid investigators in organizing their questions and work in ways more closely connected to the patient’s experience and the clinician’s work. The model can also be used to introduce the importance of patient suffering in evaluation and quality improvement in health care systems.
As a shared model, the CCMS can help organize conversations that sometimes get lost in clinical complexity, medical urgency, and competing goals. Such a model can help us learn more about our patients, their lives, goals, and experience of illness. This richer understanding and deeper care might also help us learn about ourselves.
Patient Care Example
A brief patient care example in Appendix 1, Box A1 illustrates the everyday use of the CCMS to assess a patient’s suffering in a supportive way. Such discussion can enhance clinician and patient understanding, narrative editing, and holistic healing. Assessment of suffering includes close observation, deep listening, and synthesis of all clinical, social, and biomedical information. Questions proceed from the general to the specific and can focus on each of the 8 dimensions of suffering. The table linked to this clinical vignette (Appendix 1, Table A1) illustrates how the CCMS can help investigate, organize, understand, and begin to address the suffering this patient is experiencing.
Appendix 2 offers scripts of example questions clinicians can use to explore the domains of suffering in their patients.
Of course, not every question or domain pertains to each patient’s experience, and this work does not all need to be done in one visit. The primary care clinician can leverage the power of continuity over time and across problems to piece together the patient’s narrative of suffering. Working at this level challenges the family physician to use the refined clinical skills of patient-centeredness,62 agenda-setting,63 reaching common ground,64 shared decision making,65 goal-oriented care,66 relationship-centered care,67 and motivational interviewing.68
Challenges and Barriers to Clinical Application of the Model
Factors that limit the ability of doctors to engage patient suffering include training, time, tools, and talent. Biomedical culture and education do not prepare trainees to manage suffering.23 Students focus on biomedical diagnosis and treatment of disease, not the patient’s personal experience of illness and suffering.19 Without guidance, training, and support,69,70 witnessing suffering can be stressful for students,71 and burnout hampers their ability to engage with it.72,73
As medicine has become an industry and medical services a commodity, administrative burdens for clinicians have escalated, and demands for efficiency increasingly drive clinical encounters.74,75 Time is money, and doctors are paid for doing things to patients, not for listening to them. There are no billing codes for exploring suffering. Clues to stories of suffering may be lost in the squeeze for efficiency.76
Technology distances doctors from patients and depersonalizes patients’ illness experiences.77⇓–79 Electronic medical records offer no drop-down lists to address patient suffering. Although some tools exist for assessing suffering in palliative care patients,80,81 none are designed for primary care.
Managing suffering depends on the clinician’s abilities, skills, and attitudes. Witnessing suffering with equanimity and demonstrating therapeutic empathy, warmth, and authenticity are clinical skills that can be taught and learned.82,83 But openness to the patient’s experience of suffering requires tolerance for emotional vulnerability, an aptitude variable among physicians.84,85
Despite these impediments, continuity allows family physicians to gain the deep understanding of their patients necessary to see, feel, and appreciate their suffering. If the clinician can recognize suffering and manage effective responses to patient needs, they can contribute to the healing process.52,86 This type of care is emotionally challenging, and clinicians who engage in this way must be willing to grow and learn with their patients.87,88 Those who explore their patients’ experiences of serious illness and help them edit their stories of brokenness often discover this to be some of the most fulfilling work of their careers.87,89 In a context of trust, caring, and understanding, patients can be helped to transcend their suffering.52,86
Limitations
The CCMS model is limited, as any 2-dimensional model must be, and can only incompletely account for the complexity of illness, suffering, healing, and wholeness. Our process would have been enriched by including patients, caregivers, and families in the model’s development. These essential voices should be involved in any trials or evaluation studies.
Clinical application of the CCMS in primary care practice may be limited by factors that commonly frustrate clinicians. Issues of time and competing demands must be balanced across patient and clinician priorities. Explicit agenda setting, transparent clinician intent, and sample scripts can save time.64,90,91 The CCMS may make clinical encounters more efficient and effective by structuring the assessment of the complex experience of suffering. Helping patients address the sources of their suffering may also reduce unnecessary tests and consultations.
Accepting these significant limitations, we believe the CCMS can be helpful to clinicians, patients, and learners at all levels.
Next Steps
The CCMS model warrants further development and testing that includes members of the care team, patients, family, and community members. The critical component of context deserves further emphasis and research. The influences of language, culture, and health care systems on patients and clinicians require further study across various settings. Social determinants of health, racism, and other forms of discrimination have important impacts on health, medical services, and the experience of suffering and healing and deserve further study.92⇓⇓–95
The next step is testing the model in clinical applications across the full spectrum of health, illness, life transition, and loss. Does the use of the CCMS improve the process and outcomes of care, relieve suffering, and facilitate holistic healing? How does it influence clinical effectiveness, efficiency, and professional satisfaction among the health care team?
Primary care is ideally suited to use and test this model across various care settings. However, as the relief of suffering is a goal shared by all caring professions,96 we encourage other clinicians to consider testing the CCMS in their practice and teaching.
The application of the CCMS to medical education can likewise be evaluated to determine whether its use broadens and deepens case discussions and teaching about patients, their needs, and their care, and whether such learning helps fledgling clinicians deliver more holistic care with better results.
Closing Comment
The relief of suffering is an ancient obligation and now a pressing need for modern medicine. The challenges increase as advances in science mean that more patients live longer with chronic illnesses, endure more complex medical treatments, and survive and suffer longer near the end of life. Family physicians and other primary care clinicians care for these patients and their problems. The burdens of suffering continue to increase and beg relief for patients living with multimorbidity and polypharmacy,97 medically unexplained symptoms,98 chronic pain,99 substance use disorders,100 and long Covid.101
We hope this CCMS synthesizes scholarship, clinical experience, and family medicine perspectives for practical application to stimulate deeper thought, greater empathy, more systematic patient evaluation, and more effective and fulfilling patient care.
Acknowledgments
We thank our colleagues for the insightful comments they contributed to this work: Larry B. Mauksch, Seattle, WA, USA; Mark Murphy, Dublin, IRE; and Hamish Wilson, Dunedin, NZ. Dr. Phillips thanks the Fulbright Commission in Ireland and the Department of General Practice at the Royal College of Surgeons in Ireland, Dublin, for their generous support of his work.
Appendix 1. Patient Care Example of Using the Comprehensive Clinical Model of Suffering

Domains of Suffering in the Patient Vignette
Appendix 2. Example Clinical Questions to Explore Domains of Patient suffering
Exploratory Questions
Notes
This article was externally peer reviewed.
This is the Ahead of Print version of the article.
Funding: none.
Conflict of interest: none.
To see this article online, please go to: http://jabfm.org/content/00/00/000.full.
- Received for publication September 9, 2022.
- Revision received November 1, 2022.
- Accepted for publication November 3, 2022.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
In this issue




{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- Understanding Suffering
- Suffering and the Promise of Family Medicine
- Developing a Model of Patient Suffering
- The Comprehensive Clinical Model of Suffering
- The Model at Work
- Patient Care Example
- Challenges and Barriers to Clinical Application of the Model
- Limitations
- Next Steps
- Closing Comment
- Acknowledgments
- Appendix 1. Patient Care Example of Using the Comprehensive Clinical Model of Suffering
- Appendix 2. Example Clinical Questions to Explore Domains of Patient suffering
- Notes
- References
- Figures & Data
- References
- Info & Metrics