
Abstract
Background: Given the absence of guidelines for use of virtual visits for primary care delivery, a framework is needed to inform the most appropriate use of virtual visits.
Methods: We conducted in-depth, structured interviews of 18 patients, primary care clinicians, and other select informants. They were asked to discuss optimal, acceptable, and suboptimal uses of telemedicine for delivering care relative to in-person care delivery. The concepts expressed informed our development of a framework about appropriate use of virtual visits.
Results: The 103 concepts supported 5 main themes that emerged as a framework: clinical situations which are optimal for in-person care; situations optimal for virtual visits; situations that might be exchangeable between sites; contextual factors favoring in-person care; and contextual factors favoring virtual visits.
Conclusions: After further validation, we expect that this framework may guide future research and practice: it may be valuable for clinical practice redesign, for designing evaluations of the outcomes of virtual visits, for outcomes research, for patient education, for triage, and possibly for reimbursement considerations.
Virtual primary care became prominent during the COVID-19 pandemic out of necessity.1 Surveys of patients and clinicians suggest general satisfaction with these visits and enthusiasm for their continued availability, yet clinicians wish for professional guidance to direct best use of virtual visits.2 A rare example of such guidance is the Virtual Care Playbook from several professional societies in Canada; this provides some practical recommendations about when it may be safe and unsafe to use virtual visits.3 [Box]
BOX. Virtual Care Playbook (Canada)
Might safely use virtual care to: • assess and treat mental health issues • assess and treat many skin problems • assess and treat urinary, sinus and minor skin infections • provide sexual health care, including screening and treatment for sexually transmitted infections, and hormonal contraception • provide travel medicine • assess and treat conditions monitored with home devices and/or lab tests • review lab, imaging and specialist reports with the patient • conduct any other assessments that do not require palpation or auscultation.
Problems not amenable to virtual care include: • new and significant emergency symptoms such as chest pain, shortness of breath and loss of neurologic function • ear pain • cough • abdominal/gastrointestinal symptoms • many musculoskeletal injuries or conditions • most neurological symptoms.
A recent study that used prepandemic National Ambulatory Medical Care Survey data estimated that 66% of primary care visits might require in-person care.4 In preparation for that work, the authors, by necessity, generated a list of 6 examinations, 3 specimen collections, 15 procedures, and 10 treatments that require in-person services so that they could make their estimate. Like the Virtual Care Playbook, this list of services may be a valuable starting point for considering what can and cannot be delivered virtually; however, these are certainly just a subset of all patients' needs for which decisions must be made about the appropriate site of care to achieve the best patient outcomes.
A very comprehensive systematic review published in 2016 illustrates the breadth of outcomes that are reported in studies evaluating telemedicine interventions for primary care delivery, including outcomes like utilization, health outcomes, and costs.5 These are probably a subset of the needed outcomes for evaluating the appropriateness of virtual visits relative to in-person care. A rapid systematic review in 2018 concluded that outcomes are uncertain; it is unclear whether the use of virtual visits reduces the use of other services, duplicates services, or improves access to beneficial services.6 Optimizing the use of virtual visits requires a framework for thinking about best use of this care delivery mechanism.
In this work, we were interested in advancing understanding of how best to use virtual visits for primary care delivery, in comparison to in-person interactions. This was a pressing question for health systems and payors as new work flows were established early in the COVID-19 pandemic, and remains a priority as practices grapple with the on-going integration of virtual visits into practice. Given the absence of standards for appropriate use of virtual visits, we suggest that there is a need for a framework for allocating patients' clinical needs into appropriateness categories. Our goal was to establish a framework for diverse uses. We anticipate its use for clinical practice redesign, for designing local evaluations of the outcomes of virtual visits, for health services and outcomes research, for patient education, for triage, and possibly for reimbursement considerations.
For our purpose, high value care is that which achieves best patient outcomes and highest patient satisfaction for the investment.7 Our framing assumption was that, for primary care delivery, there are clinical situations in which a virtual visit is better than in-person care, meaning that a virtual visit is of higher value than an in-person encounter. Similarly, there are clinical situations in which a virtual visit is of equivalent value to in-person care, and situations in which it is inferior, meaning of lower value than in-person care. These premises are consistent with established approaches for considering the appropriateness of medical services.8 We first sought to understand what patients and clinicians consider to be good use of virtual visits.
Methods
In a previous study, we conducted in-depth, structured interviews of 18 patients, clinicians who deliver primary care, and other select informants.9 They were asked to discuss optimal, acceptable, and suboptimal uses of telemedicine for delivering care relative to in-person care delivery. Paired reviewers analyzed the content of the recorded discussions to identify the key concepts that motivated the informants and did thematic analysis to organize the concepts into unifying themes. The informants generated 103 unique concepts that aggregated into themes suggesting situations in which a virtual visit is appropriately used in primary care and situations in which it should be avoided.
For the present article, our team developed a preliminary framework reflecting what we learned. We use the term virtual visit in this framework, as this is the subset of telemedicine care that the informants were asked to consider. We made no distinction between audio-only and video visits in our discussions. We grouped the themes illustrating clinical and contextual factors according to their perceived appropriateness for virtual care delivery. We iteratively refined the framework through discussion and presented it to a broad audience of colleagues. The framework was then circulated to each of the key informants for comment by e-mail; the patient informants were contacted by phone. They were asked whether the framework captured what emerged in the earlier discussions and whether any items were misplaced or inaccurate. The framework was revised based on this feedback.
Results
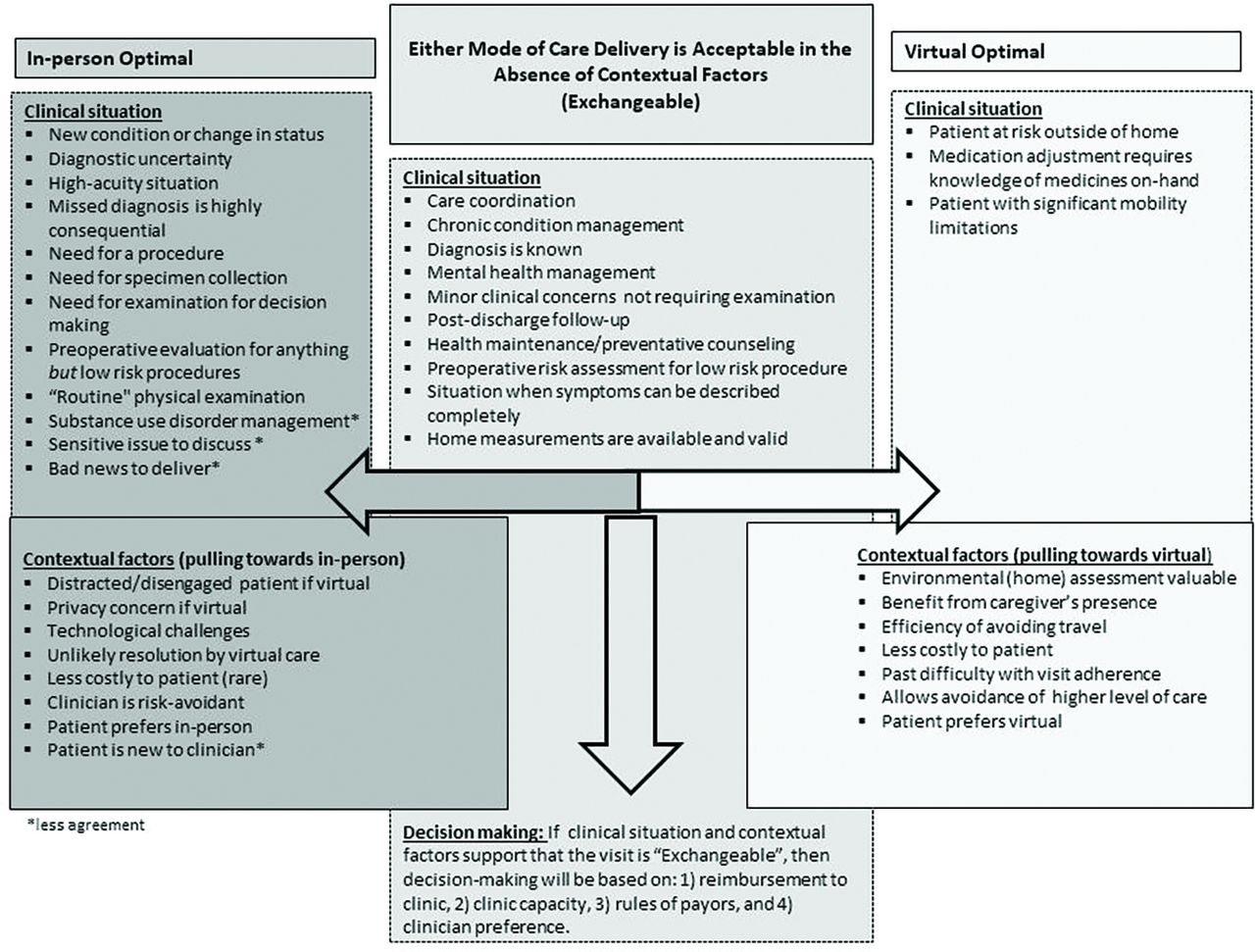
The resulting framework illustrates few clinical situations where a virtual visit is optimal, but many situations where it is likely to be exchangeable with in-person care. In addition, many contextual factors support the use of a virtual visit. As illustrated in Figure 1, the clinical situations that emerged as not exchangeable fell into categories: in-person care is optimal in situations that require that the patient be touched for specimen collection (eg, Papanicolaou smear), or intervention (eg, joint injection), or when the information needed for decision making requires a physical examination (eg, abdominal examination). In addition, in-person care is optimal if the patient has a new concern or change in status particularly in a high-acuity situation, where there is substantial diagnostic uncertainty, or where a missed diagnosis is likely to be consequential. We learned that virtual primary care delivery is considered to be optimal in just a few situations: when the patient has substantial mobility challenges limiting his or her ability to leave the home, when the patient is at risk when leaving the home (eg, infectious risk or weather-related risk), or when there is something within the home that is vital to decision making (eg, review of the medicine cabinet's content).
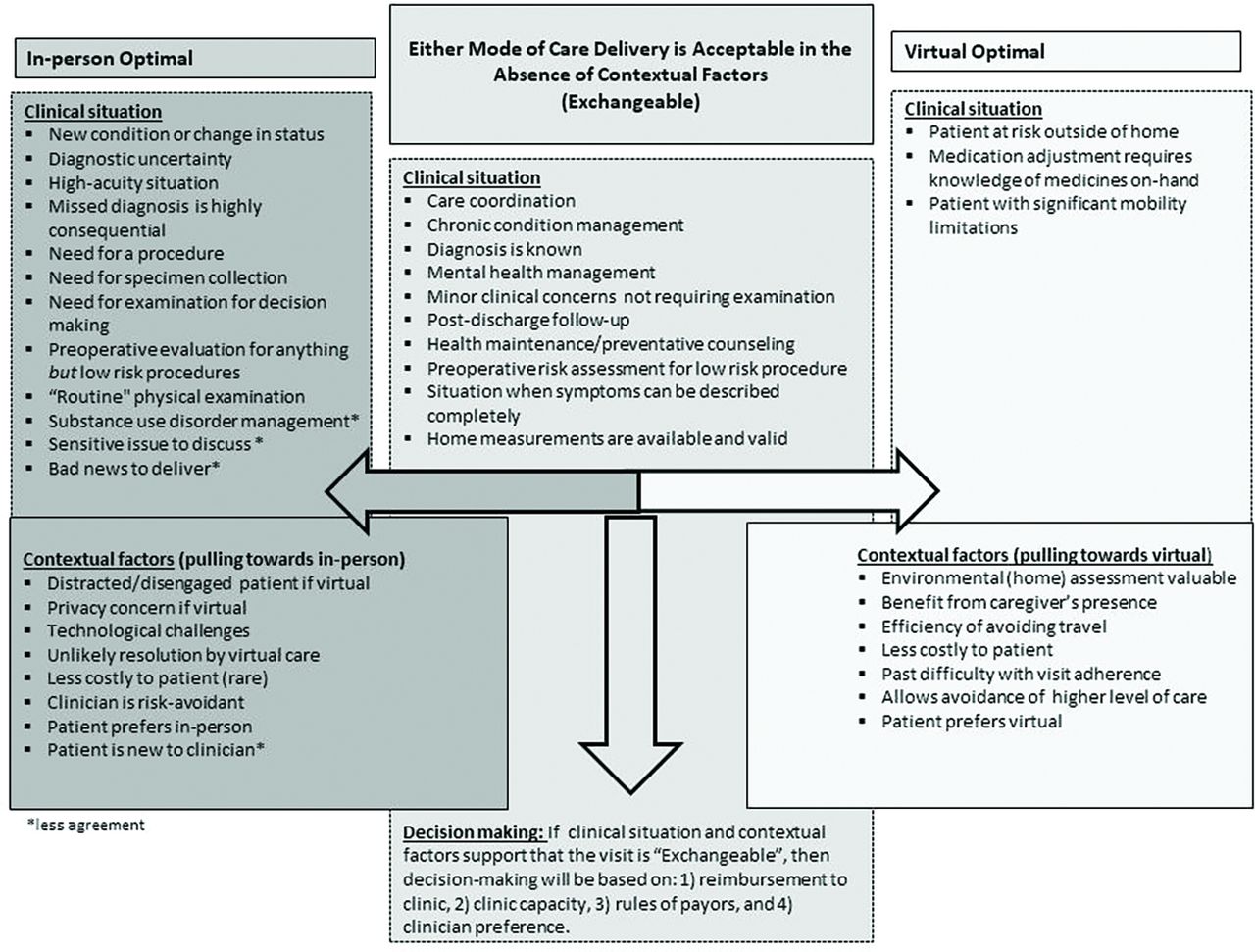
A framework for considering appropriate use of virtual care and in-person care for the delivery of primary care. Arrows indicate contextual factors that might make an “Exchangeable” clinical situation more appropriate as an in-person visit or more appropriate for a virtual visit delivery.
We found that many clinical situations were thought by our informants to be exchangeable – where a virtual visit or in-person care may be equally appropriate. In most of these situations, there will be a decision-maker who chooses whether the visit is face-to-face or via telemedicine and this decision is driven by contextual factors. The contextual factors identified by the key informants were rich and somewhat unexpected, such as clinicians' varying risk tolerance and patients' privacy concerns. Presently, the framework does not include any prioritization scheme for the contextual factors, but we suspect that they should not carry equal weight. For example, the absence of the necessary technology for virtual visits make virtual visits entirely inappropriate in any clinical situation. The decision as to whether audio-only communication is sufficient when video is unavailable is a different research question and is not addressed in this work. Additional work is needed to understand how to weigh contextual factors particularly if they are “pulling” in opposite directions. An example may be a patient who prefers in-person visits but has challenges completing appointments due to transportation barriers. In this situation, the context may favor scheduling the patient for a virtual visit.
If the clinical situation is exchangeable and there is truly an absence of contextual factors supporting a given type of visit, including an absence of a patient preference, we propose that the decision regarding visit type might be made based on: 1) reimbursement to the clinic, 2) the clinic's capacity for these visit types, 3) rules of payors, and 4) clinician preference. This did not emerge directly from the key informant discussions but seems to be a necessary part of the framework. This too requires investigation before the framework can be broadly utilized in practice.
Discussion
We expect that this framework should be valuable for the development of tools for triage and should inform the evaluation of the impact of virtual primary care services. The time is now; many practices and health systems are expanding their telemedicine services based on their prior experience, demand, new resource availability, and reimbursement.1,10 Other health systems outsource these services to providers, like Teladoc Health or AmWell that are covered by many insurance plans, and which also offer primary care services.
We recognize that our framework requires additional refinement— perhaps with the use of survey methods—with informants who are more broadly representative of clinicians and patients across primary care settings and from diverse geographies, including internationally. We might learn that there are key subgroups of informants with importantly different beliefs about appropriate and inappropriate uses of virtual primary care. In addition, the framework will require validation, which may involve learning whether virtual visits delivered in accordance with the classification illustrated in the framework is associated with high patient satisfaction, good clinical outcomes, and efficient practice.
Health care delivery systems might use the refined framework. We expect it has translational utility as a tool for triage to be used by nurses or other clinicians performing triage in response to patients seeking care. We expect it will be useful to guide the development of patient education materials that will help patients to select an appropriate modality for safe, satisfying, and efficient care. The framework should also be valuable for population health management such as by care managers who are looking to connect or reconnect patients to the most appropriate site of care, or by directors of accountable care organizations who are looking to deliver quality, high-value care to their enrolled populations. The estimates of cost-effectiveness of telemedicine have varied substantially by setting and situation;11 we expect that this framework may help in assessment of the value of virtual visits by providing a framework for considering the appropriateness of the site of care, which we expect to impact the patients' experience. The framework should guide future research and practice aimed at improving the use of virtual visits in primary care, so that the right care is delivered to the right patient, at the right time, affordably.
Acknowledgments
Kathryn McDonald, PhD for helpful edits.
Notes
This article was externally peer reviewed.
Conflict of interest: none.
All of the authors meet ICJME criteria for authorship.
Funding: Institutional funding from the Hopkins Business of Health Initiative. None of the authors has disclosures relevant to this work.
To see this article online, please go to: http://jabfm.org/content/35/3/629.full.
- Received for publication December 22, 2021.
- Revision received December 14, 2021.
- Revision received February 3, 2022.
- Accepted for publication February 8, 2022.




{kind=link}