
Abstract
Introduction: As the opioid epidemic progresses, a better understanding of those at elevated risk of opioid overdose is needed, particularly for populations whose growing risk may be overlooked. Medicare recipients under age 65 (Medicare-disability beneficiaries [MDBs]) are one such population. We sought to analyze characteristics of opioid-overdose hospitalizations among MDBs and quantify the contribution of this population to opioid-overdose hospitalizations overall.
Methods: This retrospective cohort study included patients hospitalized for opioid overdose in the National/Nationwide Inpatient Sample from 1998 to 2013. The primary outcome measurements were number and characteristics of discharges, including patient sex, age, race, prescription opioid versus heroin overdose, and comorbidities.
Results: MDBs constituted 11.7% of US opioid overdose hospitalizations among those under 65 years of age in 1998; this proportion grew to 24.5% by 2013 (P < .0001). The proportion of female patients grew markedly among this cohort (P < .0001) and were disproportionately represented among MDBs (P < .0001). Prescription opioid overdose accounted for a larger proportion of opioid overdose hospitalizations among MDBs than among non-Medicare-insured patients under 65 years old (P < .0001). MDBs generally exhibited greater comorbidity burden versus non-Medicare-insured patients under age 65; however, chronic drug and alcohol abuse were less commonly documented among the Medicare cohort (P < .0001).
Conclusions: MDBs constitute a substantial and growing proportion of opioid overdose hospitalizations in the United. To prevent opioid overdoses among MDBs, care must be taken to address the unique needs of this population.
The rate of opioid prescriptions, abuse, and overdose in the United States has grown in recent years, and the public health community has increased efforts to stem the tide of opioid abuse.1⇓–3 Examples of such efforts include Prescription Drug Monitoring Programs, prescription limits, naloxone distribution among emergency responders and laypersons, medication-assisted treatment programs, and increased provider and community education.4⇓⇓–7 However, opioid abuse and overdose rates remain unacceptably high, with nearly 2 million Americans reporting an opioid-use disorder.8⇓–10 A total of 33,000 opioid overdose fatalities occurred in the United States in 2015, and the economic cost was estimated at $504 billion.11 A better understanding of populations at an elevated risk of opioid use disorder is needed, particularly for populations whose growing risk may be overlooked.
Medicare recipients under age 65 (hereafter, Medicare-disability beneficiaries [MDBs]) constitute one such population. Medicare coverage under age 65 is restricted to individuals with certain conditions, such as end-stage renal disease or amyotrophic lateral sclerosis, and those with disabilities qualifying for Social Security Disability Insurance.12 Musculoskeletal conditions, which are often accompanied by chronic pain, are the most commonly cited qualification for Social Security Disability Insurance, suggesting that chronic pain may be common among MDBs.13,14 In fact, recent research found that nearly 50% of MDBs filled at least 1 prescription for opioid medications annually, more than 20% filled 6 or more opioid prescriptions, and 0.3% received care for a nonfatal overdose each year.7,15 Given that chronic pain and regular prescription opioid use are common among MDBs, these individuals may be at heightened risk for opioid use disorders and overdose.
The current opioid epidemic is multifaceted in nature, affecting heterogeneous populations with a variety of risk factors. Thus, the public health response to the epidemic must be equally multifaceted, addressing the unique needs of each individual affected. A thorough understanding of groups of individuals most at risk will be critical for developing actionable strategies to address the epidemic and reduce abuse and overdose. However, limited information is available on the characteristics of MDBs who overdose on opioids. This study analyzed hospital inpatient discharge data from 1998 to 2013 to characterize demographic trends in opioid overdose hospitalizations among MDBs. We aimed to determine whether MDBs are at particularly high risk of hospitalization from opioid overdose and to identify demographic trends and comorbidities among MDBs who experience such hospitalizations. Understanding the characteristics of particularly high-risk subsets of individuals may help public health leaders design opioid abuse prevention and treatment efforts that specifically cater to the unique needs of these individuals.
Methods
Data Source
This investigation used the National (Nationwide) Inpatient Sample (NIS) from 1998 to 2013, produced by the Healthcare Cost and Utilization Project under the Agency for Healthcare Research and Quality. The NIS is the largest all-payer database of inpatient discharge abstracts, containing an approximately 20% sample of US hospital discharges, which can be weighted to produce national estimates. Each year of data has approximately 7 to 8 million records, each containing International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes, patient age, and primary expected payer, among other information. Records from the years before the 2012 NIS redesign were reweighted in accordance with guidelines from the Agency for Healthcare Research and Quality. Given the deidentified and publicly available nature of this dataset, this investigation was deemed nonhuman subjects research and, therefore, was not covered under 45 CFR part 46. This investigation followed The Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines for observational studies.
Patient Selection
Patients were identified as experiencing heroin overdose (HOD) or nonheroin opioid overdose (NHOD) based on ICD-9-CM codes (NHOD, 965.00, 965.02, 965.09, e-code 85.01, e-code 85.02; HOD, 965.01, e-code 85.00). This coding algorithm has been previously used to study opioid-overdose hospitalizations in the NIS.16
Patient Characteristics
The following variables were extracted for each patient: age, sex, primary expected payer type, race, overdose type (ie, NHOD, HOD, or both), year of hospitalization, and all 29 values for the native NIS Elixhauser-defined comorbidities, which include AIDS, alcohol abuse, blood loss anemia, chronic pulmonary disease, coagulopathy, congestive heart failure, deficiency anemia, depression, diabetes (complicated and uncomplicated), drug abuse, fluid/electrolyte disorders, hypertension, hypothyroidism, liver disease, lymphoma, metastatic cancer, obesity, other neurological disorders, paralysis, peptic ulcer disease (excluding bleeding), peripheral vascular disorders, psychosis, pulmonary circulation disorders, renal failure, rheumatoid arthritis, solid tumor without metastasis, valvular disease, and weight loss. We further hypothesized a high prevalence of musculoskeletal disease among disabled patients; as musculoskeletal disease is not an Elixhauser-defined comorbidity, prevalence was assessed using an ICD-9-CM coding algorithm (Appendix Table 1).
Statistical Analysis
Descriptive statistics for opioid-overdose hospitalizations were generated. Characteristics among MDBs were compared with those among patients <65 years old without Medicare insurance. Comparisons between categoric variables were accomplished using the Rao-Scott design-corrected χ2 test. Logistic regression was used to assess trends in binary variables. All statistical analysis was performed using SAS 9.4 (SAS Institute, Cary, NC). Population data were abstracted from the US Census Bureau's intercensal estimates. Procedures such as surveyfreq, surveymeans, surveylogistic, and surveyreg were used to accurately calculate sample variance. Patients with missing data were excluded from analyses on a list-wise basis. Statistical significance was defined per the Bonferroni correction for 47 comparisons (P < .0011, [0.05/47]).
Results
Descriptive Statistics
In total, 815,970 patients (standard error, 13,944) experienced opioid overdose–related hospitalization during the study period and were included in our analysis (representing 169,640 unweighted records). A total of 50.8% (n = 425,646) patients were female, 77.5% (n = 539,856) were white, and 85.0% (n = 713,217) were aged <65.
Age Distribution of Opioid Overdose Hospitalizations
We observed a general increase in the incidence of opioid overdose hospitalization among all age groups from 1998 to 2013. The rate of overdose hospitalization among those aged 65 to 84 was 67.0 per million in 1998, increasing to 281.7 per million in 2013 (+321%). Similarly, the rate of overdose hospitalization among individuals aged 50 to 64 increased from 88.8 per million in 1998 to 411.5 per million in 2013 (+363%) (Appendix Figure 1; Appendix Table 2).
Opioid Overdose Hospitalizations among MDBs Versus Non-Medicare-Insured Under 65 Years Old
Payer Type
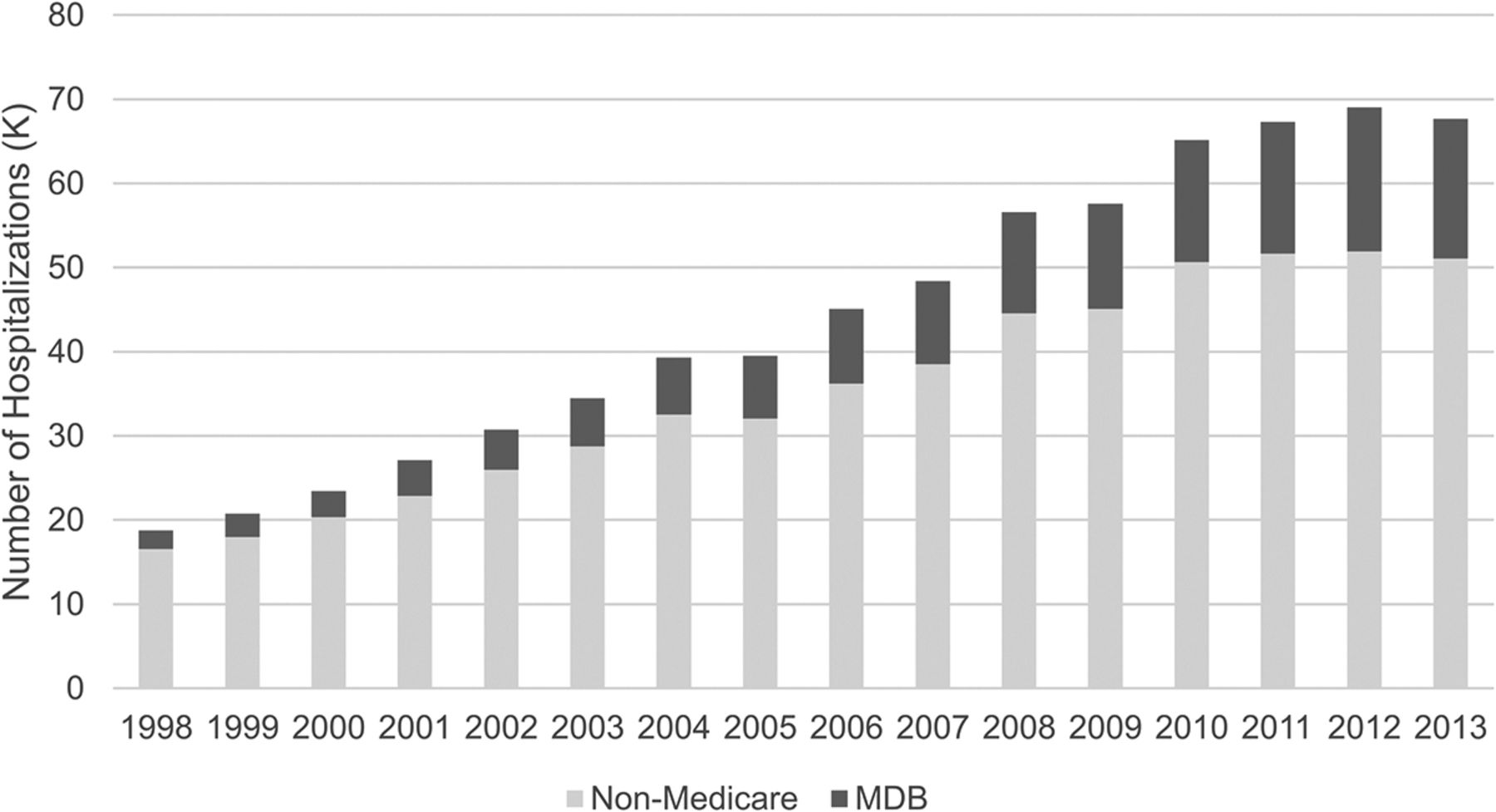
Among those patients under age 65 who were hospitalized for an opioid overdose, the proportion of patients with Medicare insurance significantly increased from 11.7% in 1998 to 24.5% in 2013 (trend, P < .0001) (Figure 1; Appendix Table 3).
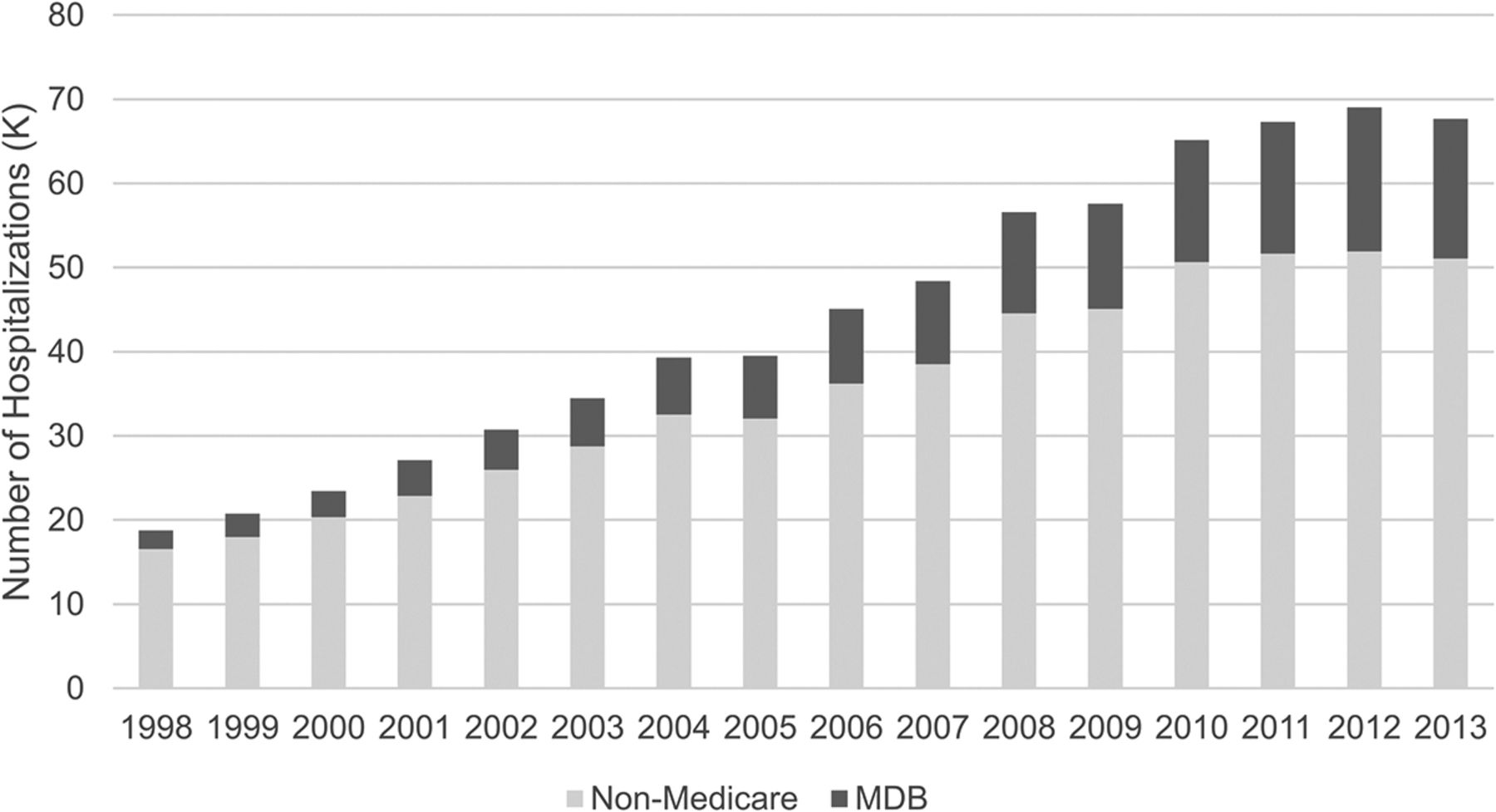
Opioid overdose hospitalizations among patients <65 years of age, by payer type (National Inpatient Sample, 1998 to 2013). MDB, Medicare-disability beneficiary.
Sex
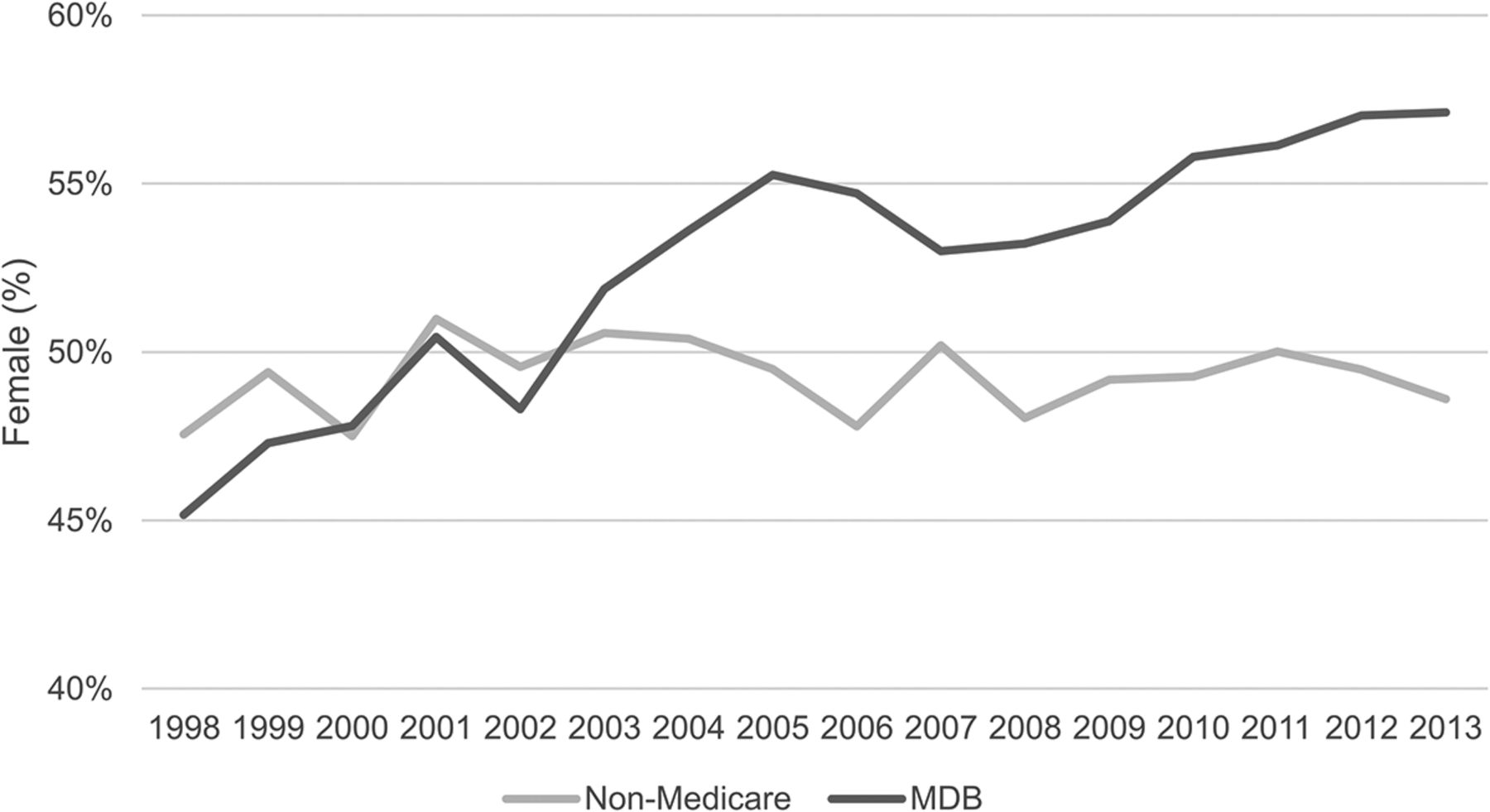
The proportion of females among MDBs significantly increased from 45.2% in 1998 to 57.1% in 2013 (trend, P < .0001). In contrast, the proportion of females among those under age 65 without Medicare did not change significantly: 47.6% in 1998 to 48.6% in 2013 (trend, P = .88). The difference between these 2 trends was statistically significant (P < .0001). In 2013, of patients hospitalized for opioid overdoses, females constituted a significantly greater proportion of MDBs than non-Medicare-insured patients (P < .0001). (Figure 2; Appendix Table 3)

Opioid overdose hospitalizations: percentage of female patients among those <65 years of age, by payer type (National Inpatient Sample, 1998 to 2013). MDB, Medicare-disability beneficiary.
Race
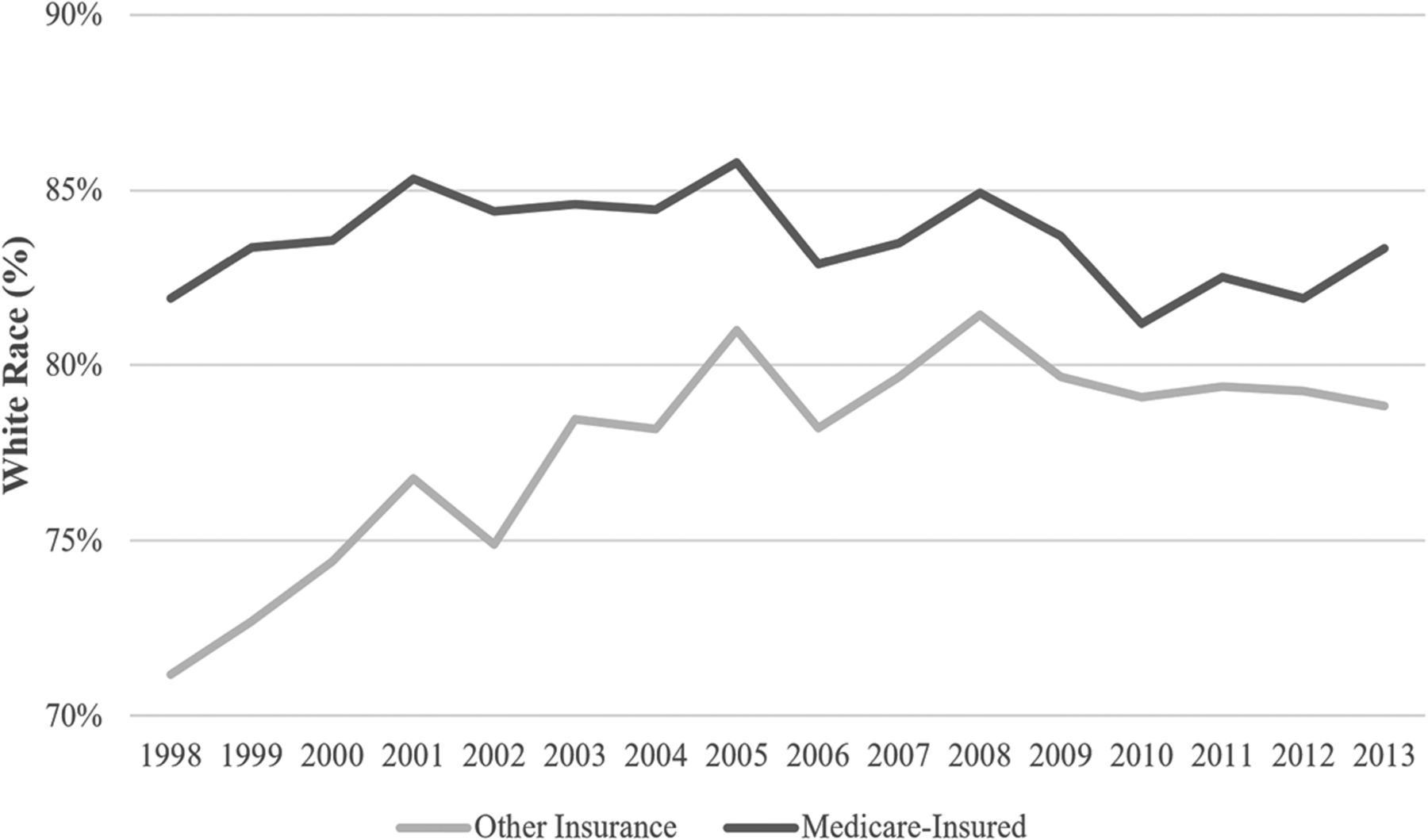
Between the years of 1998 and 2013, the proportion of MDBs in this overdose population who were identified as white did not significantly change (81.9% in 1998 to 83.3% in 2013; trend, P = .03), although the proportion of patients who were identified as white among non-Medicare-insured patients significantly increased from 71.2% to 78.8% during that same period (trend, P < .0001). The annual rate of change was significantly greater among non-Medicare-insured patients than among MDBs (P < .0001). In 2013, patients identified as white constituted a significantly greater proportion of MDBs than non-Medicare-insured patients (P < .0001) (Appendix Figure 2; Appendix Table 3).
Age
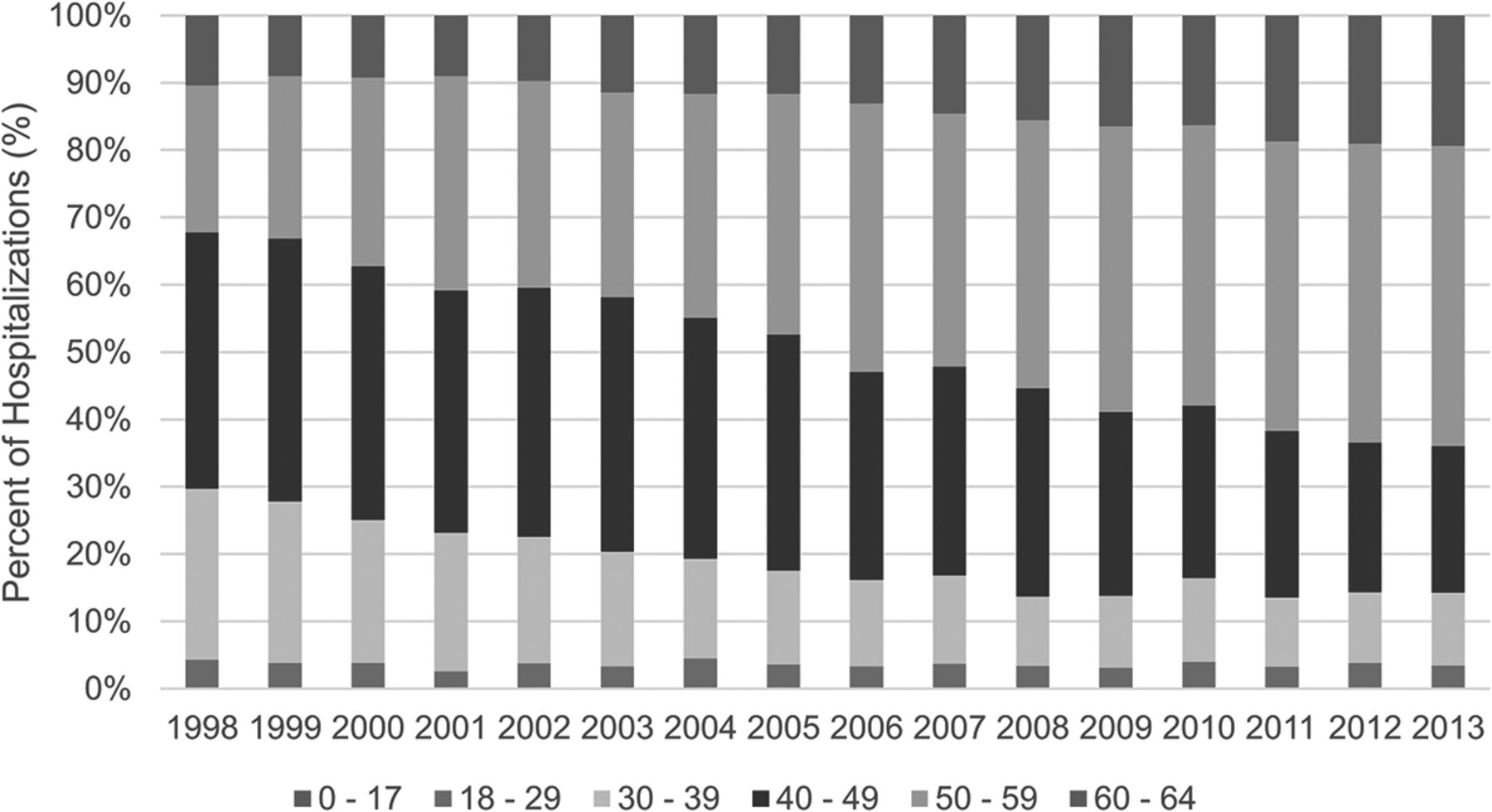
Among patients who were hospitalized for opioid overdose, the proportion of MDBs between 50 and 64 years of age significantly increased from 32.2% in 1998 to 64.0% in 2013 (trend, P < .0001), and the proportion among non-Medicare recipients significantly increased from 13.0% in 1998 to 30.3% in 2013 (trend, P < .0001). The annual rate of change in the proportion of beneficiaries between 50 and 64 years of age was significantly greater among MDBs than among non-Medicare recipients (P < .0001). In 2013, patients aged 50 to 64 constituted a significantly greater proportion of the MDBs than non-Medicare-insured patients (P < .0001) (Figure 3; Appendix Table 3).
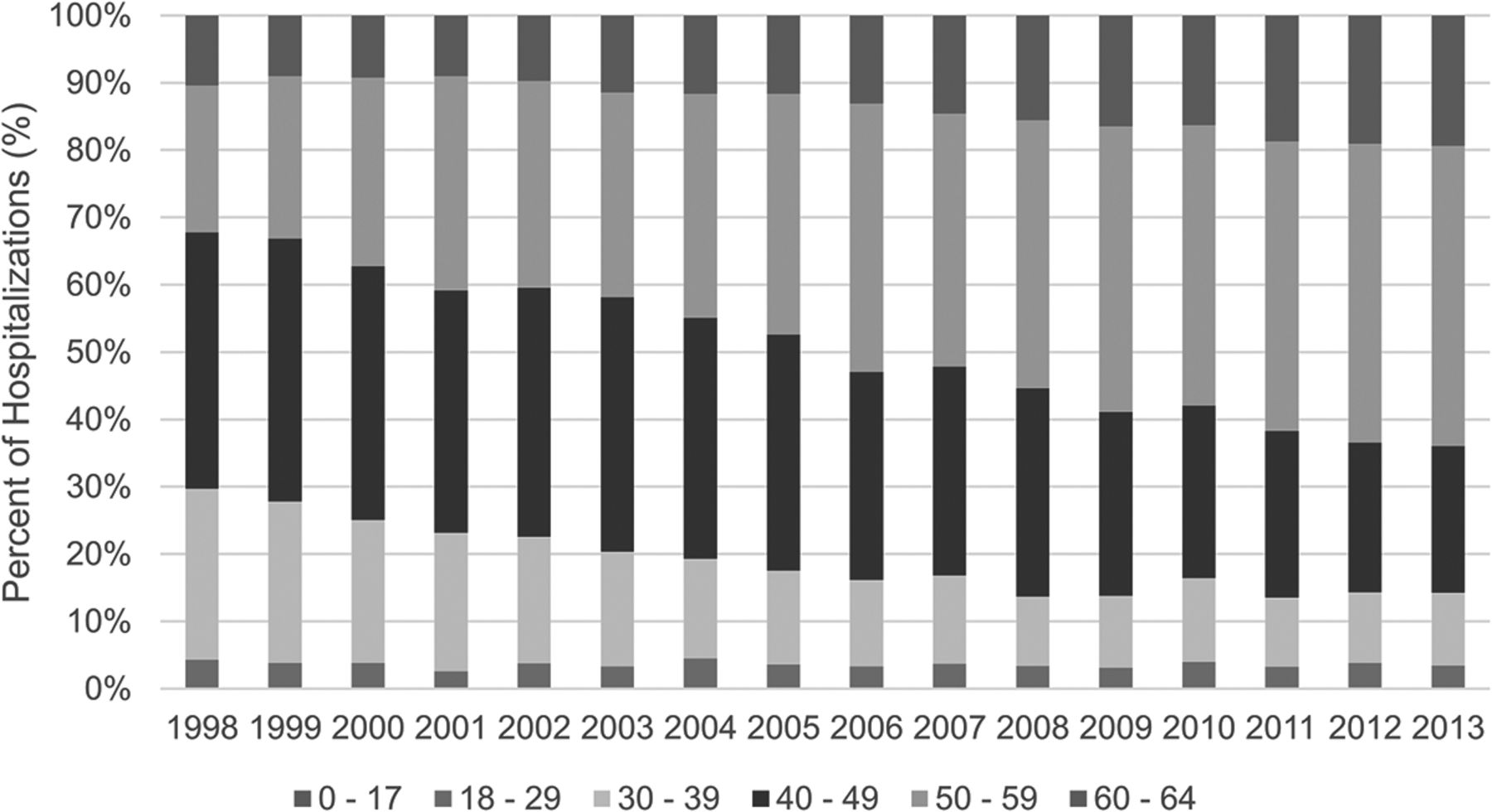
Opioid overdose hospitalizations: patient age among medicare-disability beneficiary (MDBs) (National Inpatient Sample, 1998 to 2013). The 0 to 17 age-group constitutes a very small proportion of the overall population and may not, therefore, be visible graphically.
Overdose Type
Among patients who were hospitalized for opioid overdose, the proportion of hospitalizations among MDBs attributable to NHOD (vs HOD) significantly increased from 87.5% in 1998 to 93.9% in 2013 (trend, P < .0001), and the proportion among non-Medicare-insured patients significantly increased from 69.3% in 1998 to 77.6% in 2013 (trend, P < .0001). Although the trend was greater among MDBs than among nondisabled Medicare beneficiaries, this difference was nonsignificant due to the Bonferroni correction (P = .0038). In 2013, NHODs accounted for a significantly greater proportion of MDB hospitalizations than non-Medicare-insured hospitalizations (P < .0001) (Figure 4; Appendix Table 3).

Non-heroin opioid overdose (NHOD): percentage among those <65 years of age, by payer type (National Inpatient Sample, 1998 to 2013). MDB, Medicare-disability beneficiary.
Comorbidities among MDBs Versus Non-Medicare-Insured Patients Under 65 Years of Age
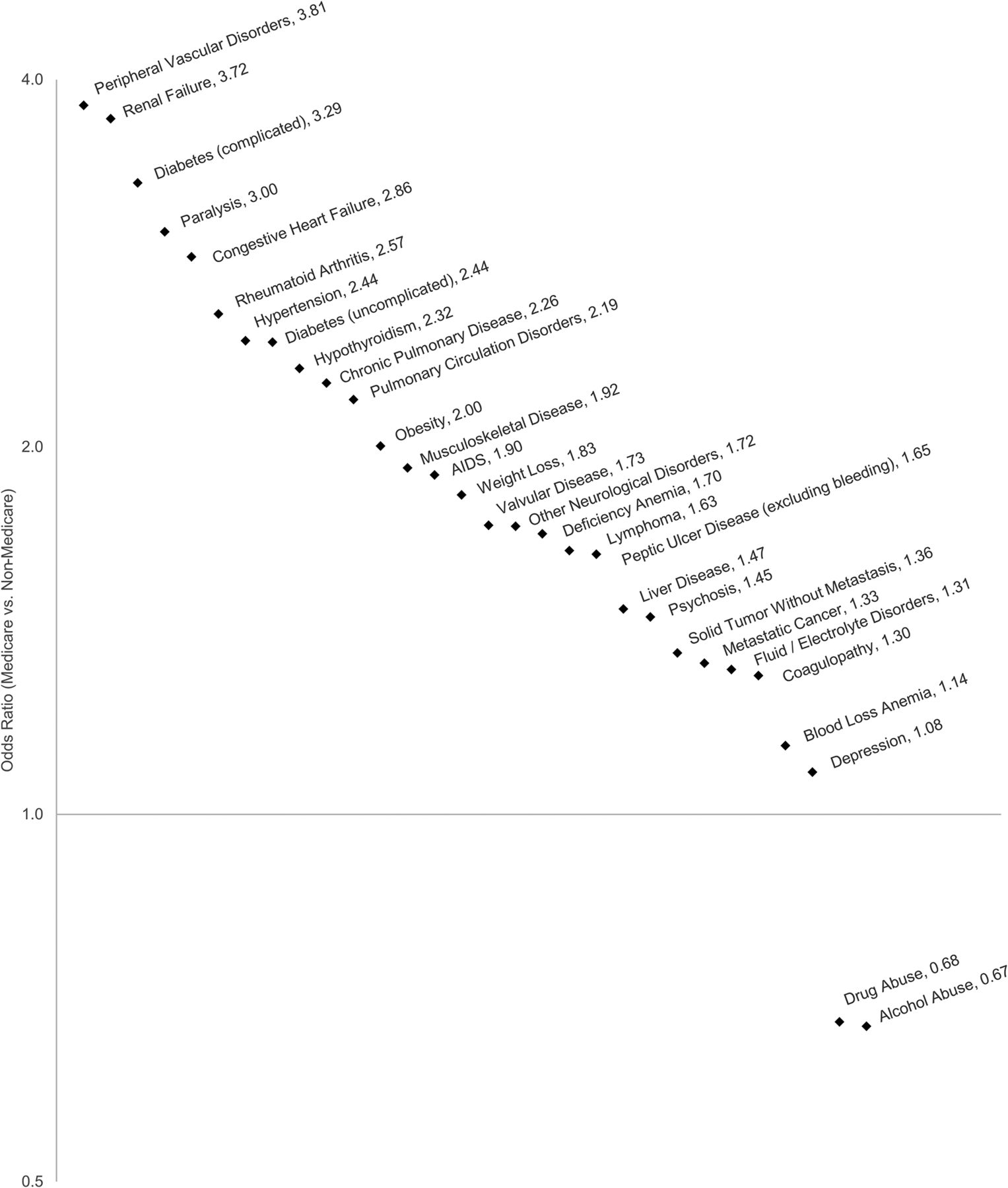
Out of 30 analyzed comorbidities (29 chronic Elixhauser-defined comorbidities and musculoskeletal disease), 26 were more prevalent among MDBs versus non-Medicare-insured patients (P < .0001 for all comparisons). Two comorbidities (blood loss anemia and peptic ulcer disease) failed to show statistical significance between the 2 groups. Notably, drug abuse and alcohol abuse were significantly less common among MDBs versus non-Medicare-insured patients (P < .0001 for both comparisons). The greatest relative differences were observed for peripheral vascular disorders (odds ratio [OR], 3.81; 95% CI, 3.45–4.21; P < .0001 for MDBs vs non-Medicare-insured), renal failure (OR, 3.72; 95% CI, 3.50–3.95; P < .0001), complicated diabetes (OR, 3.29; 95% CI, 3.06–3.54; P < .0001), and paralysis (OR, 3.00; 95% CI, 2.72–3.31; P < .0001). The greatest absolute differences were observed for hypertension (40.6% of MDBs vs 21.9% of non-Medicare-insured patients), chronic pulmonary disease (29.8% vs 15.9%), musculoskeletal disease (23.5% vs 13.8%), and drug abuse (36.8% vs 46.3%) (Figure 5; Appendix Table 4).

Odds ratios for comorbidities among those <65 years of age, by payer type (National Inpatient Sample, 1998 to 2013).
Discussion
This study robustly characterizes opioid overdose hospitalizations among MDBs by using nationally representative data and is the first to compare the frequency of documented comorbidities among MDBs versus non-Medicare insured patients among individuals hospitalized for opioid overdose. Our findings indicate that hospitalizations among MDBs constitute a substantial and growing proportion of opioid overdose hospitalizations in the United States, from 11.7% of those under age 65 hospitalized for opioid overdose in 1998 to 24.5% in 2013; this relative increase of +109% is far greater than the +52% growth in the proportion of those under age 65 with Medicare disability insurance.17,18 The percentage of female patients grew disproportionally among this cohort. The proportion of patients aged 50 to 64 years grew significantly among both MDBs and non-Medicare insured patients. Despite a marked growth in the proportion of white patients among those without Medicare insurance, white patients still constituted a larger proportion of discharges among MDBs. Prescription opioids accounted for a growing proportion of overdose hospitalizations within both cohorts but accounted for a greater percentage of hospitalizations among the MDB cohort than among the non-Medicare-insured cohort. MDBs generally exhibited greater comorbidity burden versus non-Medicare-insured patients under age 65; however, drug and alcohol abuse were less commonly documented among the Medicare cohort.
To qualify for Medicare under age 65, an individual must have been diagnosed with end stage renal disease or amyotrophic lateral sclerosis or have received 24 months of Social Security Disability benefits for another qualifying disability.12 Among all MDBs in the United States in 2014, 23% were under age 45, 29% were from 45 to 54 years old, and 48% were from 55 to 64 years old. A total of 48% individuals were female and 67% were white, 17% were black, and 16% were Hispanic, Asian, or of other race.18 The prevalence of conditions that require pain management in the Medicare-disability population is also particularly high; musculoskeletal disorders are most frequently cited as the primary cause of disability among these individuals.13,14 Our comorbidity analysis confirmed that musculoskeletal disorders are highly prevalent among MDBs hospitalized for opioid overdose. In a 5-year retrospective analysis of MDBs, Morden and colleagues15 reported that more than 40% used any amount of opioids and over 20% used opioids chronically. A retrospective claims analysis from 2008 to 2010 found that the prevalence of diagnosed opioid abuse doubled among Medicare members of Humana, Inc.19 Our findings are consistent with previous studies characterizing the high rate of opioid use among MDBs.15,19,20
The percent of females among MDBs hospitalized for opioid overdose markedly increased; by 2013, this cohort was majority female. Prior research has identified the growing impact of the opioid epidemic on females; this may reflect differences in pain management between males and females. The Centers for Disease Control and Prevention reported that from 1999 to 2015, overdose death rates for all drugs rose for both sexes, but females had consistently lower drug overdose death rates than males21; however, drug overdose deaths grew by a larger percentage in women than men.22 Moreover, the Centers for Disease Control and Prevention reported that from 1999 to 2010, prescription opioid deaths grew 5-fold among women and less than 4-fold among men, indicating increased mortality among women using opioids.22 A survey of 2163 individuals on chronic opioid therapy found that women under age 65 had more pain and lower function than men of the same age.23 Furthermore, an analysis of insurance claims between 1997 and 2002 found that women had more pharmacy claims for opioids than men and at higher doses.24
Age is increasing among MDBs hospitalized for opioid overdose. Our results showed that opioid overdoses among MDBs were more likely to involve older patients (particularly 50 to 60 years old). In 1998, approximately one-third of patients were over the age of 50, whereas by 2013, nearly two-thirds were over the age of 50. These results are consistent with literature reporting the increasing age among patients hospitalized for opioid overdose in the United States.25,26 Our analysis also found that among patients under age 65 hospitalized for opioid overdose, MDBs were more likely to have overdosed using prescription opioids than were non-Medicare-insured patients. This is consistent with the high rates of prescription opioid use reported among MDBs,15 and with reported higher prevalence of opioid abuse in individuals with disability than without disability.27
We observed a generally greater comorbidity burden among MDBs versus non-Medicare-insured patients. Drug abuse and alcohol abuse, however, were less commonly documented among MDBs as compared with non-Medicare-insured patients. The specific ICD-9-CM codes for drug and alcohol abuse Elixhauser comorbidities are generally associated with chronic substance abuse. Previous analyses found a lower prevalence of alcohol abuse among individuals with disability, consistent with our findings.27 However, there is a higher reported prevalence of opioid abuse in individuals with disability than those without, suggesting that coding bias may play a role in our finding that drug abuse was less commonly documented among MDBs. Specifically, given the commonality of chronic pain among MDBs, clinicians may be less inclined to identify chronic opioid use as abusive in this population and may rather view it as necessary for appropriate management. The growing proportion of MDBs among those hospitalized for opioid overdose suggests that medically indicated opioid pain control is nevertheless associated with an increased risk of overdose. Increased vigilance for red-flag signs of opioid abuse among those prescribed long-term opioid pain management is highly warranted. An alternate explanation for the finding that MDBs were less likely to have drug abuse as a documented comorbidity is that clinicians may be less likely to document substance abuse among MDBs for fear of medical or administrative repercussions. MDBs have elevated opioid-related in-hospital mortality risk, and a robust understanding of this patient population will be critical for efforts to reduce opioid overdose.20
This study had several limitations. Our use of the NIS captures only opioid overdoses that require hospitalization; this inherently excludes overdose patients who are treated and released from the emergency department, and those that are fatal in the prehospital setting, among others. As a result, although our study can provide comparative relative proportions of patients, these results should not be extrapolated to represent the absolute magnitude of opioid overdoses as a whole. Future studies should be conducted using datasets including outpatient and prehospital overdoses to further evaluate the findings from this study. As with all analyses of administrative datasets, it is possible that our results are affected by coding bias; opioid overdose patients may be coded according to their symptomatic presentation rather than as an overdose proper. For example, a patient presenting with respiratory failure due to opioid overdose could receive only a code for respiratory failure and none for opioid overdose. However, our study improves on comparable investigations in this regard, as we assessed patients with any listed code corresponding to opioid overdose, while select previous investigations have analyzed only patients with a primary ICD-9-CM code for opioid overdose (specific codes listed in Methods). In addition, ICD-9-CM codes provide only limited detail regarding the specific type of opioid involved in overdoses. Accordingly, we were unable to distinguish between various nonheroin opiates, such as fentanyl and carfentanil. These substances have contributed significantly to the opioid epidemic.28,29 Future investigations should be conducted using datasets offering a greater degree of granularity with regard to opioid type.
Further research should be undertaken to inform the prevention and treatment of opioid use disorder among MDBs, as this population may respond differently than the general population. For example, Moyo and colleagues30 found that Prescription Drug Monitoring Programs had a more beneficial impact on MDBs than patients qualifying for Medicare based on age. Characterization of the nature of opioid abuse among these individuals, including whether opioids were prescribed as a component of pain management, may inform efforts to prevent the development of opioid abuse. Additional efforts to optimize recovery paradigms are also needed for this patient population.
To counter the trend of increasing opioid overdoses among MDBs, particular care must be taken to address the unique needs of this population and the individuals of which it is comprised. Some patients may have limited options for alternative treatment or rehabilitation, depending on the patient's Medicare-qualifying condition. Some may have pain that is severe, enduring, and not well managed by any other interventions. Our findings emphasize that the MDB population is a critical subset of patients to address as the opioid epidemic continues.
Appendix
ICD-9-CM Coding Algorithms

Incidence of Opioid Overdose Hospitalization by Age.
Age Distribution of Opioid Overdoses, Overall
Characteristics of Opioid Overdose Hospitalizations Among Patients <65 Years of Age
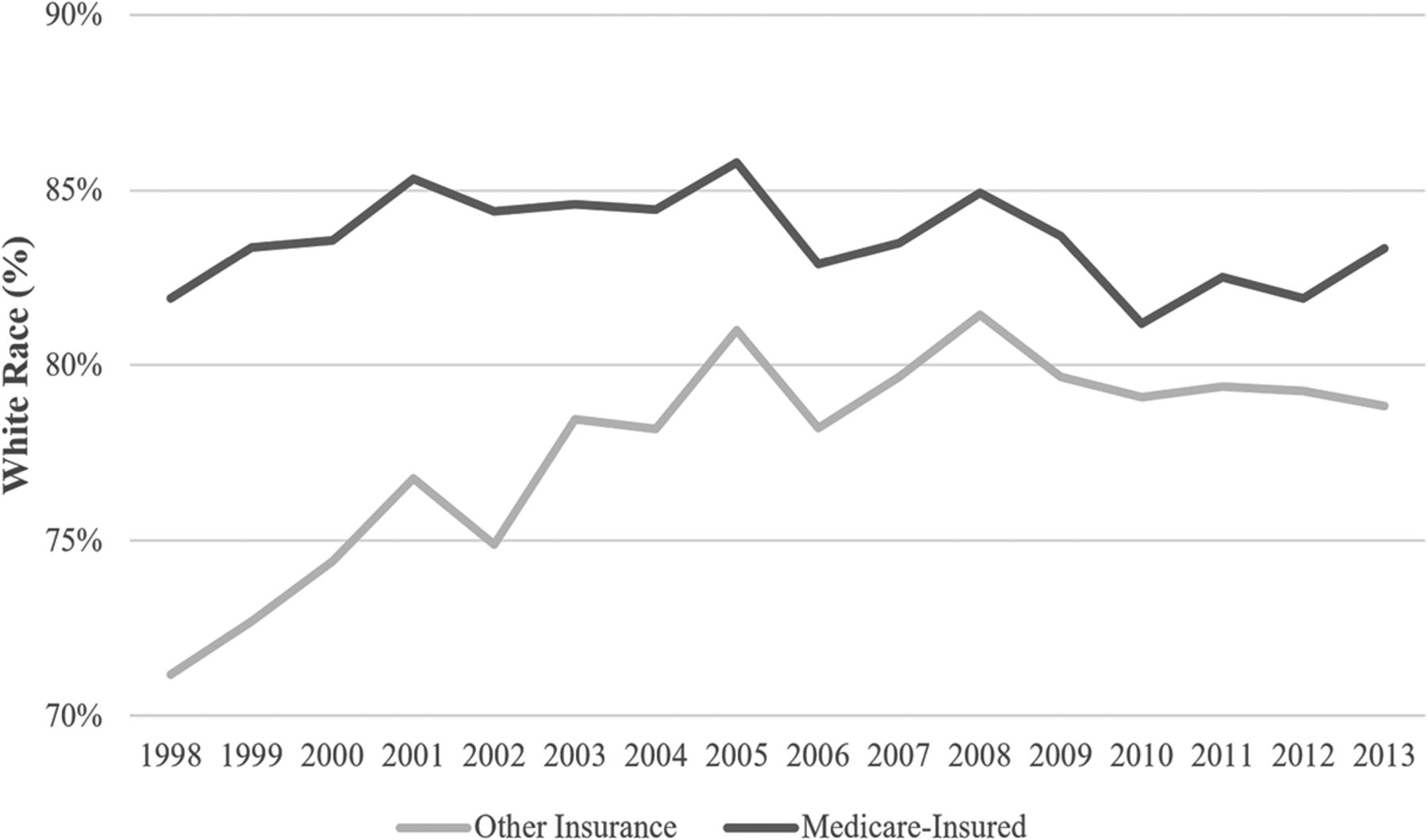
Opioid Overdose Hospitalizations: Percentage of White Patients Among Those <65 years of Age, by Payer Type.
Prevalence of Comorbidities Among Patients <65 y/o
Notes
This article was externally peer reviewed.
Funding: Substance Abuse and Mental Health Services Administration (SAMHSA): Grant funds used to purchase NIS data.
Conflict of interest: JLP and WMD contributed equally to this work.
To see this article online, please go to: http://jabfm.org/content/31/6/881.full.
- Received for publication May 21, 2018.
- Revision received July 4, 2018.
- Accepted for publication August 1, 2018.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}