
Abstract
Background: Cutaneous odontogenic fistulas or sinus tracts are frequently misdiagnosed and incorrectly treated, leading to unnecessary procedures and patient suffering. An understanding of the draining of cutaneous sinus tracts will lead to more appropriate treatment. Most cases respond to conservative, nonsurgical root canal therapy. Our objective is to report 2 cases of cutaneous sinus tract secondary to chronic periapical dental infection that were recently observed at our hospital.
Methods: We present 2 cases of recurrent suppurative facial lesions that were initially misdiagnosed and treated with oral antibiotics without response.
Results: Clinical findings included palpable facial nodules with drainage, palpable intraoral cords, and poor dentition with gingivitis; radiologic examination showed a periapical disease process consistent with dental sinus tracts. Both of the cases were referred to the maxillofacial department, where the cyst and nonrestorable teeth were extracted.
Conclusion: Because patients with cutaneous facial sinus tracts of dental origin often do not have obvious dental symptoms, a possible dental etiology may be overlooked. If dental origin is suspected, the diagnosis is easily confirmed by dental examination and dental roentgenograms of the involved area. Early correct diagnosis, based on radiologic evidence of a periapical root infection and treatment of these lesions can help prevent unnecessary and ineffective antibiotic therapy or surgical treatment, reducing the possibility of further complications such as sepsis and osteomyelitis.
Cutaneous odontogenic fistulas or sinus tracts have been well documented in the medical literature.1⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–15 However, they are frequently misdiagnosed and incorrectly treated, leading to unnecessary procedures and patient suffering. Cutaneous, rather than intraoral, lesions are likely to occur as a result of pulpal necrosis and suppurative apical periodontitis. Since many patients have no dental symptoms, a high degree of suspicion is required to make the correct diagnosis. We report 2 cases of cutaneous sinus tract secondary to chronic periapical dental infection that were recently observed at our hospital.
Case Reports
Case 1
A 45-year-old man presented to us for evaluation of a “pyogenic granuloma.” The patient reported a 2-month history of a drained and recurrent abscess in his face. He had a personal history of “gum boils” and had been previously treated with antibiotics for this condition, without response. Examination revealed a nodule with crusting and surrounding induration on his right mandible (Figure 1). A dental origin was suspected. Computed tomography revealed focal depression and hyperdensity in subcutaneous cellular tissue in the right mandibular region. The patient was referred to maxillofacial surgery, where extraction of the remains of several roots and surgical excision of fibrosis on his right mandible mucosa was performed. The patient was lost to follow-up.

Suppurative nodule with crusting and surrounding induration on the right mandible.
Case 2
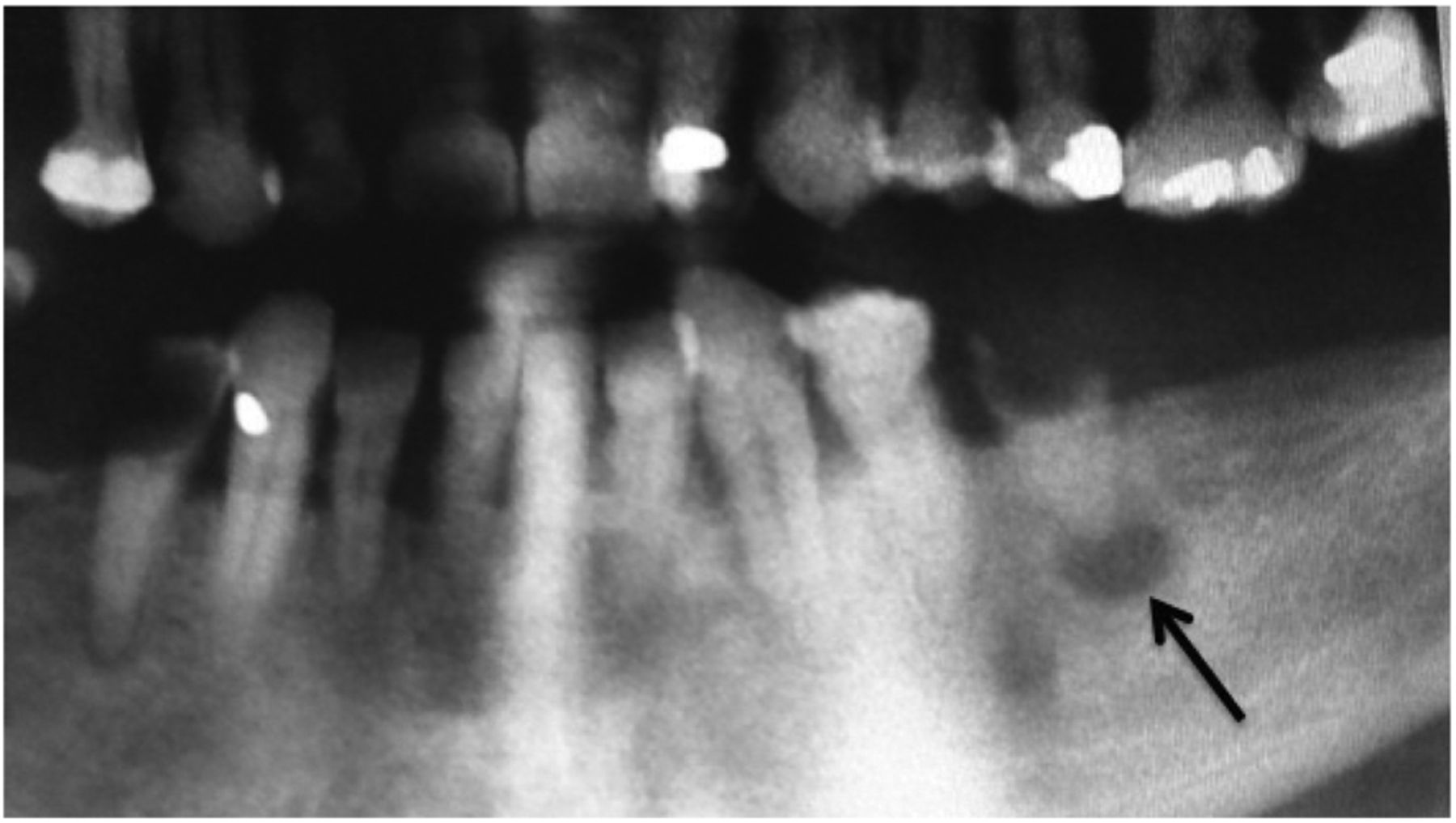
A 62-year-old man presented with a chronically draining cutaneous lesion on his left face, diagnosed as a furuncle. Physical examination revealed an indurated area with thickening of subcutaneous tissues and skin retraction on the left mandible (Figure 2). Intraoral examination was remarkable for poor dentition and gingivitis. A dental radiograph revealed diffuse radiolucency at the apex (consistent with a chronic periapical abscess), as well as radicular remains involving the root of the mandibular left premolar (Figure 3). It was too late to be corrected with endodontic treatment; therefore the tooth as well as the cyst were extracted by a maxillofacial surgeon. The dental sinus healed soon after treatment.

Indurated area with thickening of subcutaneous tissues lesion and skin retraction on the left mandible.
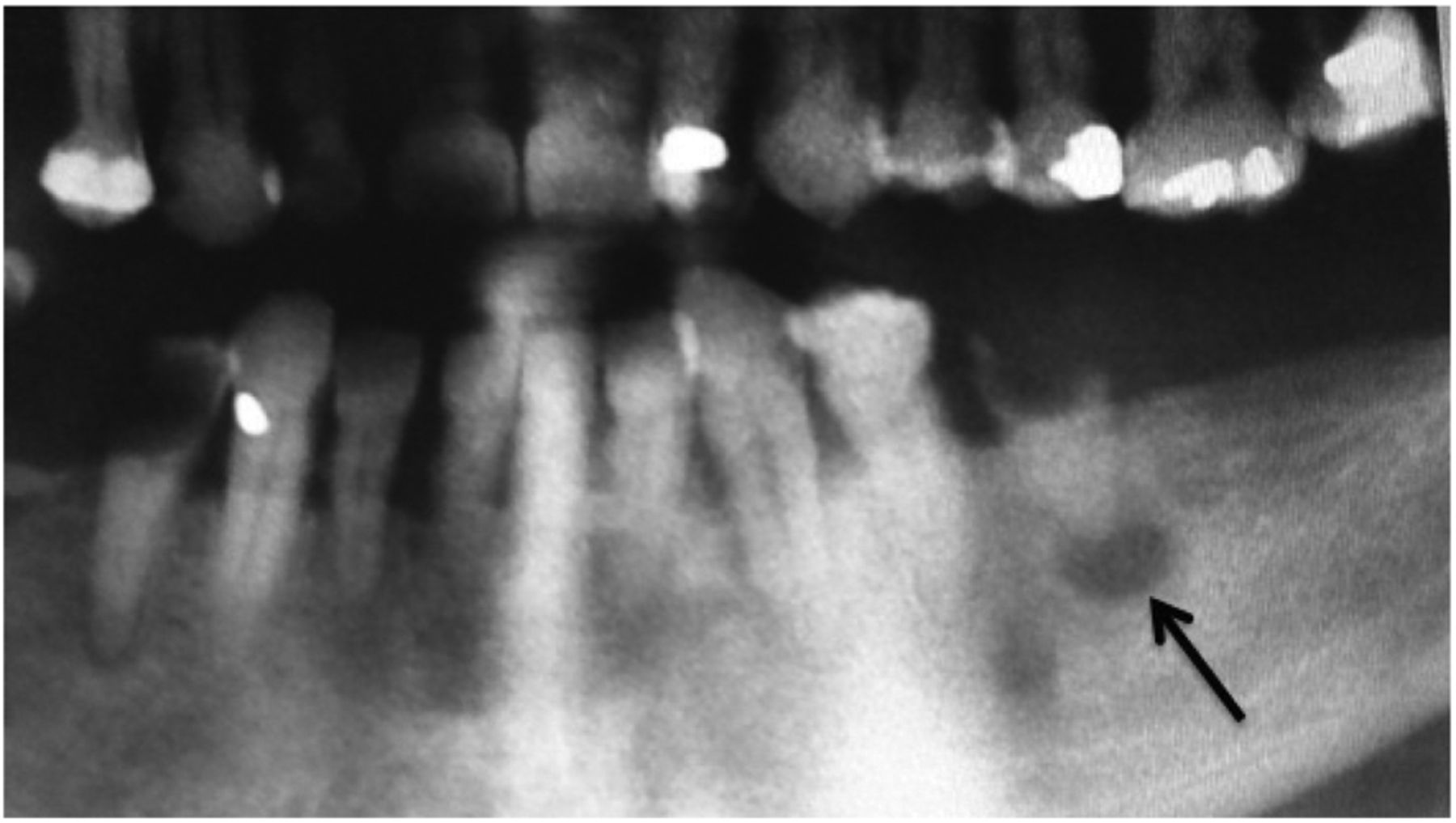
Diffuse radiolucency at the apex and radicular remain involving the root of the mandibular left premolar.
Discussion
Suppurative dental infections, osteomyelitis, infected cysts, and tubercular or fungal infections are common conditions leading to the formation of cutaneous sinuses or abnormal blind tracts arising from or terminating in an opening.14 The most common cause of draining cutaneous sinus tracts on the face is a chronic periradicular abscess. Cutaneous lesions may occur early or up to 30 years after a primary dental problem has occurred.8,9
Cutaneous odontogenic sinus is an uncommon disease and may be easily misdiagnosed. An injury or disease of the tooth may result in degeneration of the pulp and periapical abscess. The local destructive process progresses slowly through the alveolar bone and may spread into the surrounding soft tissues and erupt through the skin. Findings consistent with dental sinus tracts are palpable and painless facial nodule or pustule with or without drainage. Retraction or dimpling is caused by fixation with the underlying tissues and may be associated with a palpable intraoral cord.1,8 Only half of patients have reported a history of toothache.5
The majority of dental sinus tracts develop intraorally. When an extraoral odontogenic sinus tract occurs, it most often develops in close proximity to the offending tooth. Patients often seek treatment from a physician and present with chronic suppurative lesions that resemble a cyst, furuncle, or ulcer.7 The most common sites for a cutaneous sinus of dental origin are the chin and the jaw.1,2 The sinus tract's exit is determined by the location of muscle attachments and fascial planes.2,6 Of the reported cases, 80% arise from mandibular teeth. Mandibular incisors and cuspids typically drain to the chin or submental region. Mandibular premolar and molar infections drain to the posterior mandible or below the inferior border in the submandibular region. Dental fistulas may arise from infection of the maxillary teeth, resulting in sinus tracts erupting intranasally or the nasal sinus or inner canthal areas.2,5 Tracts in the mandibular, submandibular, and neck regions are most often associated with disease of the mandibular molars. Osteomyelitis is a rare complication. A dental etiology should be suspected in chronic draining sinus tracts of the face and neck.
Diagnosis is established by tracing the sinus tract with gutta-percha or similar radiopaque material, dental examination, and radiologic evaluation.6 Dental panoramic or periapical radiographic views reveal evidence of a radiolucent periapical disease process. Patients should be evaluated with orthopantomography and, if possible, with cone-beam computed tomography. The pulp vitality test should be used to determine whether the diseased tooth is restorable.14 Histologically, the cutaneous sinus usually consists of granulomatous tissue or epithelium.11 Diagnostic errors can result in multiple surgical excisions and biopsies, antibiotic therapy, and even radiation therapy.
Differential diagnosis of nodulocystic lesions of the chin and mandibular region include local physical trauma, foreign body reaction, pyogenic granuloma, squamous cell carcinoma, basal cell carcinoma, metastatic tumor, actinomycosis, deep mycoses, chronic tuberculosis or atypical mycobacteria, gumma of tertiary syphilis, salivary fistulae, lymphadenitis, as well as developmental defects such as branchial cleft cysts or thyroglossal ducts.9,11
An understanding of the draining of cutaneous sinus tracts leads to more appropriate treatment. Most cases respond to conservative, nonsurgical root canal therapy.5 Endodontic treatment is recommended. Extraction may be required in nonrestorable fractured or carious teeth, or in cases associated with extensive alveolar bone loss2,5 The retention of natural teeth preserves function, arch integrity, and esthetics, and eliminates the need for a costly restorative procedure. After appropriate dental therapy the sinus tract resolves spontaneously within a few weeks, but a retracted dimple or scar may develop. Because odontogenic sinus trace is a localized entity, systemic antibiotic administration is not indicated in healthy patients. The sinus tract will recur unless the source of infection has been eliminated.5,6
Conclusion
Because patients with cutaneous facial sinus tracts of dental origin often do not have obvious dental symptoms, a possible dental etiology may be overlooked. If a dental origin is suspected, the diagnosis is easily confirmed by dental examination and dental roentgenograms of the involved area. Early correct diagnosis, based on radiologic evidence of a periapical root infection, and treatment of these lesions can help prevent unnecessary and ineffective antibiotic therapy or surgical treatment, reducing the possibility of further complications such as sepsis and osteomyelitis.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication February 3, 2015.
- Accepted for publication May 1, 2015.




{kind=link}
{kind=link}
{kind=link}