
Abstract
The past few years have seen numerous additions and modifications to the current immunization schedules. Starting with the 2010 to 2011 influenza season, the Centers for Disease Control and Prevention have recommended universal annual influenza vaccination for all persons without a contraindication who are 6 months of age and older, including healthy persons aged 19 to 49 years. Hepatitis B vaccination is now recommended for all susceptible diabetics ≤60 years of age. One dose of tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccine, adsorbed, is recommended to replace one tetanus and diphtheria toxoids adsorbed (adult) vaccination for all adults, including those 65 years of age or older, who are anticipating contact with infants and unvaccinated pregnant women (preferably during the second or third trimester). All adult vaccines remain underused. This article will summarize the most recent changes in the adult immunization recommendations of the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention.
Rates of vaccination of adults have consistently fallen behind vaccination rates for children and adolescents. The Centers for Disease Control and Prevention (CDC) analyzed data from the 2010 National Health Interview Survey to assess adult vaccination rates and found them to be low for most routinely recommended vaccines. Rates of the 3 vaccines included in Healthy People (HP) 2020—pneumococcal, herpes zoster, and hepatitis B (for health care personnel [HCP])—were well below the respective target levels: for pneumococcal vaccine, rates in 2010 were 59.7% for persons aged >65 years (HP2020 target of 90%) and 18.5% for persons at high risk aged 18 to 64 years (HP2020 target, 60%); for herpes zoster vaccine, rates were 14.4% for persons aged ≥60 years (HP2020 target, 30%); and for the hepatitis vaccine for HCP, the rates were 63.2% (HP2020 target, 90%). For adults for whom tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccine, adsorbed (Tdap) status could be assessed, coverage was only 8.2%; for HCP Tdap coverage was 20.3%.1
The CDC estimated that 40,000 to 50,000 vaccine-preventable deaths occur every year in the United States and estimates the health care burden of vaccine-preventable diseases at $10 billion.2 Family physicians are specialists in preventive care and can be leaders in seeing that adult patients get the full benefit of protection against vaccine-preventable diseases. This article summarizes the most significant recent changes in the US adult immunization schedule.
Influenza Vaccine
Universal Influenza Immunization
Since the 2010 to 2011 flu season, the CDC has recommended that all persons should be immunized annually against influenza, starting from the age of 6 months, which is the youngest age for which any influenza vaccine is approved. The 2011 to 2012 US seasonal influenza vaccine virus strains are identical to those contained in the 2010 to 2011 vaccine and includes the 2009 pandemic influenza A (H1N1) vaccine virus strain.3
Available Influenza Vaccines
There are 2 types of influenza vaccine available for administration to adults: the trivalent inactivated influenza vaccine (TIV) and the live attenuated influenza vaccine (LAIV). LAIV is administered intranasally and contains the same influenza viruses as TIV. The live viruses in LAIV are temperature sensitive and do not replicate effectively at the human core body temperature; thus, they cannot produce disease. However, the LAIV viruses are adapted to cold, which enables them to replicate in the slightly cooler temperature of the nasopharyngeal mucosa and produce immunity. A recent meta-analysis comparing TIV with LAIV concluded that LAIV seems to be slightly more effective than TIV in children.4 Studies comparing TIV with LAIV in adults have shown conflicting results.5,6 The CDC has stated that both TIV and LAIV have been demonstrated to be effective in children and adults and that there is insufficient data directly comparing the effectiveness of these 2 types of influenza vaccines to identify whether one vaccine might offer a clear advantage over the other in a particular population.3 LAIV is not approved for adults ≥50 years of age and may not be given to pregnant women or persons who are immunocompromised, which includes those with chronic pulmonary (including asthma), cardiovascular (except hypertension), renal, hepatic, neurological/neuromuscular, hematologic, or metabolic (including diabetes) disorders or with immunosuppression (including that caused by medications or HIV).
A new influenza vaccine, trivalent influenza vaccine intradermal (TIVI) (Fluzone Intradermal, Sanofi Pasteur, Swiftwater, PA), was licensed in May 2011. This vaccine is indicated for persons aged 18 through 64 years and is administered intradermally via a single-dose, prefilled microinjection syringe. TIVI contains 9 μg of each flu strain in 0.1 mL total volume versus intramuscular TIV preparations, which contain 15 μg of each strain in 0.5 mL total volume. The preferred site for administration is over the deltoid muscle. The most common adverse reactions are local: erythema, induration, swelling, pain, and pruritus. With the exception of pain, these reactions occurred more frequently than with the intramuscular vaccine but generally resolved within 3 to 7 days.7 The CDC has not indicated a preference for this vaccine over other influenza vaccines.3
Trivalent influenza vaccine high dose (TIVHD; Fluzone High-Dose, Sanofi Pasteur), available since the 2010 to 2011influenza season, contains 60 μg of hemagglutinin per vaccine strain (rather than 15 μg per strain as in other TIV preparations). TIVHD is available as an alternative TIV for persons aged ≥65 years. The rationale for the higher antigen dose is to stimulate a better antibody response in the elderly, who have a weaker response to influenza vaccines because of immunosenescence. The CDC has indicated no preferential recommendation for this vaccine over other influenza vaccines indicated for use in the elderly.3
A web page listing influenza vaccines available in the United States for the current influenza season and their age indications is available at http://www.immunize.org/catg.d/p4072.pdf (Acquired from Immunization Action Coalition on April 22, 2012); the link is updated continuously to match current recommendations and availability.
Pneumococcal Polysaccharide Vaccine
Pneumococcal disease causes significant illness and death worldwide. The most serious manifestations of illness are pneumonia, pneumococcal sepsis and meningitis. In 2005 the World Health Organization estimated that 1.6 million persons died of pneumococcal disease throughout the world, mainly the elderly and small children.8 In 2005 in the United States, more than 40,000 cases and more than 4,400 deaths from invasive pneumococcal disease (IPD; bacteremia and meningitis) were estimated to have occurred. More than half of these cases occurred in adults for whom the pneumococcal polysaccharide vaccine was indicated.9
Pneumococcal polysaccharide vaccine (23-valent) (PPSV23; Pneumovax 23, Merck, Whitehouse Station, NJ) was licensed in 1983. It contains antigens against strains that account for 88% of pneumococci that cause sepsis. The vaccine is recommended for all persons 65 years of age and older and also is recommended for certain high-risk groups (see Table 1). In 2008 the CDC added smokers and asthmatics aged 19 to 64 years to the high-risk list because these groups have an increased risk of IPD. Observational studies generally have shown that PPSV23 is 50% to 80% effective in preventing IPD in immunocompetent adults and that it may reduce the severity of pneumonia in those patients who develop pneumonia after vaccination.10 Recent studies even have indicated that pneumococcal vaccination may prevent myocardial infarction and stroke by reducing thrombosis caused by inflammation.11⇓–13
Persons who are immunocompromised, such as HIV patients or cancer patients undergoing chemotherapy or radiation therapy, have a particularly high rate of IPD. Health care workers administering PPSV23 should be proactive and have patients newly diagnosed with any malignancy vaccinated immediately upon diagnosis because a full immune response to the vaccine requires at least 2 weeks and is weakened by chemotherapy or radiation therapy.9 If chemotherapy or radiotherapy is initiated less than 2 weeks after administering PPSV23, the CDC recommends that the patient be considered unvaccinated, and should be revaccinated at least 3 months after therapy is discontinued if immune competence has been restored.
Persons ≥65 years of age who have had one prior dose of PPV23 should receive a second dose if ≥5 years have elapsed since the previous dose. Only one revaccination dose of PPV23 is recommended for certain high-risk persons (see Table 1); a third dose is not presently recommended by the CDC because of a lack of proven efficacy.9 However, some recent studies have shown a good antibody response to a primary and booster dose of PPSV23.14⇓–16
In December 2011, the US Food and Drug Administration (FDA) approved a pneumococcal 13-valent conjugate vaccine (PCV13; Prevnar 13, Wyeth Pharmaceuticals, Radnor, PA) to help protect adults aged 50 and over from pneumococcal pneumonia. At this time the optimal use of PCV13 in adults, alone or in a series with PPV23, has not been determined.17
Recognizing the importance of pneumococcal immunizations, the Centers for Medicare & Medicaid Services has added screening for and administration of pneumococcal immunization as a quality measure for hospital inpatients. Beginning January 1, 2012, rates of pneumococcal immunization will be assessed for all inpatients ≥65 years of age and inpatients 5 to 64 years of age with high-risk conditions.18 After October 2013, reported data will be available to the public at http://www.hospitalcompare.hhs.gov/. (See Table 2 for Level of Evidence [LOE].)
Herpes Zoster Vaccine
Varicella zoster virus (VZV) causes 2 clinical conditions. The first, varicella (chickenpox), was widespread in childhood before the era of varicella vaccination and has infected 98% of the adult US population. The virus travels through affected sensory nerves to the sensory dorsal root ganglia next to the spinal cord, where it enters a latent phase. The second stage, herpes zoster, occurs when the virus reactivates in one dorsal root ganglion and travels back to the skin, where it causes a localized unilateral vesicular rash.19 Reactivation seems to be related to declining cell-mediated immunity and is more common with advancing age and in patients with immunosuppressive conditions such as neoplastic disease, organ transplant recipients, persons receiving immunosuppressive medication, and HIV patients.20 Pain is the most common symptom of herpes zoster, affecting about 75% of cases. Lingering pain after a zoster infection is called postherpetic neuralgia (PHN) and is commonly defined as pain lasting more than 1 to 3 months after the primary infection. PHN can be excruciatingly painful and can last for months and occasionally for years. Antiviral therapy after the onset of shingles has not shown efficacy for the prevention of PHN.21
The herpes zoster (shingles) vaccine (ZOS; Zostavax, Merck), was approved by the FDA in May 2006 for use in persons ≥60 years of age. Although the FDA licensed ZOS for use in adults aged 50 to 59 years in March 2011, the Advisory Committee on Immunization Practices (ACIP) so far has declined to extend a formal recommendation for this age range because of concerns about limitations in the vaccine supply and uncertainty about the duration of the vaccine's protection in younger adults.22 ZOS is similar to the varicella vaccine (VAR; Varivax, Merck); it is made from the live-attenuated Merck-Oka viral strain but contains 14 times as much viral antigen as is present in varicella vaccine. In the Shingles Prevention Study, more than 38,000 adults (median age, 69 years; range, 59–99 years) were followed for a mean of 3.1 years after receiving either vaccine or placebo. Vaccination with ZOS reduced the incidence of herpes zoster by 51% and the incidence of PHN by 66%.19,23 Side effects were mild, and there was no significant increase in serious adverse events in the vaccine group when compared with the placebo group. A subsequent cohort study found ZOS to be as effective, and in some subpopulations, more effective, than was indicated by the Shingles Prevention Study.24
ZOS is recommended by the ACIP for all adults 60 years of age and older (LOE: A; see Table 2).19 A history of zoster is not a contraindication to vaccination because there is no way to document the level of herpes zoster immunity and vaccine side effects are minimal. In addition, immunization will give additive immunity against shingles; this may be particularly important in view of a recent study indicating higher rates of recurrence of shingles than previously believed.3 ZOS is an attenuated live-virus vaccine and is not indicated for persons with certain immune-suppressing conditions (see Table 3).
A study showing a reduced VZV antibody response when ZOS was given simultaneously with PSV23 (Pneumovax) led the manufacturer to recommend that these 2 vaccines should not be given simultaneously and that there should be a 4-week interval between administration of the 2 vaccines.25 However, the CDC continues to recommend that these vaccines be given simultaneously, if indicated, because VZV immunity is cell mediated and does not correlate well with antibody levels.22,26 This is supported by an observational study published in 2011 that found no evidence that simultaneous administration of the 2 vaccines would impair zoster immunity.27 (See Table 2 for Level of Evidence.)
Human Papillomavirus Vaccine
Human papillomavirus (HPV) is estimated to be the most common sexually transmitted disease; more than 80% of sexually active American women will acquire an HPV infection by the age of 50 years with seroprevalence of HPV type 16 (the most carcinogenic type) as high as 41%.28 HPV is responsible for more than 99% of cervical cancer and is believed to be responsible for 90% of anal cancers and 40% of vulvar, vaginal, or penile cancers.29 In developed countries, HPV has passed tobacco use to become the major cause of oropharyngeal cancer (found in 45% to 90% of cases).30 Four HPV types account for the most serious illness: high-risk types 16 and 18 are found in 70% of cervical cancers, and low-risk types 6 and 11 cause 90% of genital warts. HPV type 16 is responsible for >85% of HPV-related head and neck squamous cell cancers.30 Most HPV infections clear within 8 months to 2 years, but high-risk HPV subtypes are more likely to persist and lead to precancer and cancer. Progression from high-grade precancerous lesions to cancer is estimated to take 10 years.31
Two vaccines are available to prevent HPV infections. HPV4 (Gardasil, Merck) contains types 16 and 18 (high risk) and types 6 and 11 (low risk). HPV2 (Cervarix, GlaxoSmithKline, Research Triangle Park, NC) contains types 16 and 18 (high risk). Both HPV2 and HPV4 are composed of virus-like particles prepared from the recombinant L1 capsid protein of HPV—neither is a live vaccine. Both vaccines have shown efficacy well over 90% for preventing precancerous cervical lesions.32
HPV4 vaccine is licensed for girls and young women 9 through 26 years of age for the prevention of cervical, vulvar, vaginal, and anal cancers caused by HPV types 16 and 18; genital warts caused by HPV types 6 and 11; and precancerous or dysplastic lesions caused by HPV types 6, 11, 16, and 18. As of October 2011, HPV4 also is recommended by the ACIP for boys and men 9 through 21 years of age for the prevention of anal cancer caused by HPV types 16 and 18; for the prevention of anal dysplasias and precancerous lesions caused by HPV types 6, 11, 16, and 18; and for the prevention of genital warts caused by HPV types 6 and 11. The ACIP also recommends HPV4 for previously unvaccinated men 22 to 26 years of age who are immunocompromised, who test positive for HIV infection, or who have sex with men. However, any man may receive the vaccine through age 26 if desired. The HPV2 vaccine is licensed for girls and women ages 10 through 25 years for the prevention of cervical cancers and precancers. The ACIP recommends the same age range, 9 to 26 years of age, for both HPV2 and HPV4. If a man or woman reaches age 27 before the vaccination series is complete, the vaccine series may still be completed if it had been started before the 27th birthday.32 The ACIP recommends the same 3-dose schedule for either vaccine. Each dose is 0.5 mL and is administered intramuscularly. The second dose is administered 1 to 2 months after the first dose, and the third dose is administered 6 months after the first dose. The ACIP has not expressed a preference for one HPV vaccine over the other for vaccination of women.
Although HPV vaccines are not recommended to be given during pregnancy, testing for pregnancy is not necessary before giving the vaccine, and no intervention is needed if a patient is found to be pregnant after receiving HPV vaccine. Women receiving the HPV vaccine should be counseled to continue routine Papanicolaou screening for cervical cancer according to existing guidelines. Although it is biologically plausible that HPV2 and HPV4 could prevent oropharyngeal cancers, it may take several decades before this effect could be detectable in population studies30 (see the box titled, “Can HPV Vaccination Prevent Cancer of the Head and Neck?”). Information about administration, precautions, and contraindication are listed in Table 2.
Tetanus–Diphtheria–Pertussis Vaccine
Tetanus and diphtheria have become rare in the United States, and most cases occur in adults who have not completed a primary immunization series. However, pertussis, a coughing illness caused by the bacteria Bordetella pertussis, remains an endemic disease, with the true number of cases estimated to be between 800,000 and 3.3 million annually in the United States.40 Pertussis incidence has been increasing gradually since the early 1980s. More than 25,000 cases were reported in 2004, the largest number since 1959.41 In 2010, 9,143 cases of pertussis (including 10 infant deaths) were reported throughout California. This is the most cases reported in 63 years, when 9,394 cases were reported in 1947.
Adolescents and adults serve as a reservoir of disease because pertussis immunity wanes 4 to 12 years after the completion of childhood vaccination.42 Giving a booster dose of pertussis vaccine to adults is considered essential to reduce the burden of disease and protect newborns from infection, especially during the vulnerable first 2 months of life before the first pertussis vaccination.
Vaccines containing acellular pertussis were first licensed for use in adolescents and adults in 2005. Tdap is written with small d and p letters to indicate that the dose of diphtheria and acellular pertussis toxoid in the vaccine has been reduced in the adolescent/adult formulations to minimize the incidence of adverse effects. Two Tdap vaccines are currently available. Boostrix (GlaxoSmithKline) is approved for persons 10 through 64 years of age. Adacel (Sanofi Pasteur) is approved for persons 11 through 64 years of age. In response to the 2010 pertussis epidemic in California, the ACIP voted on October 27, 2010, to approve the off-label use of Tdap in adults aged ≥65 years who anticipate contact with children aged ≤12 months to protect both themselves and the infant.43
The ACIP recommends that Tdap should replace a single dose of the tetanus–diphtheria vaccine (Td) for adults aged ≥19 years or older who have not previously received a dose of Tdap. Tdap also can be substituted for any Td dose in the 3-dose primary series. A dose of Tdap is recommended for pregnant women (preferably given in the third or late second trimester), postpartum women, those with close contacts with infants aged <12 months, and all HCP with direct patient contact if they have not previously received Tdap. When giving Tdap to protect an infant, no minimum interval needs to be adhered to; a dose of Tdap can be given immediately after a dose of Td in such cases.44 Ideally, these adults should receive Tdap at least 2 weeks before they are in close contact with the infant. Tdap, if given during pregnancy, preferably should be administered during the third or late second trimester (after 20 weeks' gestation). If not administered during pregnancy, Tdap should be administered immediately postpartum.43
Meningococcal/Varicella/Measles–Mumps–Rubella/Polio/Hepatitis A/Hepatitis B
Some adults will require catch-up vaccination with these vaccines, particularly HCP and travelers. A summary of ACIP recommendations for immunization of HCP can be found in Table 4.45 Key updates are given below.
Meningococcal
Two quadrivalent meningococcal conjugate vaccines (MCV4) are now available: Menactra (Sanofi Pasteur), for persons aged 2 to 55 years, and Menveo (Novartis, East Hanover, NJ), for persons aged 11 to 55 years. A quadrivalent meningococcal polysaccharide vaccine (MPSV4), Menomune (Sanofi Pasteur), still is available for use in adults ≥56 years of age.
The ACIP now recommends revaccination with MCV4 after 5 years for adults previously vaccinated with MCV4 or MPSV4 who remain at increased risk for infection (eg, adults with anatomic or functional asplenia or microbiologists or travelers with prolonged exposure). Either MCV4 vaccine may be used to revaccinate people aged 11 to 55 years who need a second dose, regardless of which vaccine was used for the first dose.46 In addition, the ACIP has now recommends a booster dose 5 years after the first MCV4 dose for those who received their initial dose at ages 13 to 15.47 These changes were made because antibody levels were found to decline over time, and people ages 16 to 21, particularly college freshmen living in dormitories, are considered to be at increased risk for meningococcal disease. However, college freshmen who were vaccinated at age ≥16 years do not need revaccination unless they are also in a high-risk category.
Varicella
All healthy adults should be assessed for varicella immunity. Evidence of immunity includes documentation of age-appropriate vaccination, laboratory evidence of immunity (or confirmation of disease), or diagnosis of varicella or zoster by a health care provider. Birth in the United States before 1980 is considered evidence of immunity, except for HCP, pregnant women, and immunocompromised persons, who require other evidence of immunity. Those who do not have evidence of immunity should receive 2 doses of single-antigen varicella vaccine 4 to 8 weeks apart. Varicella vaccination should be considered for HIV-infected adults with a CD4+ T-lymphocyte count of ≥200 mm3; these individuals should receive 2 doses separated by 3 months.48 Pregnant women should be screened for varicella immunity; one dose given postpartum when indicated, with a second dose 4 to 8 weeks later.
Hepatitis A
A hepatitis A/hepatitis B combination vaccine—Twinrix (GlaxoSmithKline)—can be given in an accelerated 4-dose schedule to protect travelers who need to depart in less than 1 month. Doses are given at 0, 7, and 21 days and 12 months.49
For unvaccinated adults who are acutely exposed to the hepatitis A virus or are traveling to areas of high prevalence who do not have time to complete a 2-dose hepatitis A vaccine series, a single dose of hepatitis A vaccine now can be used as an alternative to immunoglobulin. For adults younger than age 40, vaccine is preferred; for persons ≥40 years of age, immunoglobulin is preferred but vaccine is acceptable. Older adults, immunocompromised persons, and persons with chronic liver disease or other chronic medical conditions planning to depart in ≤2 weeks should receive the initial dose of vaccine and immunoglobulin can be administered simultaneously (0.02 mL/kg) at a separate anatomic injection site.50
The CDC recommends hepatitis A vaccination for all previously unvaccinated persons who anticipate close personal contact (eg, household contact or regular babysitting) with an international adoptee from a country of high or intermediate endemicity during the first 60 days after arrival of the adoptee in the United States. The first dose of the 2-dose hepatitis A vaccine series should be administered as soon as adoption is planned, ideally ≥2 weeks before the arrival of the adoptee.51
Hepatitis B
Hepatitis B Vaccination for Diabetics ≥60 Years Old
In December 2011 the ACIP recommended that all previously unvaccinated adults aged 19 to 59 years with diabetes mellitus (both type 1 and type 2) be vaccinated against hepatitis B as soon as possible after a diagnosis of diabetes is made.52 The rationale was the finding that diabetics have approximately double the risk of acquiring a new hepatitis B infection; this increased risk seems to be associated with assisted blood glucose monitoring (when equipment is shared and adequate hand hygiene procedures are not used). Although the risk also is present for diabetics ≥60 years old, hepatitis B vaccination is less cost-effective in this age range. The CDC notes that a health care provider may still wish to vaccinate a diabetic ≥60 years of age after assessing their risk, particularly regarding the patient's need for assisted blood glucose monitoring in long-term care facilities and the likelihood of experiencing chronic sequelae if infected with the hepatitis B virus.52
Persons at High Risk for Sexual Transmission of Hepatitis B
The most common source of hepatitis B infection in the United States is sexual contact. Heterosexual transmission accounts for 39% of new cases, and men who have sex with men account for 24%, whereas intravenous drug use accounts for 16% of new cases of hepatitis B infection. The CDC recommends that persons with multiple sexual partners (eg, persons with more than one sex partner during the previous 6 months), men who have sex with men, and all persons seeking evaluation of or treatment for sexually transmitted diseases should be vaccinated against hepatitis B.53 Serologic testing before vaccination only is recommended for adult populations with a prevalence of hepatitis B virus infection of >20% (eg, injection-drug users, incarcerated persons, men who have sex with men, and persons born in countries with high levels of endemic hepatitis B virus infection). Prevaccination testing can be done with a single test, hepatitis B core antibody (anti-HBc) or with a panel of tests (eg, hepatitis B surface antigen and hepatitis B surface antibody [anti-HBs]). The CDC does not recommend delaying vaccination until the test results are reviewed; the first vaccine dose typically should be administered immediately after collection of the blood sample for serologic testing.53
Keeping Current with Vaccines
To help providers keep current with changing immunization recommendations, a number of regularly updated web-based resources are available: see Table 5.
Can HPV Vaccination Prevent Cancer of the Head and Neck?
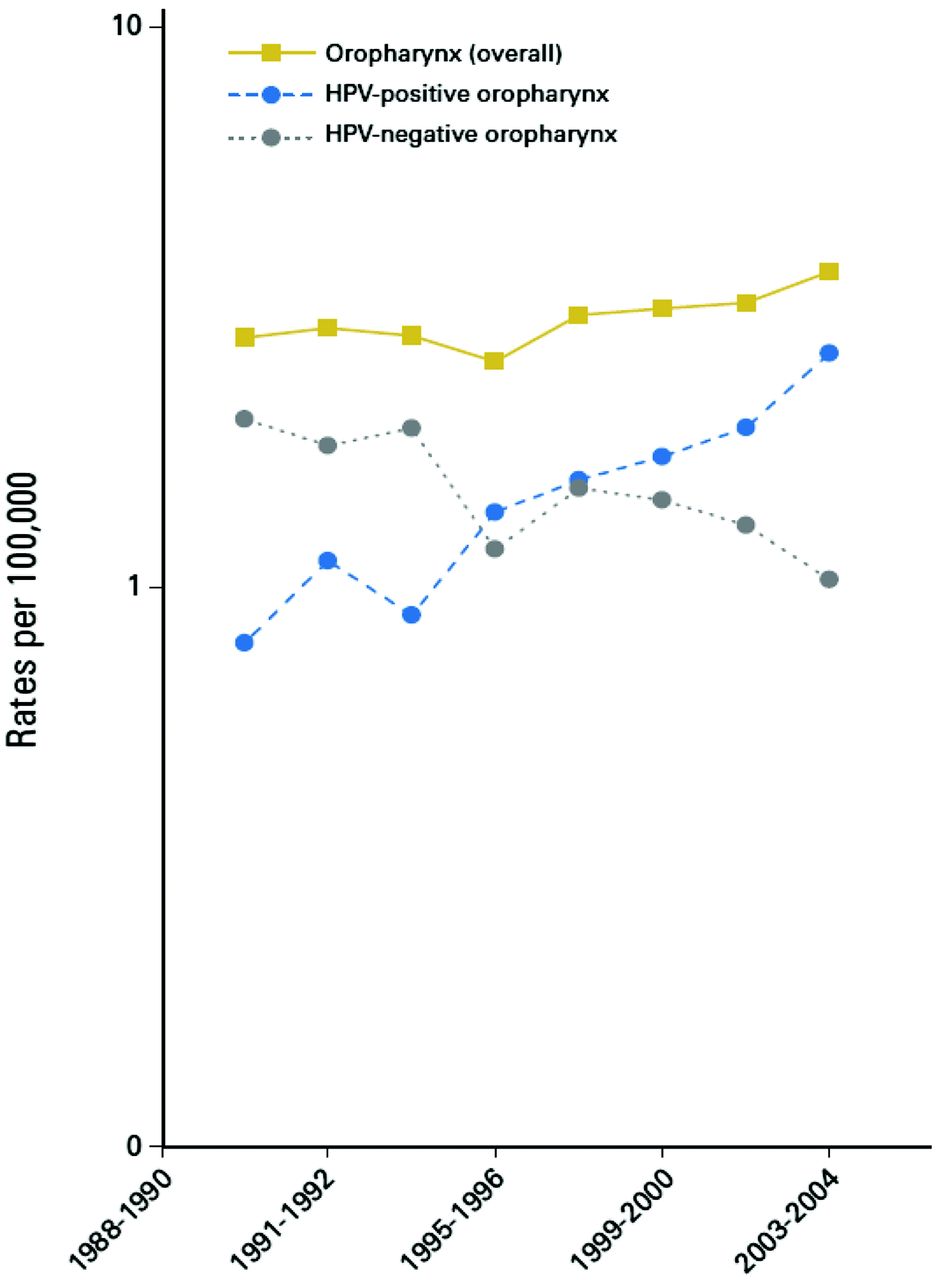
There is mounting evidence that HPV causes not only cervical and anal cancer but also is responsible for ∼25% of head and neck squamous cell carcinoma (HNSCC). The majority of these HPV-associated HNSCCs are oropharyngeal (tonsillar and base of tongue) squamous cell cancers (OSCCs), and in developed countries HPV is detected in 45% to 90% of these cases.30 There is strong evidence connecting HPV as a cause of these tumors, both on a molecular level and in epidemiologic studies showing a strong connection between OSCC, rates of oral HPV, and HPV sexual exposure. 30,33 Of HPV-positive OSCC, ∼90% are positive for high-risk HPV type 16, the type responsible for the majority of cervical cancers.34 Whereas HPV-negative OSCC has been steadily declining in the United States, paralleling the decline in smoking, HPV-positive OSCC has been steadily rising and parallels the rise in rates of oral sex and oral HPV exposure (Figure 1).35
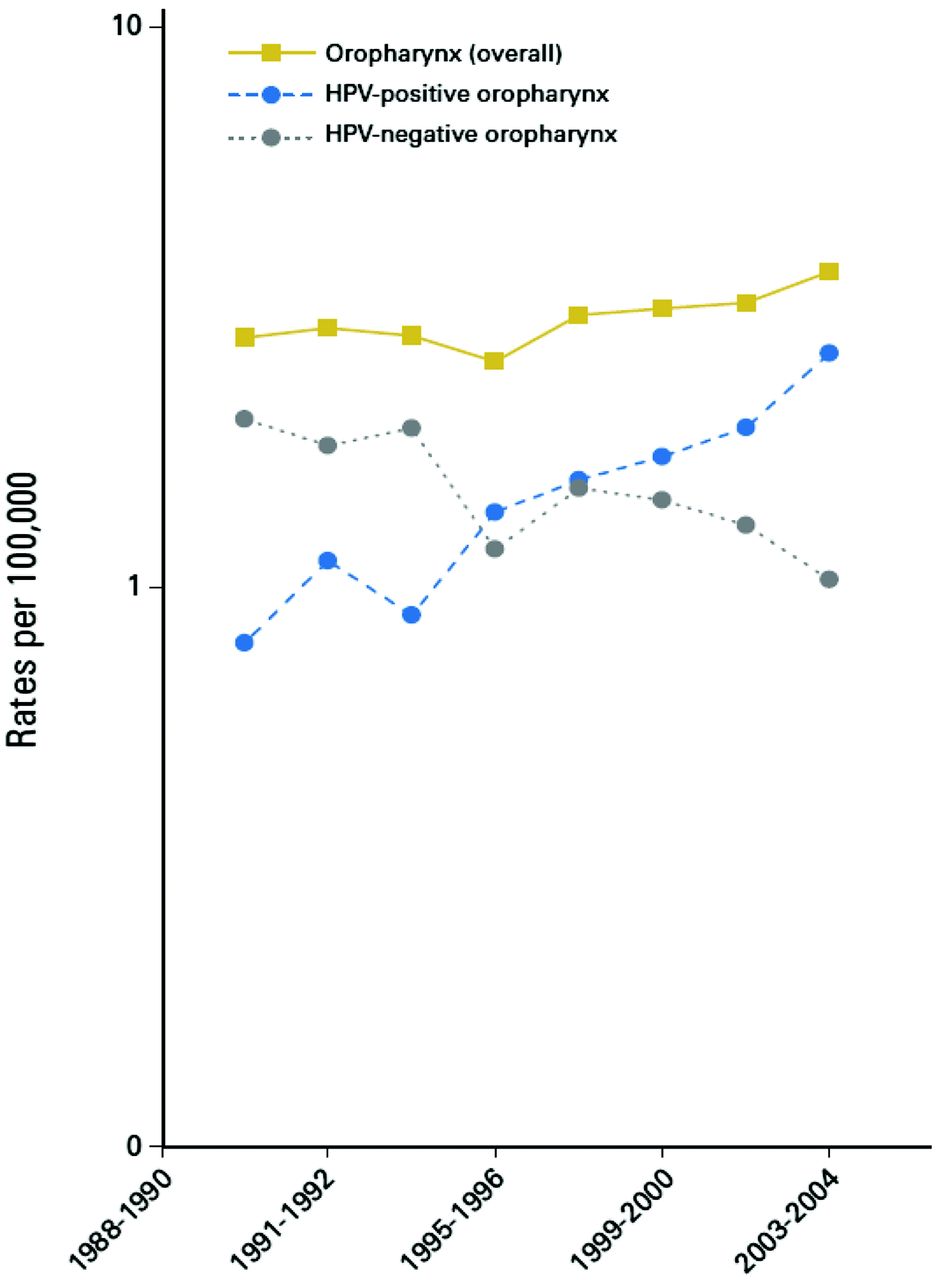
Incidence rates for overall oropharyngeal cancer, human papillomavirus (HPV)–positive oropharyngeal cancers, and HPV-negative oropharyngeal cancers during 1988 to 2004 in Hawaii, Iowa, and Los Angeles. (From Chaturvedi AK, Engels EA, Pfeiffer RM et al Human papillomavirus and rising oropharyngeal cancer incidence in the united states. J Clin Oncol 2011;29:4294-301 (Ref. 49). Reprinted with permission.)
There are significant differences between HPV-positive and HPV-negative OSCC. Patients with HPV-positive OSCC tend to be younger by about 10 years, usually are nonsmokers, have higher numbers of vaginal and oral sex partners, and have a much better response to treatment.36,37 A recent study showed that HPV-positive patients had a 69% reduction in risk of death compared with HPV-negative patients, with a mean survival of 131 versus 20 months. 35 The incidence of both HPV-associated and HPV-unassociated HNSCC is more than 2-fold higher among men than women, with a ratio from 2:1 to 5:1. The prevalence of oral HPV infection in a US study was approximately 3-fold higher in men than women (10.1% vs 3.6%) and HPV-16 prevalence was more than 5-fold higher, which could explain the higher incidence of HPV-positive OSCC among men. 38 Possible reasons for this difference include higher risk of HPV acquisition from oral sex on women versus men and higher rates of systemic antibody response to HPV genital infection in women versus men.38
By 2020, the number of HPV-positive OSCCs is projected to surpass the number of cervical cancers.35 Clinical studies to evaluate the effectiveness of HPV vaccines to prevent OSCC are in developmental stages. 39 It is highly likely that as these studies are completed and as surveillance rates monitor OSCC incidence in HPV-vaccinated populations, prevention of head and neck cancers may prove to be an additional benefit of HPV vaccination, particularly for men, who are at higher risk.
Notes
This article was externally peer reviewed.
Funding: The author is on the speakers bureau of Merck, Inc. and has been on the speakers bureau and served as a consultant for Sanofi Pasteur. He has received honoraria from both companies for these services. Both companies manufacture vaccines mentioned in this article. Author is member of the STFM Group on Immunization Education, contributes content to SHOTS program mentioned in Table 5, and receives a small stipend for this.
Conflict of interest: none declared.
- Received for publication November 15, 2010.
- Revision received February 7, 2012.
- Accepted for publication February 15, 2012.




{kind=link}