
Article Figures & Data
Figures
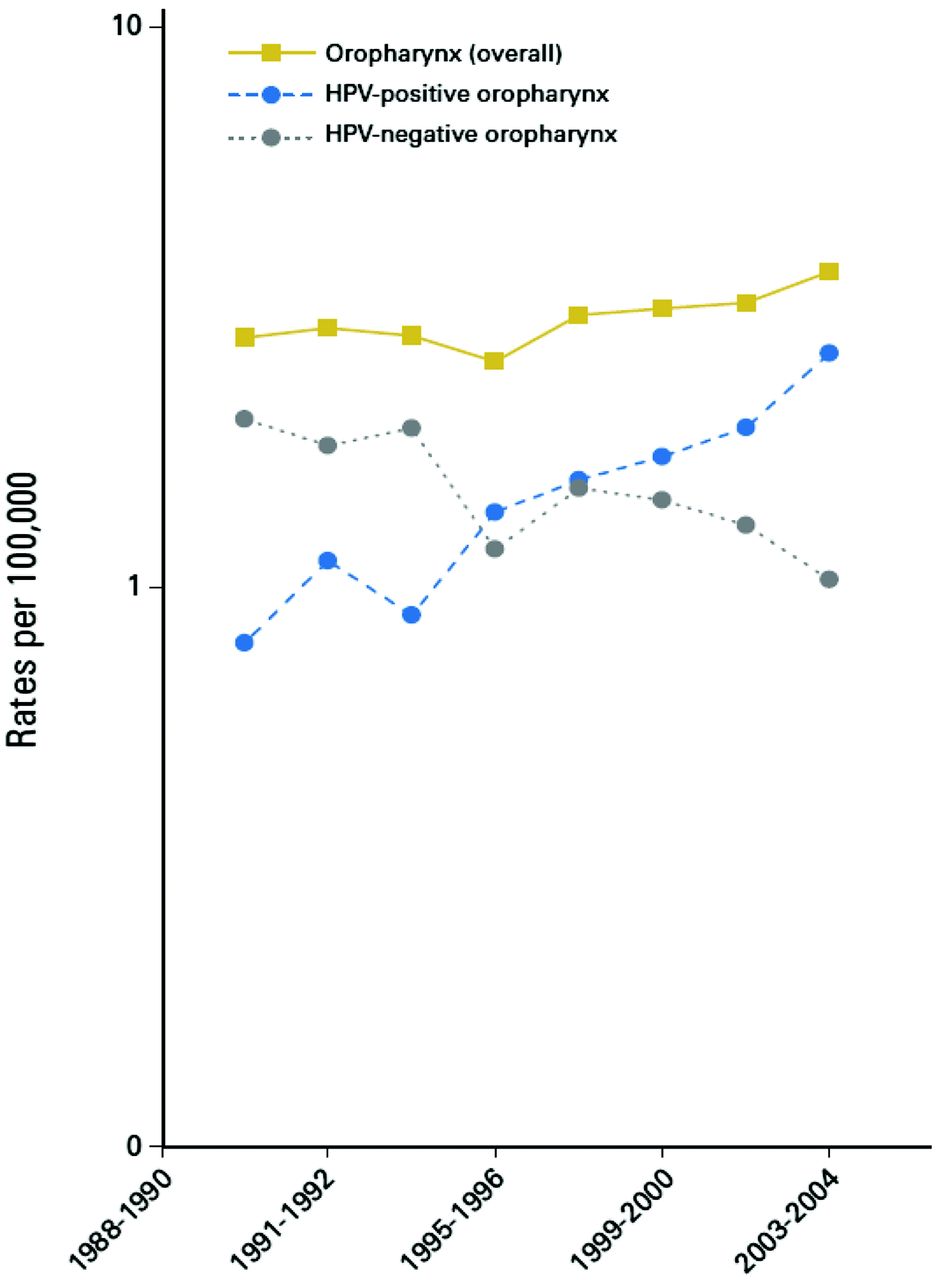
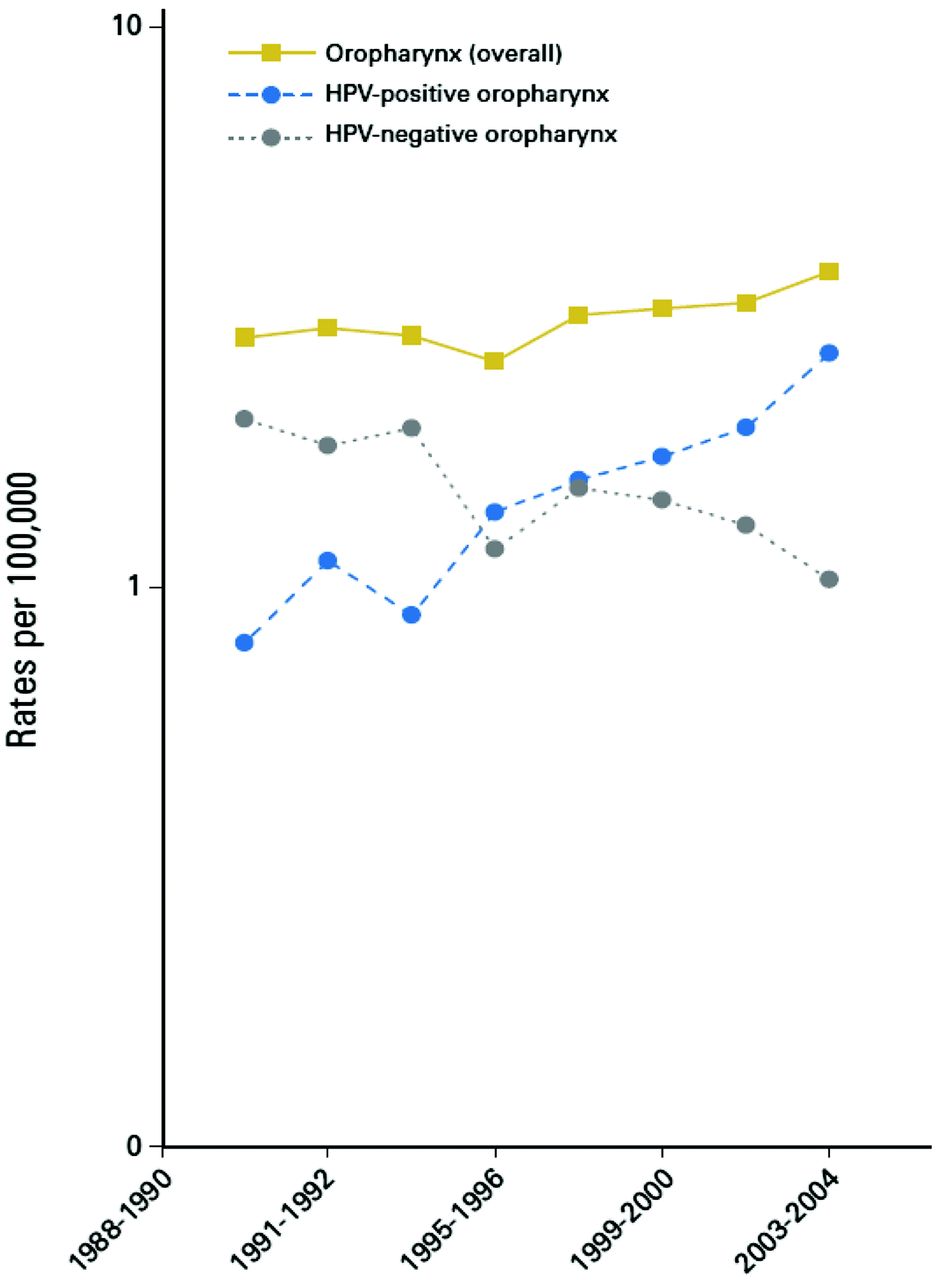
- Figure 1.
Incidence rates for overall oropharyngeal cancer, human papillomavirus (HPV)–positive oropharyngeal cancers, and HPV-negative oropharyngeal cancers during 1988 to 2004 in Hawaii, Iowa, and Los Angeles. (From Chaturvedi AK, Engels EA, Pfeiffer RM et al Human papillomavirus and rising oropharyngeal cancer incidence in the united states. J Clin Oncol 2011;29:4294-301 (Ref. 49). Reprinted with permission.)
Tables
Who needs to be vaccinated with PPV23? Vaccinate all previously unvaccinated adults aged 65 years and older.
Vaccinate all adults who smoke cigarettes.
Vaccinate persons aged 2 to 64 years who:
have chronic cardiovascular disease (eg, congestive heart failure, cardiomyopathy); chronic pulmonary disease (eg, chronic obstructive pulmonary disease, emphysema, adults with asthma); or diabetes mellitus or those who are cochlear implant patients.
have chronic liver disease (including cirrhosis), are alcoholic, or have a cerebrospinal fluid leak.
live in special environments or social settings (eg, adults aged 50 to 64 years who are Alaska Natives or certain American Indian populations if recommended by local health authorities).
Vaccinate persons aged 2 to 64 years with functional or anatomic asplenia (including persons with sickle cell disease or splenectomy patients).
Vaccinate immunocompromised persons aged 2 years and older, including those with HIV infection,* leukemia, lymphoma, Hodgkin disease, multiple myeloma, generalized malignancy, chronic renal failure (including dialysis patients), or nephrotic syndrome; those receiving immunosuppressive therapy (including long-term systemic corticosteroids); and those who have received an organ or bone marrow transplant.†
Who needs a second dose of PPV23? A one-time revaccination is indicated for: All adults aged 65 years and older who were previously vaccinated with PPSV before age 65 if ≥5 years have elapsed since the previous dose.
All children and adults who are at the highest risk of serious pneumococcal disease or are likely to have a rapid decline in pneumococcal antibody levels (categories 4 and 5 above) if ≥5 years have elapsed since the previous dose.
↵* Persons with asymptomatic or symptomatic HIV infection should be vaccinated as soon as possible after their diagnosis is confirmed (per Prevention of pneumococcal disease: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 1997;46(RR-8):1–24).
↵† When cancer chemotherapy or other immunosuppressive therapy is being considered (eg, for patients with Hodgkin disease or those who undergo organ or bone marrow transplantation), PPV23 should be given 2 weeks before or 3 months after immunosuppressive or radiation therapy. Vaccination during chemotherapy or radiation therapy should be avoided (per Prevention of pneumococcal disease: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 1997;46(RR-8):1–24).
Adapted with permission from Pneumococcal polysaccharide vaccine (PPSV) CDC answers your questions. From the Immunization Action Coalition, St. Paul, MN. Available online at: www.immunize.org/catg.d/p2015.pdf.
Practice Recommendations Level of Evidence Reference Give pneumococcal polysaccharide vaccine (PSV23, Pneumovax) for prevention of pneumococcal disease to following persons: Immunocompetent persons and persons aged ≥65 years of age. A 54 Persons aged 2–64 years with chronic cardiovascular disease, chronic pulmonary disease, or diabetes mellitus. A 54 Persons aged 2–64 years with alcoholism, chronic liver disease, or cerebrospinal fluid leaks. B 54 Give herpes zoster vaccine (Zostavax) for the prevention of herpes zoster and its complications in persons ≥60 years without contraindications. A 55 Vaccine Name and Route For Whom Vaccination Is Recommended Schedule for Vaccine Administration* Contraindications and Precautions† Influenza
TIV (give IM)
LAIV (give intranasally)• Vaccination is recommended for all adults. (This includes healthy adults aged 19–49 years without risk factors.)
• LAIV is only approved for healthy nonpregnant people aged 2–49 years.
• Adults aged 18-64 years may be given any intramuscular TIV product or, alternatively, the intradermal TIV product (Fluzone Intradermal).
• Adults ages 65 years and older may be given standard-dose TIV or, alternatively, the high-dose TIV (Fluzone High-Dose).
Note: LAIV may not be given to some adults; see contraindications and precautions listed in far right column.• Give 1 dose every year in the fall or winter. Begin vaccination services as soon as vaccine is available and continue until the supply is depleted.
• Continue to give vaccine to unvaccinated adults throughout the influenza season (including when influenza activity is present in the community) and at other times when the risk of influenza exists.
• If 2 or more of the following live virus vaccines are to be given—LAIV, MMR, varicella, or yellow fever—they should be given on the same day; otherwise space them apart by at least 28 days.Contraindications:
• Previous anaphylactic reaction to this vaccine or to any of its components. Egg allergy is no longer a contraindication for TIV.
• For LAIV only: pregnancy; chronic pulmonary (including asthma), cardiovascular (except hypertension), renal, hepatic, neurological/neuromuscular, hematologic, or metabolic (including diabetes) disorders; immunosuppression (including that caused by meds or HIV)
Precautions:
• Moderate or severe acute illness.
• History of Guillain-Barré syndrome within 6 weeks after previous influenza vaccination.
• For LAIV only: close contact with an immunosuppressed person when the person requires protective isolation or receipt of specific antivirals (ie., zanamivir or oseltamivir) 48 hours before vaccination. Avoid use of these antiviral drugs for 14 days after vaccination.Human papillomavirus
HPV2 (Cervarix; give IM)
HPV4 (Gardasil; give IM)HPV2 or HPV4:
• All previously unvaccinated women through age 26 years
HPV4 only:
• All previously unvaccinated men through the age of 21 years and previously unvaccinated men 22-26 years who are immunocompromised, who test positive for HIV infection, or who have sex with men
Note: any man may receive the HPV4 through age 26 if desired• Give 3 doses on a 0, 2, and 6 month schedule.
• There must be at least 4 weeks between doses 1 and 2 and at least 12 weeks between doses 2 and 3. Overall, there must be at least 24 weeks between doses 1 and 3. If possible, use the same vaccine product for all 3 doses.Contraindication:
• Previous anaphylactic reaction to this vaccine or to any of its components.
Precautions:
• Moderate or severe acute illness.
• Data on vaccination in pregnancy are limited. Vaccination should be delayed until after completion of the pregnancy.Pneumococcal polysaccharide (PSV23; give IM or SC) See Table 1 See Table 1 Contraindication: Previous anaphylactic reaction to this vaccine or to any of its components.
Precaution: Moderate or severe acute illness.Td, Tdap (give IM) • All adults who lack written documentation of a primary series of at least 3 doses of tetanus and diphtheria toxoid vaccine.
• A booster dose of tetanus- and diphtheria toxoid–containing vaccine may be needed for wound management as early as 5 years after last dose; consult ACIP recommendations‡
• During pregnancy, when indicated, give Td or Tdap in second or third trimester. If not administered during pregnancy, give Tdap in immediate postpartum period.
For Tdap only:
• Adults <65 years who have not already received Tdap.
• Adults of any age, including adults ≥65 years in contact with infants <12 months (eg, parents, grandparents, childcare providers) who have not received a dose of Tdap should be prioritized for vaccination.
• Health care personnel of all ages.
• Adults aged ≥65 years without a risk indicator (eg, not in contact with an infant) may also be vaccinated.• For people who are unvaccinated or behind, complete the primary Td series (spaced at 0, 1- to 2-month, 6- to 12-month intervals); substitute a one-time dose of Tdap for one of the doses in the series, preferably the first.
• Give Td booster every 10 years after the primary series has been completed.
• Tdap should be given regardless of interval since previous Td.Contraindications:
• Previous anaphylactic reaction to this vaccine or to any of its components.
• For Tdap only, history of encephalopathy not attributable to an identifiable cause, within 7 days after DTP/DTaP.
Precautions:
• Moderate or severe acute illness.
• Guillain-Barré syndrome within 6 weeks after previous dose of tetanus toxoid–containing vaccine.
• For Tdap only, progressive or unstable neurologic disorder, uncontrolled seizures, or progressive neuropathy until a treatment regimen has been established and the condition has stabilized.
• History of arthus reaction after a prior dose of tetanus- or diphtheria toxoid–containing vaccine; defer vaccination until at least 10 years have elapsed since the last tetanus toxoid–containing vaccine.Zoster (shingles; give SC) • People aged ≥60 years
Note: Zoster is FDA-approved for persons 50 years and older, but is not CDC recommended for this age group and therefore may not be covered by some insurers for persons aged 50–59 years• Give one-time dose if unvaccinated, regardless of previous history of herpes zoster (shingles) or chickenpox.
• If 2 or more of the following live virus vaccines are to be given—MMR, zoster, or yellow fever—they should be given on the same day. If they are not, space them by at least 28 days.Contraindications:
• Previous anaphylactic reaction to this vaccine or to any of its components
• Primary cellular or acquired immunodeficiency
• Pregnancy
Precautions:
• Moderate or severe acute illness.
• Receipt of specific antivirals (ie, acyclovir, famciclovir, or valacyclovir) 24 hours before vaccination, if possible; delay resumption of these antiviral drugs for 14 days after vaccination.Meningococcal
Meningococcal conjugate vaccines (MCV4; give IM)
Menactra, Menveo
Meningococcal polysaccharide vaccine (MPSV4; give SC)For people through age 18 years, consult “Summary of Recommendations for Child/Teen Immunization” at www.immunize.org/catg.d/p2010.pdf.
• People with anatomic or functional asplenia or persistent complement component deficiency.
• People who travel to or reside in countries in which meningococcal disease is hyperendemic or epidemic (eg, the “meningitis belt” of Sub-Saharan Africa).
• Microbiologists routinely exposed to isolates of Neisseria meningitidis
• First-year college students through age 21 years who live in residence halls (see fifth bullet in the column to the right for details).• Give 2 initial doses of MCV4 2 months apart to adults ≤55 years with risk factors listed in first bullet in column to left or to adults with HIV in this age group.
• Give one initial dose to all other adults with risk factors (see second through fourth bullets in column to left).
• Give booster doses every 5 years to adults with continuing risk (see the first through third bullets in column to left).
• MCV4 is preferred over MPSV4 for people ≤55 years old unless contraindicated; use MPSV4 only if age ≥56 years
• For first-year college students aged 19-21 years living in residence halls, give one dose if unvaccinated plus booster dose if most recent dose was given when <16 years.Contraindication:
• Previous anaphylactic reaction to this vaccine or to any of its components
Precaution:
• Moderate or severe acute illnessHepatitis A Refer to the Summary of Recommendations for Adult Immunization table at the Immunization Action Coalition (IAC) website at www.immunize.org/adultrules Hepatitis B MMR Varicella Polio ↵* Any vaccine can be given with another.
↵† Mild illness is not a contraindication.
Adapted with permission from Summary of Recommendations for Adult Immunization, Immunization Action Coalition, St. Paul, MN (2011). The original table is adapted from the recommendations of the Advisory Committee on Immunization Practices (ACIP) and is updated regularly at www.immunize.org/adultrules.
CDC, Centers for Disease Control and Prevention; FDA, US Food and Drug Administration; IM, intramuscularly; LAIV, live attenuated influenza vaccine; MMR, measles–mumps–rubella; SC, subcutaneously; Td, tetanus–diptheria; Tdap, tetanus, diphtheria, acellular pertussis; TIV, trivalent inactivated influenza vaccine.
- Table 4. Summary of Main Changes* from 1997 Advisory Committee on Immunization Practices/Hospital† Infection Control Practices Advisory Committee Recommendations for Immunization of Health Care Personnel
Hepatitis B HCP and trainees in certain populations at high risk for chronic hepatitis B (eg, those born in countries with high and intermediate endemicity) should be tested for HBsAg and anti-HBc/anti-HBs to determine infection status. Influenza Emphasize that all HCP, not just those with direct patient care duties, should receive an annual influenza vaccination. Comprehensive programs to increase vaccine coverage among HCP are needed; influenza vaccination rates among HCP within facilities should be measured and reported regularly. MMR History of disease is no longer considered adequate presumptive evidence of measles or mumps immunity for HCP; laboratory confirmation of disease was added as acceptable presumptive evidence of immunity. History of disease has never been considered adequate evidence of immunity for rubella. The footnotes have been changed regarding the recommendations for personnel born before 1957 in routine and outbreak contexts. Specifically, guidance is provided for 2 doses of MMR for measles and mumps protection and 1 dose of MMR for rubella protection. Pertussis HCP, regardless of age, should receive a single dose of Tdap as soon as feasible if they have not previously received Tdap. The minimal interval was removed, and Tdap now can be administered regardless of interval since the last tetanus- or diphtheria-containing vaccine. Hospitals and ambulatory care facilities should provide Tdap for HCP and use approaches that maximize vaccination rates. Varicella Criteria for evidence of immunity to varicella were established. For HCP they include: Written documentation with 2 doses of vaccine; Laboratory evidence of immunity or laboratory confirmation of disease; Diagnosis of history of varicella disease by health care provider or diagnosis of history of herpes zoster by health care provider. Meningococcal HCP with anatomic or functional asplenia or persistent complement component deficiencies should now receive a 2-dose series of meningococcal conjugate vaccine. HCP with HIV infection who are vaccinated should also receive a 2-dose series. Those HCP who remain in groups at high risk are recommended to be revaccinated every 5 years. ↵* Updated recommendations made since publication of the 1997 summary of recommendations (CDC Immunization of health-care workers: recommendations of the Advisory Committee on Immunization Practices [ACIP] and the Hospital Infection Control Practices Advisory Committee [HICPAC]. MMWR 1997;46[No. RR-18]).
↵† Is now “Healthcare.”
CDC, Centers for Disease Control and Prevention; HBsAg, hepatitis B surface antigen; anti-HBc, hepatitis B core antibody; anti-HBs, hepatitis B surface antibody; HCP, health care personnel; MMR, measles, mumps, rubella; Tdap, tetanus toxoid, reduced diptheria toxoid, and acellular pertussis vaccine, adsorbed.
Reprinted with permission from: Centers for Disease Control and Prevention. Immunization of health-care personnel: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2011;60(RR-7):1-45.
Family physicians who wish to stay current with the most recent updates in vaccine recommendations can get up-to-date information at these sites: CDC The Healthcare Professional website of the National Immunization Program of the CDC has extensive current information on immunizations and has an Adult Immunization Scheduler program available for free download. www.cdc.gov/vaccines/hcp.htm Immunization Action Coalition The Immunization Action Coalition is a nonprofit organization based in St. Paul, Minnesota. Their website contains extensive, easy-to-access informational materials for providers and patients, and features IAC Express, a free weekly email immunization newsletter for health professionals. www.immunize.org/ SHOTS by STFM The Group on Immunization Education of the Society of Teachers of Family Medicine (STFM) created the SHOTS program, developed with support from the CDC.
SHOTS by STFM is a free point-of-care immunization information system that can be accessed online or as a stand-alone program compatible with iPhone, Android, and Blackberry. SHOTS contains the complete immunization schedules for children, adults, and persons with special medical conditions. In addition, information can be quickly viewed for each individual vaccine regarding immunization basics, high-risk indications, adverse reactions, contraindications, administration, and catch-up schedules.www.immunizationed.org/ShotsOnline.aspx CDC, Centers for Disease Control and Prevention.




{kind=link}