
Abstract
Objective: To evaluate the efficacy of videotaped instruction of a behavioral intervention to reduce crying among newborns.
Methods: Mothers of healthy, full-term newborns were recruited from the postpartum unit of a large community hospital for a prospective, randomized, controlled trial of an intervention to reduce infant crying. Mothers participating in the intervention viewed a videotape with instructions involving swaddling, side positioning, white noise, jiggling, and sucking. Mothers in the control group viewed a videotape with instructions for normal newborn care. Intervention was assessed by mean hours per day of infant total crying (fussing, crying, and unsoothable crying) and sleeping as recorded in a diary 3 days a week during the 1st, 4th, 6th, 8th, and 12th weeks of age; the Parenting Stress Index was also used during the 6th and 12th weeks.
Results: Fifty-one mother-infant pairs were recruited; 35 completed the study (18 intervention and 17 controls). Sixteen were lost to follow-up. There were no statistically significant differences between the groups in the hours of mean daily total crying or sleeping during the 1st, 4th, 6th, 8th, or 12th weeks of age. For example, during the 6th week of age mean daily total crying was 1.9 hours for infants in the control group versus 2.2 hours for infants in the intervention group (P = .4); sleep was 14.5 hours for infants in the control group versus 14.4 hours for infants in the intervention group (P = .8). During the 12th week mean daily total crying was 1.2 hours for infants in the control group versus 1.8 hours for infants in the intervention group (P = .8) and sleep was 14.1 hours for infants in the control group versus 14.0 hours for infants in the intervention group (P = 1.0). There was no difference between the groups in the Parenting Stress Index during the 6th week of age.
Conclusion: The behavioral intervention, when provided via videotape, does not seem to be efficacious in decreasing total crying among normal infants.
The persistent crying of infants during the first 3 months of life is one of the most frequent complaints made by caregivers and one of the most common reasons for both breastfeeding cessation and visits to medical care providers.1–3 Persistent crying can be associated with maternal physical and psychological symptoms or marital tension and affect the maternal-infant bonding process.4,5 Infant crying and the caregiver's inability to console the infant has been identified as a common inciting event for shaken baby syndrome.6–9 Infants who cry persistently may sleep less than other infants,10,11 which contributes to these problems. Although persistent crying is a self-limiting condition,12,13 caregiver fatigue and frustration, impaired bonding, and child abuse are compelling reasons to develop and evaluate interventions.
Recent reviews of the literature describe several treatments that have been shown to be effective in randomized controlled trials.14,15 Most reviews recommend a trial of a hypoallergenic diet, especially for infants who had other associated symptoms.14–16 Lactobacillus reuteri, fennel seed oil, herbal tea, and an herbal preparation have all been shown to decrease daily crying in randomized controlled trials.17–20 None of these trials reported adverse events, but the short-term and long-term safety is not known. Behavioral interventions, such as decreasing stimulation and providing parent support, have been taught to parents with mixed results on the amount of crying,21–25 although an educational intervention has shown an increased knowledge about infant crying.26 There seems to be no consensus on treatment and further research is generally recommended.14,15
One method for calming infants, referred to as The Happiest Baby (THB) method, is based on the hypothesis that actions mimicking conditions in the womb will trigger a calming reflex.27 This method uses swaddling as a basis for the intervention, and proceeds to incorporate side/stomach positioning, shushing (producing a loud and constant sound near the infant's ear), swinging/jiggling, and sucking as needed. This method has some similarities to behavior exhibited by the !Kung San, whose infants have been found to have a shorter duration of crying than those in western societies.28
We hypothesized that infants of mothers who viewed a videotape teaching the THB method would fuss and cry less and sleep more during the 4th to 8th weeks of age than those whose mothers viewed a control tape. We also hypothesized that mothers viewing the intervention video would experience less stress, as indicated by a lower Parenting Stress Index (PSI).
Methods
Study Population
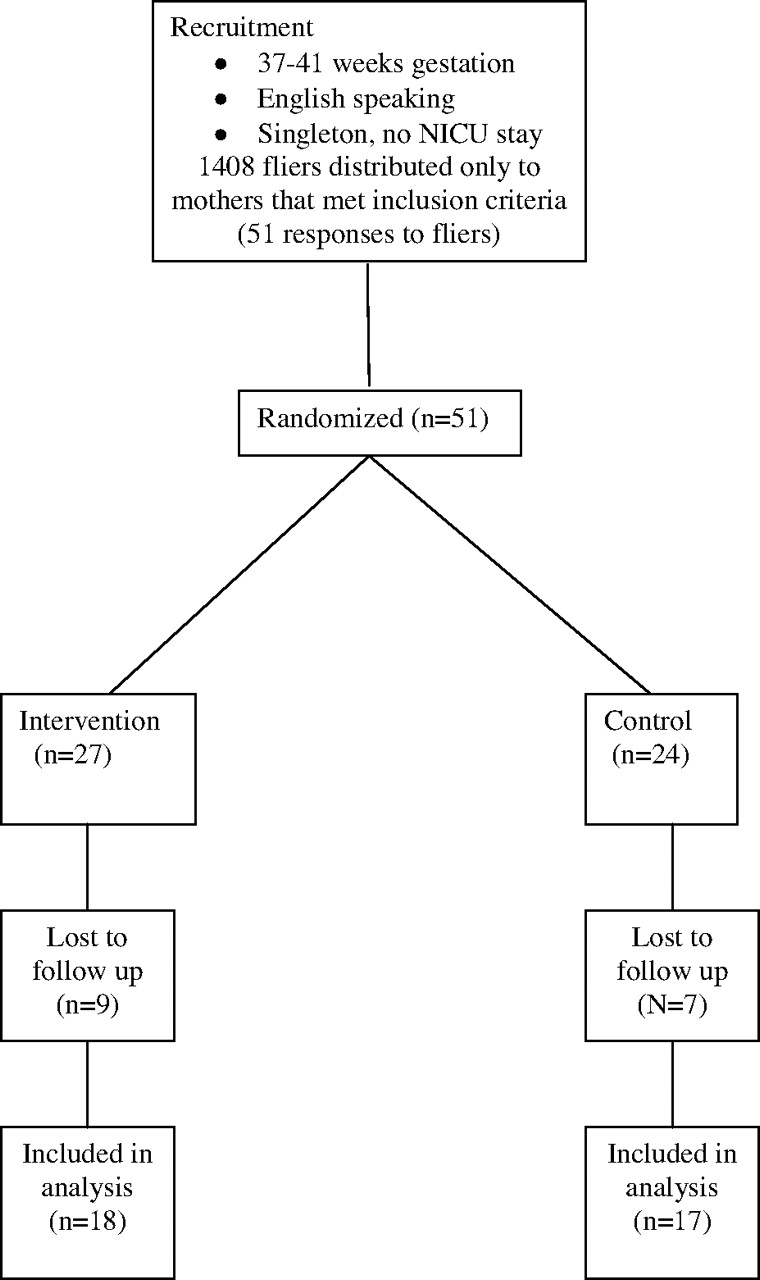
Mothers of healthy, singleton, newborn infants with a gestational age of 37 to 41 weeks admitted to the normal newborn nursery of a large community hospital and who had the resources to view a VHS tape at home were given a flier inviting them to participate in a study on parenting advice by contacting a research assistant by phone before being discharged. Mothers who did not speak English or were unable to fill out a diary (described below) themselves were excluded. Mothers were recruited between August 2005 and February 2006.
Intervention
The intervention was a 30-minute videotape demonstrating the THB method for calming newborn infants. Caregivers were reminded to first try feeding, holding, and changing their newborn when he/she cried. If none of these was effective, they were encouraged to try the following technique, the basis of which is swaddling. How to swaddle an infant is illustrated in the video, with specific advice to allow the hips to flex and to avoid overheating. If the infant is not consoled with swaddling alone, a series of additional steps is recommended, each added to the other, until the infant is calm. The second step is to place the infant on his/her side or stomach. Caution is given not to do this when babies are put to sleep. The third step is to expose the infant to a loud, harsh, white noise, such as “shushing” in the ear. The fourth step is swinging (rhythmically, jiggling) in rapid, tiny movements. Here caution is given never to shake an infant. The final step is to give the infant a pacifier or otherwise allow the infant to suck.
Control
The control videotape was a 30-minute videotape entitled “Begin with Love” by Civitas (Chicago, IL). It is offered on the Newborn Channel and is available to mothers in many postpartum inpatient settings. This videotape provides 5 standard recommendations for taking care of normal newborns:
Take care of yourself.
Provide a warm and loving environment.
Talk, sing, and read to your baby.
Create a predictable world with routines.
Respond to your baby's needs; a newborn infant cannot be spoiled.
This videotape provides standard advice for parents of infants who are not consoled with feeding, changing, or holding; namely, never shake your infant, get help to handle the stress, and take heart that it will eventually get better.
Clinical Protocol
Informed consent was obtained by the research assistant. Mothers completed a survey at baseline. The survey included the open-ended question, What do you do to calm your baby when he/she cries? in an effort to determine whether mothers were already using the THB method. All mothers received training on completing a Baby's Day Diary, which is described below.29 Each mother-infant pair was randomized by a randomization table to either the intervention or control group and given a unique code number. The research assistant was initially blinded to participant assignment; however, to assess study compliance, follow-up data were collected with knowledge of group assignment. Mothers were given a videotape in an unmarked jacket to view before discharge and to take home to view as often as she found helpful. All mothers received a lightweight blanket large enough to swaddle a newborn infant, along with the following recommendations:
It is safest to put your baby to sleep on his/her back.
Never put your baby to sleep with loose blankets.
Do not allow your baby to overheat. Check the baby's neck to see if he/she is too hot.
When your baby cries, see if he/she needs to be fed, changed, or held.
Never shake your baby.
All mothers were contacted by phone during their first week home to assess their understanding of and compliance with the Baby's Day Diary.29 Mothers in the intervention group were also asked open-ended questions to assess their understanding of the intervention both during the first week at home and during the sixth week. Intervention mothers were considered compliant if they answered “yes” to the question, Have you had an opportunity to try the technique taught in the videotape? and also “yes” or “sometimes” to the question, Do you swaddle your infant when you are trying to calm him/her? Compliance was coded as a dichotomous variable: either the parents endorsed some use of the method or none. Control mothers were considered compliant if they provided diaries for week 6.
During the 6th and 12th weeks, all mothers were asked the open-ended questions, What do you do to calm your baby when he/she cries? and Have you ever had to put your baby in a safe place and leave for a few minutes because you could not calm him/her? Mothers were given stamped, self-addressed envelopes and were contacted by phone if the diaries were more than 6 days past due. Mothers received incentives in the form of gift cards for completion of the diaries and surveys ($25 per set of diaries; $75 maximum).
Measures
Mothers completed an Edinburgh Postnatal Depression Scale30 at baseline and during the 6th and 12th weeks. This was done to make sure there was no difference between the groups should maternal depression affect the way mothers completed the diaries or performed the intervention.
Primary and Secondary Outcome Measures
The primary outcome measure was the mean hours per day of total infant crying (fussing, crying, and unsoothable crying) as recorded in the Baby's Day Diary29 by their mothers 3 days per week during the 1st, 4th, 6th, 8th, and 12th weeks of age. The diary was a printed sheet with the 24-hour day divided into 4 timelines of 6 hours each. The timelines were further divided into 5-minute intervals. Mothers recorded their baby's activity by filling in the behavior, represented by marks for each activity according to a code included on the sheet: sleep, awake and content, awake and fussy, awake and crying, unsoothable crying, feeding, or cannot remember. The frequency and duration of crying recorded on the Baby's Day Diary29 has been found to have a moderately strong correlation with simultaneous audio-taped recordings29,31 and is commonly used in studies of infant crying. Secondary outcome measures included the mean hours per day of sleep and the mother's level of stress as measured using the PSI, which was administered to the mother during the infants’ 6th and 12th weeks of age. The PSI was developed to assess stress in the parent-child relationship in parents of children 1 month to 12 years of age.32
Statistical Methods
Statistical analyses were done using the SAS software (SAS, Inc., Cary, NC). The primary outcomes were analyzed as continuous variable with either a Wilcoxon 2-sample test or a student t test. Shapiro Wilk tests for normality were used to make decisions between parametric and nonparametric statistical tests. Fisher exact tests were used when expected cell counts were <5. P < .01 was interpreted as indicating a statistically significant difference caused by multiple testing. P < .05 was considered suggestive of a statistically significant difference.
Diaries
Mean daily total crying time included time spent crying, fussing, and crying that was unable to be soothed. For each day, the sum of these 3 behaviors was calculated; the mean of the 3 daily sums at each specific age was then calculated, yielding the mean daily total crying time. Mean daily total sleep time was, similarly, the mean of 3 daily sleep times reported at each age. Diary data that had more than 3 hours not recorded or recorded as “can't remember” were excluded from analysis. If fewer than 3 diaries were completed for a given time period (ie, one or 2 of the days was missing or had more than 3 hours unrecorded), then the means of only the completed diaries were used.
The PSI was scored according to the manual.32 Total stress scores can range from 131 to 320 (less stress to more), with a score of 222 being the 50th percentile.
Institutional review board approval was obtained from Nationwide Children's Hospital and Riverside Methodist Hospital (both in Columbus, OH). During the 6th and 12th weeks, mothers were asked the open-ended question, Have you taken the baby to the doctor for any visits other than regularly scheduled check-ups since he/she was born? All Edinburgh Postnatal Depression Scales were scored as they were received and the mother was notified to contact her physician for evaluation if her screen was positive for depression (a score of ≥12).30
Results
Participant Drop Out
Of the 51 participants enrolled, 16 (31%) did not complete the study and were excluded from statistical analyses (Figure 1). These 16 participants (9 from the intervention group and 7 from the control group) did not complete any of the diaries or data collection instruments beyond baseline. Because crying and sleeping scores were not available, an intention-to-treat analysis including these participants was not possible. Demographic characteristics of these 16 participants were compared with the 35 who completed the study. Those who did not complete the study had significantly lower levels of education compared with those who did complete it, but were not different on any of the other demographic variables.

Flow of participant progress. NICU, neonatal intensive-care unit.
Group Differences at Randomization
Demographic and baseline characteristics of the intervention and control participants were compared (Table 1). There were no statistically significant differences between groups, indicating successful randomization. Edinburgh Postnatal Depression Scale scores were not significantly different between groups at baseline or at weeks 6 or 12.
Comparison of Groups on Demographic and Baseline Characteristics
Mean Daily Total Crying
There were no statistically significant differences between control and intervention groups with respect to mean daily total crying (fussing, crying, and unsoothable crying) at any of the 5 age points (Table 2). Daily total crying time was recalculated to include only crying and unsoothable crying (“awake and fussy” was excluded). Again, there were no statistically significant differences between the control and intervention groups. During the eighth week, mean daily total crying time for infants in the intervention group was greater than the control group (mean difference, 0.7 hours), but the difference did not reach statistical significance (P = .04) and the direction of the effect was opposite to the hypothesized direction.
Mean Daily Total Crying* and Sleeping (Hours/Day)
Mean Daily Sleep
There were no statistically significant differences between the control and intervention groups with respect to mean daily sleep at any of the 5 age points (Table 2). Analysis was repeated using the definitions of compliance noted above. Of the 18 intervention participants, 15 were compliant with swaddling during the sixth week (2 did not answer the question and one said “no”). Of the 17 controls, 16 were compliant. There were no differences between the groups in average daily total crying or sleeping.
Parenting Stress Index
The total stress scores on the PSI are presented in Table 3. During the 12th week, the intervention group had higher scores compared with controls (P = .01).
Parenting Stress Index
Questions to Mothers
In response to the question, What do you do to calm your baby when he/she cries?, there were no answers specifically referring to the THB method or the videotape. However, mothers in each group reported behaviors such as “swaddle,” “bounce,” “swing,” and “pacifier,” both at baseline and on the surveys during the 6th and 12th weeks. There were no positive responses to the question, Have you ever had to put your baby in a safe place and leave for a few minutes because you could not calm him/her? There were no responses of “colic” or “crying” to the question, Have you taken the baby to the doctor for any visits other than regularly scheduled check-ups since he/she was born?
Discussion
When mothers learned the THB method from watching a videotape alone, it failed to have a positive impact on infant mean daily total crying or sleep. There were modest, sporadic differences in mean daily total crying and parenting stress that favored the control group. None of these differences reached the predetermined level of statistical significance, except PSI scores from week 12; this may be because of chance or multiple testing.
There are many reasons this intervention may have failed to reduce infant crying. We did not provide personalized training. The method is now being taught to certified trainers, who then work with parents one on one. We were not able to have the mothers show us how they used the method. Mothers were encouraged by the research assistant to ask questions about using the method, both in the hospital and during follow-up, although few did. We also asked mothers questions addressing how they used the method. We did this within the first week at home and during the sixth week. Swaddling is the foundation for THB technique and this prompted us to use an affirmation of swaddling as an indicator of compliance. However, conversations with mothers in the intervention group indicated that many were not using the method as instructed in the videotape.
It is difficult to change behaviors, and studies of behavioral interventions in other areas of health behavior have shown that minimal interventions often demonstrate little or no impact on behaviors.33 Maternal response to newborn crying is both instinctual and bound in complicated social norms and expectations that vary from “don't hold him so much or you will spoil him” to constant holding, feeding, and skin contact. In addition, many of the action steps promoted in THB method may be common to mothers who never received such an intervention. The unique contribution of THB method is the order of the steps and the specifics of the steps (ie, how to swaddle).
It may be that women in the intervention group did not interpret their baby's crying as necessitating the use of THB method. When asked, none of the mothers in the study responded that they took their baby to the doctor for “colic” or “crying” at weeks 6 and 12, despite the fact that many recorded that their infant cried in excess of 180 minutes per day, possibly indicating colic.34 Studies vary, but the incidence of infants with colic is between 3% and 19%.16,35 It has been noted that similar crying may not be interpreted in the same way by all mothers.36 This may also explain why several mothers were enthusiastic about the technique during conversations with the research assistant despite the fact that they recorded their infants as having prolonged periods of crying.
This trial may have been too small to demonstrate a difference. For a minimally intense intervention to reduce crying time by 40% among average babies (α = 0.05 and a power of 0.8), a sample of 42 mothers with data at follow-up would be required. It is possible that this intervention may have modest effects on crying (10% to 20% decrease), which this study was not sufficiently powered to detect. However, a more modest reduction in crying may also not be clinically important unless it is accompanied by improvements in parenting stress, depression symptoms, and feelings of control.
Future studies of this type of crying reduction program might be more likely to yield positive results if the intervention includes one-on-one coaching, verification that THB techniques were being used as they were taught, and periodic reinforcement of the techniques. However, when provided as videotape training to otherwise normal mothers and infants, apparently there is little difference in infant crying or sleeping.
Acknowledgments
Support from the University of Toledo College of Medicine, Nationwide Children's Hospital, and Riverside Methodist Hospital is greatly appreciated. Special thanks to Nancy Buderer for statistical analysis and Sandra Puczynski for her inspiration.
Notes
This article was externally peer reviewed.
Funding: Funding of this research was provided by a grant from Prevent Child Abuse America.
Conflict of interest: none declared.
- Received for publication June 6, 2009.
- Revision received February 10, 2010.
- Accepted for publication February 15, 2010.




{kind=link}