
Abstract
Abnormal uterine bleeding is a common problem, and its management can be complex. Because of this complexity, concise guidelines have been difficult to develop. We constructed a concise but comprehensive algorithm for the management of abnormal uterine bleeding between menarche and menopause that was based on a systematic review of the literature as well as the actual management of patients seen in a gynecology clinic. We started by drafting an algorithm that was based on a MEDLINE search for relevant reviews and original research. We compared this algorithm to the actual care provided to a random sample of 100 women with abnormal bleeding who were seen in a university gynecology clinic. Discrepancies between the algorithm and actual care were discussed during audiotaped meetings among the 4 investigators (2 family physicians and 2 gynecologists). The audiotapes were used to revise the algorithm. After 3 iterations of this process (total of 300 patients), we agreed on a final algorithm that generally followed the practices we observed, while maintaining consistency with the evidence. In clinic, the gynecologists categorized the patient’s bleeding pattern into 1 of 4 types: irregular bleeding, heavy but regular bleeding (menorrhagia), severe acute bleeding, and abnormal bleeding associated with a contraceptive method. Subsequent management involved both diagnostic and treatment interventions, which often occurred simultaneously. The algorithm in this article is designed to help primary care physicians manage abnormal uterine bleeding using strategies that are consistent with the evidence as well as the actual practice of gynecologists.
Abnormal uterine bleeding is a common problem,1 and its management can be complex.2,3 Physicians are often unable to identify the cause of abnormal bleeding after a thorough history and physical examination.4,5 The management of abnormal bleeding can involve many decisions about diagnosis and treatment,3,6,7 which often occur simultaneously and without the benefit of comprehensive, evidence-based guidelines. The available evidence tends to focus on narrow treatment questions rather than the broad clinical approach to management.8,17 It is not difficult to find long lists of potential causes of abnormal bleeding, but primary care physicians need practical advice about how to approach this common problem.
Abnormal uterine bleeding includes both dysfunctional uterine bleeding and bleeding from structural causes. Dysfunctional bleeding can be anovulatory, which is characterized by irregular unpredictable bleeding, or ovulatory, which is characterized by heavy but regular periods (ie, menorrhagia).2 Structural causes include fibroids, polyps, endometrial carcinoma, and pregnancy complications. Abnormal bleeding can also result from contraceptive methods.
Many articles have reviewed the management of abnormal uterine bleeding,3,6,7,15,16,18,21 and they often include management algorithms. Although clinical algorithms have potential shortcomings,22,25 there are data to support their benefit to both physicians and patients.26,29 Rather than simply listing causes of abnormal bleeding, management algorithms force authors to face the same decisions clinicians face. Most algorithms simply state the author’s opinion about what to do. A MEDLINE search (1985 to present) found 76 review articles on abnormal uterine bleeding that appeared to address the topic comprehensively, and 24 of these included an algorithm. Of these 24 algorithms, 23 were based on the opinions of the authors and one was based on the available evidence.15 This single evidence-based algorithm addressed only one aspect of abnormal bleeding (menorrhagia), and most of the diagnostic recommendations were based on grade C evidence (expert opinion). Authors who study clinical algorithms recommend validating them to assure their feasibility in practice,30,32 but this is rarely done.27 None of the 24 identified algorithms were systematically compared with actual practice. Our goal was to produce a comprehensive algorithm for the management of abnormal uterine bleeding that was consistent with the evidence and feasible in practice.
Bleeding Patterns
We addressed abnormal uterine bleeding between menarche and menopause. We excluded premenarchal bleeding because of its rarity. We excluded amenorrhea and postmenopausal bleeding because their generally straightforward evaluation has been well described elsewhere.3,4,33,34 Postoperative, postpartum, and pregnancy-related bleeding were also excluded.
We found that gynecologists usually start the evaluation by determining the general pattern of abnormal bleeding (Figure 1). Thus, the algorithm starts by asking the physician to categorize patients according to the bleeding patterns defined in Table 1. Subsequent figures present algorithms for each pattern. The physician may have difficulty distinguishing prolonged periods from irregular bleeding, and we set an arbitrary bleeding duration of 12 days as a limit for menorrhagia. The distinction is important because endometrial sampling can often be avoided in patients with menorrhagia. However, the conservative approach would be to follow the irregular bleeding algorithm (Figure 3) in borderline cases because it calls for endometrial sampling in women at high risk for endometrial cancer.

Abnormal Uterine Bleeding between Menarche and Menopause.
Bleeding Patterns
Severe Acute Bleeding
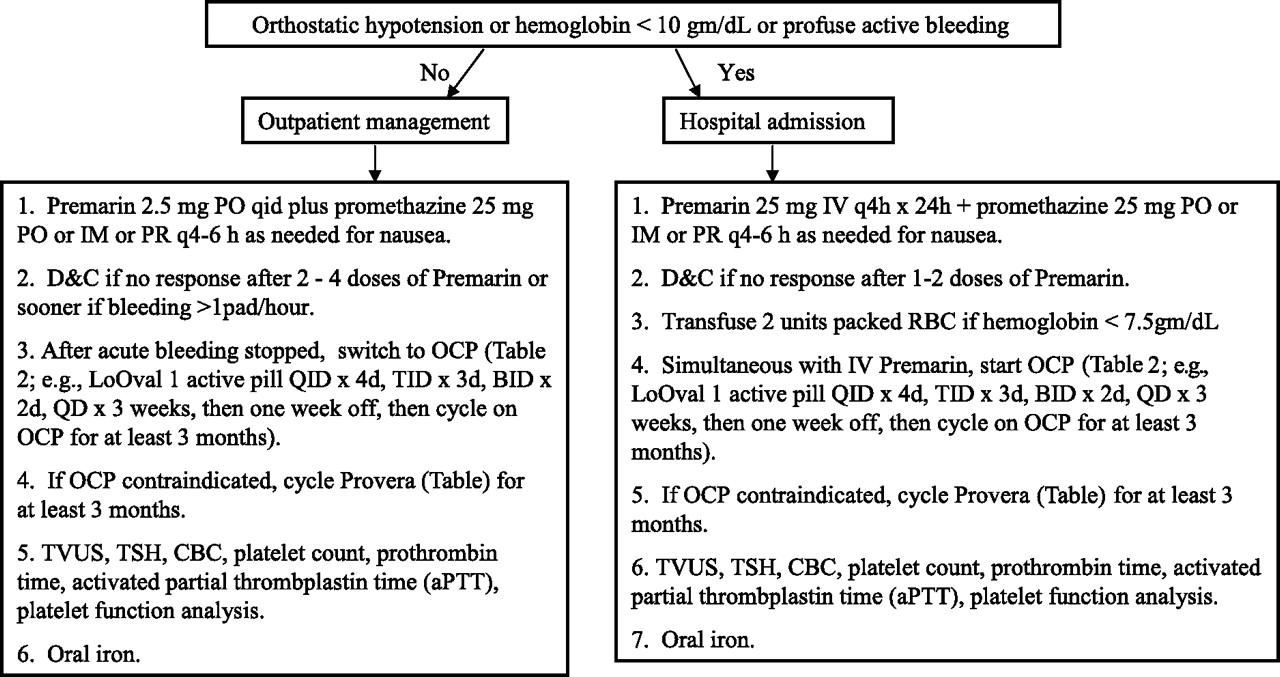
Severe acute uterine bleeding in the nonpregnant patient usually occurs in one of three settings: the adolescent with a coagulopathy (most commonly von Willebrand disease35,36), the adult with submucous fibroids, or the adult taking anticoagulants. Initial management is based on hemodynamic stability as outlined in Figure 2. The patient is given high-dose estrogen (orally or intravenously depending on bleeding severity) and then a tapering schedule of oral contraceptives. One common oral contraceptive regimen is ethinyl estradiol 30 μg/norgestrel 0.3 mg (eg, LoOvral) 1 active pill 4 times daily for 4 days, followed by 3 times daily for 3 days, followed by 2 times daily for 2 days, followed by once daily for 3 weeks. The patient then stops the pill for 1 week and then cycles in the usual manner, 3 weeks on and 1 week off, for at least 3 months. Once the patient is clinically stable, an investigation into the cause of bleeding includes screening coagulation studies and possibly transvaginal ultrasound (TVUS). The ultrasound may include a saline-infused sonohysterogram, especially when the endometrial stripe is thick, because of the increased sensitivity for endometrial polyps and submucous fibroids.37,38 In general, ultrasound is less likely to be helpful at menarche, and instead the evaluation for coagulopathy, especially von Willebrand disease, becomes more relevant.
Severe Acute Bleeding in the Nonpregnant Patient.
Irregular Bleeding
Irregular bleeding is a heterogenous category that includes metrorrhagia, menometrorrhagia, oligomenorrhea, prolonged bleeding that can last weeks or months, and other irregular patterns. These patterns were lumped together in the algorithm because their initial management is similar.
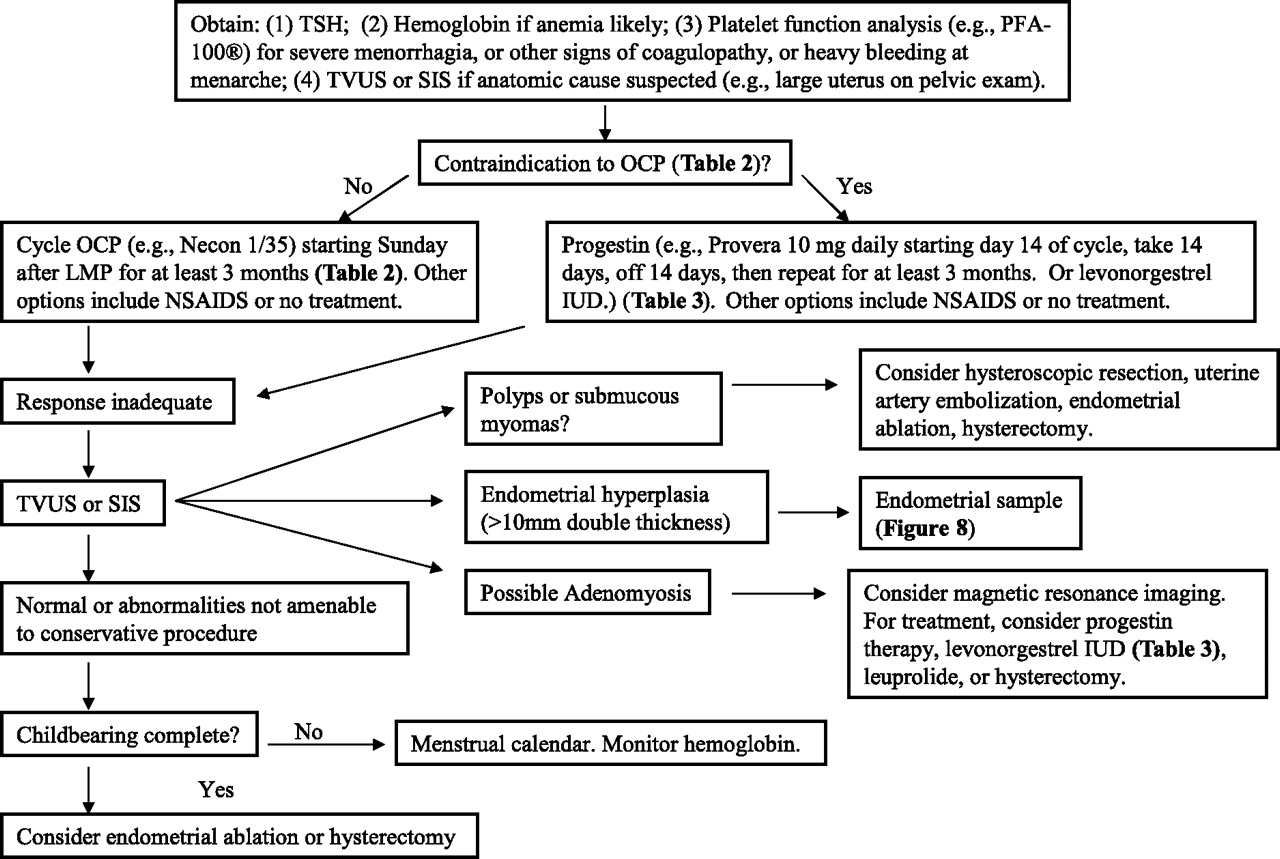
Patients with minor variations of normal bleeding may not require the evaluation outlined in Figure 3. For example, irregular bleeding within 2 years of menarche is usually due to anovulation, secondary to an immature hypothalamic-pituitary-ovarian axis.21,39,40 However, adolescents may request more than simple reassurance and can be offered oral contraceptives or a progestin as described in the algorithm (Figure 3). Missed periods and prolonged intervals are expected in perimenopause.41,42 Intervals may also decrease in the perimenopause, but repeated intervals less than 21 days or other irregular patterns require endometrial sampling. In any reproductive-aged woman, a few days of premenstrual spotting, if it is contiguous with the period, can be a normal variant, but the total duration should be less than 8 days.43 A few days of postmenstrual spotting, if it is contiguous with the period, can also be considered a normal variant.43 Postmenstrual spotting is sometimes caused by endometritis, which can be treated with 100 mg of doxycycline twice daily for 10 days. Brief midcycle spotting can occur at the time of ovulation due to the normal dip in serum estrogen levels.43 However, this is not common and should prompt an endometrial biopsy in women >35 years old.2 A single early period (<21 days) may not require an endometrial biopsy even in a woman over age 35 if subsequent periods are regular and no other abnormal bleeding occurs. Early periods and occasional missed periods are common in younger women and may result from mental stress or illness.44,45

Irregular Bleeding in the Nonpregnant Patient.
Before beginning hormonal therapy, systemic causes of abnormal uterine bleeding should be considered:
If the uterus is tender, indicating possible chronic endometritis, the patient should be tested for gonorrhea and chlamydia and initially treated with 100 mg of doxycycline twice daily for 10 days, pending culture results.46,47
Medications that can cause abnormal uterine bleeding include phenytoin, antipsychotics (eg, olanzapine, risperidone), tricyclic antidepressants (eg, amitriptyline, nortriptylene), and corticosteroids (eg, prednisone, dexamethasone).48
Abnormal uterine bleeding can result from advanced systemic disease such as liver failure or kidney failure.48 However, laboratory screening for these diseases in the absence of obvious clinical findings is not necessary because abnormal bleeding is a late manifestation. The exception is thyroid disease (hypothyroidism or hyperthyroidism), which should be screened for early in the evaluation with a thyroid-stimulating hormone (TSH).
Polycystic ovary syndrome (PCOS) is a common cause of abnormal uterine bleeding.49 The diagnostic criteria for PCOS include at least two of the following50,51:
Menstrual irregularity due to oligo- or anovulation.
Signs of androgen excess, either on physical examination (eg, hirsutism, acne) or laboratory testing (eg, elevated testosterone).
Evidence of polycystic ovaries by ultrasound.
In addition to these criteria, other causes of hyperandrogenism or abnormal bleeding must be excluded before making the diagnosis of PCOS. Conditions that should be ruled out include congenital adrenal hyperplasia (manifested by an elevated early morning 17-hydroxyprogesterone), androgen-secreting tumors (manifested by a serum testosterone >200 ng/dL or dehydroepiandrosterone sulfate >800 μg/dL), and hyperprolactinemia.
In women more than age 35 and those at risk for endometrial carcinoma (Figure 3), TVUS with or without a saline-infused sonohysterogram may be indicated before, after, or instead of endometrial biopsy. TVUS can detect endometrial polyps, uterine myomas, and endometrial hyperplasia.52,53 Endometrial biopsy can detect hyperplasia, atypia, and carcinoma. The conservative approach is to do the endometrial biopsy whether or not a TVUS is obtained. However, other factors may enter this decision:
TVUS may be indicated if the patient will likely require operative management (eg, office biopsy would be a technical challenge or fibroids suspected on physical examination or probable need for hysteroscopy or endometrial ablation).
High-quality TVUS is not available in many locations. Also TVUS is costly and insurance status may influence the order of testing.
One option is to first rule out neoplasia with the endometrial biopsy, then start hormonal therapy, and then obtain a TVUS only if abnormal bleeding persists despite hormonal therapy.
TVUS is less invasive and less painful than endometrial biopsy. One study reported experience with initial TVUS and no further evaluation if the double-thickness endometrial stripe was <5 mm.54 However, the conservative approach remains endometrial biopsy in women at risk for endometrial carcinoma.
Menorrhagia
Menorrhagia is defined as blood loss greater than 80 mL per cycle. A more pragmatic but less precise definition is simply the patient’s perception of excessive blood loss. Unfortunately, these judgments do not correlate well with actual blood loss.55 Menorrhagia can often be managed without endometrial sampling because regular bleeding, even if heavy, is less concerning for endometrial cancer. However, if the bleeding is prolonged (>7 days) or does not respond to hormonal therapy as outlined in Figure 4, further evaluation with TVUS or endometrial sampling is indicated. Platelet function analysis to screen for von Willebrand disease should be ordered in women with severe menorrhagia or other signs of coagulopathy.36,56,58 For treatment, women can be offered oral contraceptives if not contraindicated (Table 2), progestins (Table 3), nonsteroidal anti-inflammatory drugs, or observation. The decision between oral contraceptives and progestins is often based on contraindications to estrogen, most commonly smoking. A recent clinical trial found that the levonorgestrel intrauterine device (IUD) (Mirena) resulted in comparable quality of life scores and lower costs compared with hysterectomy in women with menorrhagia.59 Women who prefer no hormones can be started on nonsteroidal anti-inflammatory drugs, which decrease blood loss.60,61
Menorrhagia in the Nonpregnant Patient.
Oral Contraceptive Pill
Progestin Therapy
Hormonal Contraception
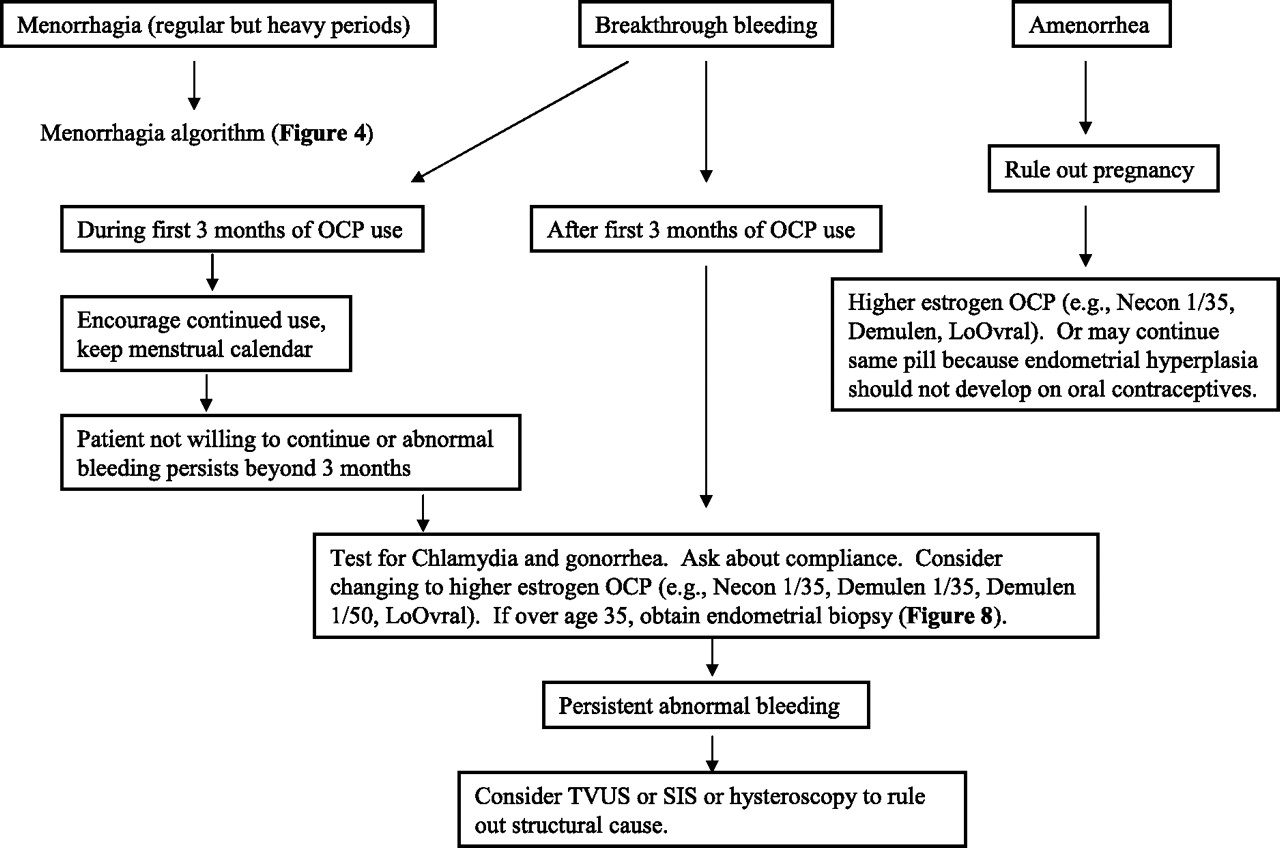
Breakthrough bleeding occurs commonly with low-dose oral contraceptive pills (Figure 5). If the abnormal bleeding persists after the first 3 months, a higher dose pill can be used, as indicated in Figure 5. Gonorrhea and chlamydia in association with oral contraceptives commonly leads to abnormal bleeding, and cervical cultures should be obtained.

Oral Contraceptive Pill-associated Bleeding.
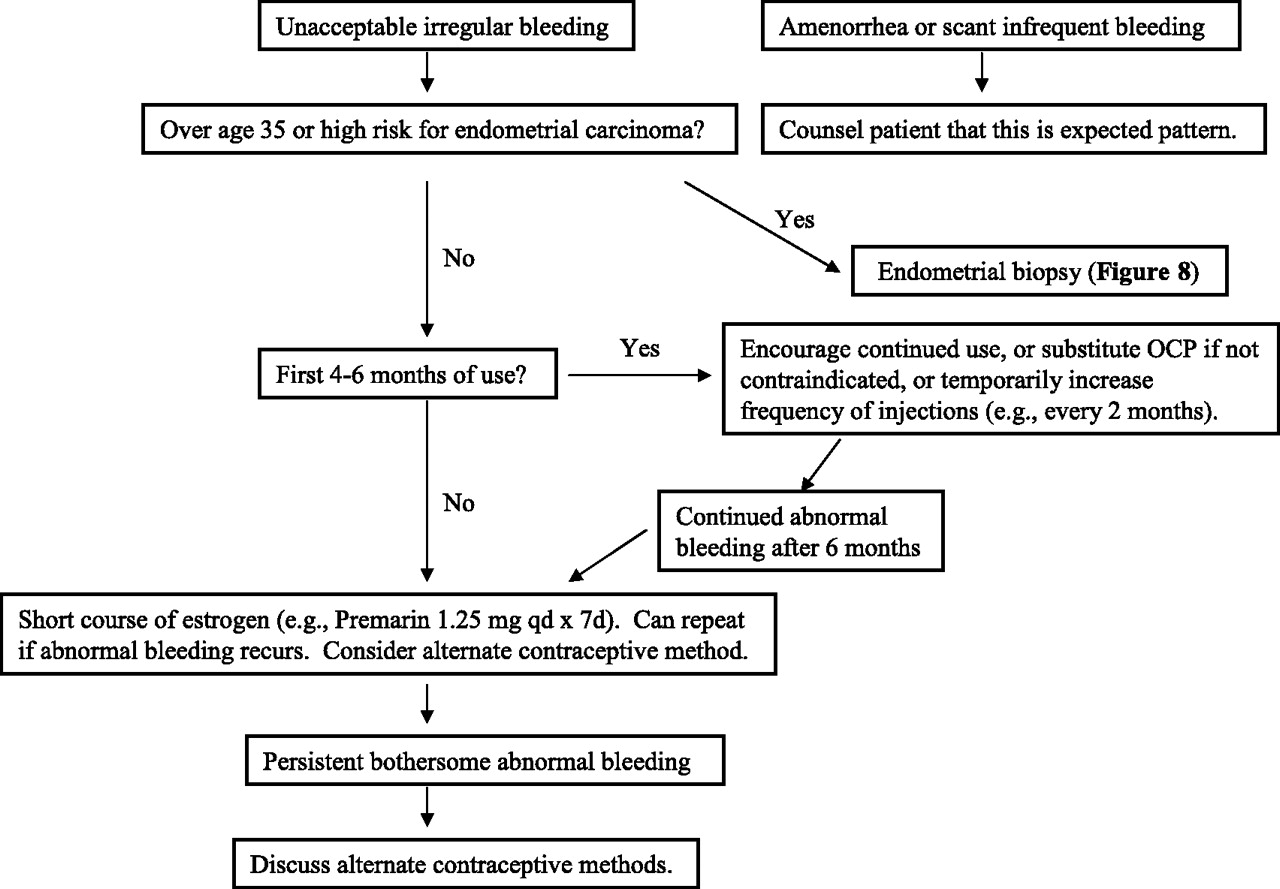
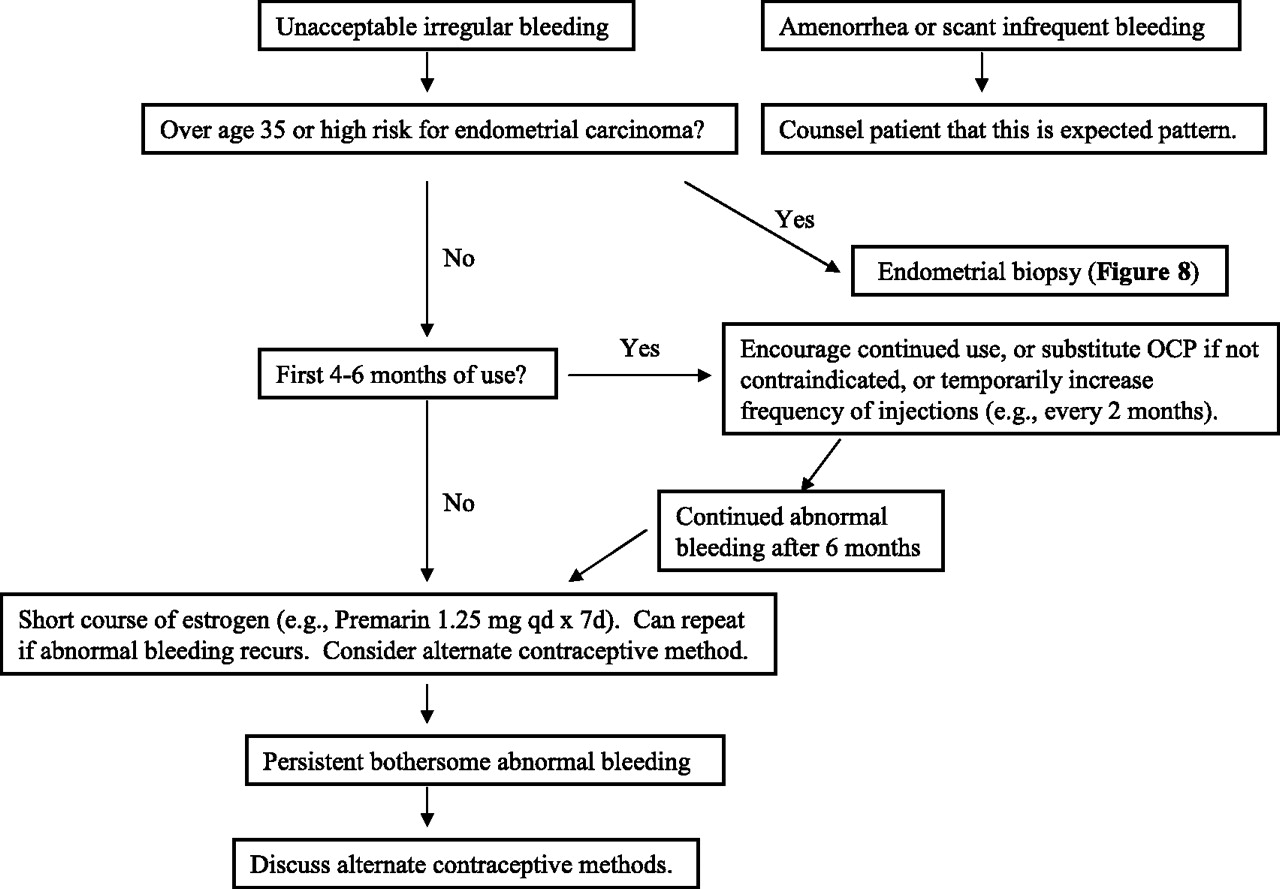
Patients on depo-medroxyprogesterone with persistent irregular bleeding can be treated with a 7-day course of estrogen (eg, 1.25 mg of Premarin daily, 1 mg of estradiol daily, or an estrogen patch such as 0.1 mg Climara). This can be repeated if the abnormal bleeding recurs.
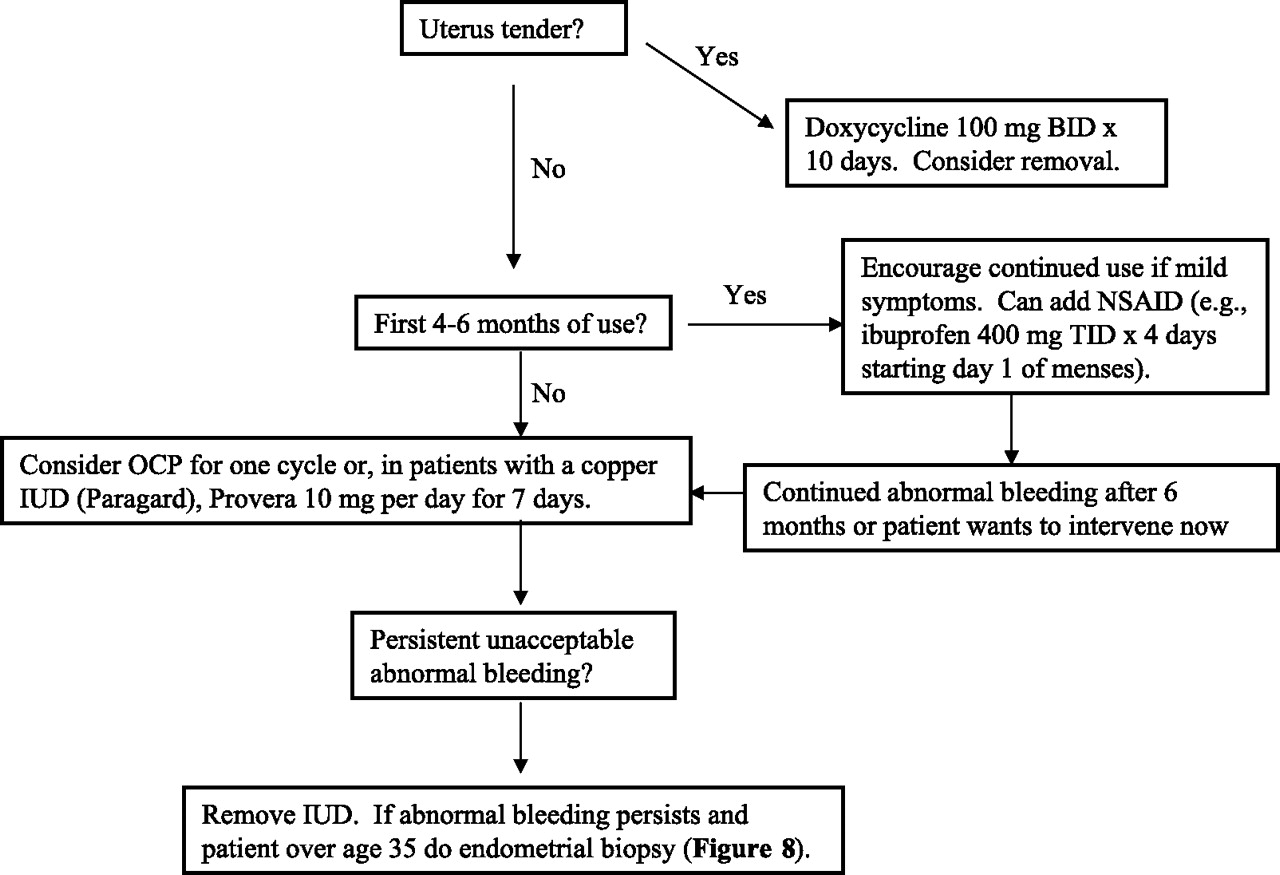
In patients with an IUD, abnormal bleeding may be associated with endometritis. After culturing the cervix, patients with a tender uterus can be treated with 100 mg of doxycycline twice daily for 10 days and possible removal of the IUD. In the absence of endometritis, patients with a copper IUD (Paragard) can be treated with one cycle of the oral contraceptive pill or 10 mg of medroxyprogesterone daily for 7 days. Patients with a progestin-releasing IUD (Mirena, Progestasert) can be treated with one cycle of the oral contraceptive pill. If the abnormal bleeding persists, the IUD can be removed and alternative contraceptive methods discussed.
Comment
In this review, we developed an algorithm for the management of abnormal uterine bleeding and compared it to actual practice. The algorithm is generally consistent with previous comprehensive algorithms. For example, Albers and colleagues presented an algorithm that covered several pages in a recent review.3 Space limitations forced the authors to use general recommendations such as “medical management” rather than specific drugs. Other algorithms have solved the space problem by limiting their algorithms to single aspects of abnormal bleeding, such as only menorrhagia15,62,63 or only amenorrhea.64,67 Some reviews start from the pathophysiologic perspective, addressing topics such as “anovulatory bleeding”2 or “dysfunctional uterine bleeding,”68 but this approach may be less helpful to clinicians because patients do not present with these labels.
Little is known about how to develop clinical algorithms. Authors recognize the importance of validating clinical algorithms, but they have little advice about how to do it or even what is meant by “validation.”30,31 Validation could involve building algorithms that optimize patient preferences, physician preferences, compliance with the evidence, conformity with physicians’ diagnostic reasoning processes, or, as in this study, conformity with actual practice. Algorithms could be tested by determining whether physicians follow the “correct” path (validity) and whether they follow the same path (reliability).
Although the algorithm presented in this article is based on the practice of gynecologists in a tertiary setting, the recommendations should be generally applicable to primary care settings in the United States because they consist of routine tests, such as pregnancy tests and endometrial biopsies, and simple treatments, such as oral contraceptives and progestins.
The algorithm is lengthy, and busy clinicians might find it unwieldy. However, a clinician with an individual patient could focus on only the first figure (Figure 1) plus the one other figure that addresses the specific bleeding pattern. Although we could have shortened the algorithm by using general recommendations, such as “medical therapy,” or “appropriate laboratory evaluation,” we wanted a practical tool that could stand alone at the point of care.
We sought to develop a good algorithm, but it was not clear how to define “good.” A good algorithm might be cost-effective, evidence-based, intuitive, efficient (arrives at a treatment plan quickly without unnecessary steps), comprehensive (no need to consult other information resources), noninvasive (avoids endometrial biopsy when possible), practice-based (works in practice), filled with action-oriented advice (“don’t just talk about the problem, tell me what to do”), and able to account for patient preferences. A good algorithm should lead to favorable patient outcomes in a randomized clinical trial, but trials involving comprehensive algorithms for complex problems, such as abnormal uterine bleeding, are generally not feasible.
The algorithm in this study was initially based on the evidence but modified to match the actual care of patients. The strength of the evidence for the major recommendations in the algorithm are summarized Table 4. The validation procedures we followed were time consuming and may not be practical for algorithms that address other topics. However, even limited attempts to test an algorithm or compare it with actual patient care might reassure authors and readers of its usability in practice.
Strength of Evidence for Major Management Recommendations
Appendix
Handheld Computer Version of Algorithm for the Management of Abnormal Uterine Bleeding
Initial approach
History and physical examination
Rule out pregnancy
Determine bleeding pattern
Severe acute bleeding
Irregular bleeding
Menorrhagia
Contraceptive method (oral contraceptive pill (OCP), depo-medroxyprogesterone, IUD)
Severe acute bleeding (not pregnant)
Orthostatic hypotension or hemoglobin <10 g/dL or profuse bleeding. Admit to the hospital. Premarin 25 mg IV q4 hours × 24 hours + 25 mg of promethazine PO or IM or per rectum every 4 to 6 hours as needed for nausea. Dilation and curettage (D&C) if no response after 1 to 2 doses of Premarin. Transfuse if hemoglobin <7.5 g/dL. Simultaneous with IV Premarin, start LoOvral, 1 active pill QID × 4d, TID × 3d, BID × 2d, QD × 3 weeks, then one week off, then cycle for at least 3 months. If OCP contraindicated, cycle 10 mg of Provera for 14 days, off 14 days, on 14 days, and so on for at least 3 months. Obtain TVUS, TSH, complete blood cell count (CBC), platelet count, prothrombin time, activated partial thromboplastin time, and platelet function analysis. Start oral iron.
No orthostatic hypotension, hemoglobin ≥10 g/dL, bleeding not profuse. Outpatient management: 2.5 mg of Premarin PO QID plus 25 mg of promethazine PO or IM or per rectum every 4 to 6 hours as needed for nausea. D&C if no response after 2 to 4 doses of Premarin or sooner if bleeding >1 pad/hour. After acute bleeding start LoOvral, 1 active pill QID × 4d, TID × 3d, BID × 2d, QD × 3 weeks, then 1 week off, then cycle for at least 3 months. If OCP contraindicated, cycle 10 mg of Provera for 14 days, off 14 days, on 14 days, and so on for at least 3 months. Obtain TVUS, TSH, CBC, platelet count, prothrombin time, activated partial thromboplastin time, and platelet function analysis. Start oral iron.
Irregular bleeding in nonpregnant patient
TSH. Prolactin if oligomenorrhea.
If more than age 35 or prolonged unopposed estrogen, obtain endometrial biopsy and consider TVUS.
Consider as a cause endometritis (tender uterus), medications (phenytoin, antipsychotics, tricyclic antidepressants, corticosteroids), advanced systemic disease, or polycystic ovary syndrome.
If the patient does not want to achieve pregnancy, start oral contraceptive (eg, Necon 1/35) and cycle at least 3 months. If the oral contraceptive is contraindicated, start 10 mg of Provera QD for 14 days, off 14 days, on 14 days, and so on for at least 3 months. If abnormal bleeding persists, offer higher dose oral contraceptive (eg, Demulen 1/50) or higher dose Provera (20 mg, 30 mg, 40 mg, 60 mg, 80 mg). If abnormal bleeding persists, consider TVUS and endometrial biopsy.
Contraindications to oral contraceptives include history of thromboembolic event or stroke, estrogen-dependent tumor, active liver disease, pregnancy, hypertriglyceridemia, smoking more than 15 cigarettes per day when age is ≥35.
Menorrhagia in nonpregnant patient
TSH. Hemoglobin. Consider platelet function analysis. Consider TVUS if abnormal uterus on pelvic examination.
Cycle oral contraceptive (eg, Necon 1/35). If oral contraceptive contraindicated, 10 mg of Provera QD x 14 days, off 14 days, on 14 days, and so on for at least 3 months. Other options include nonsteroidal antiinflammatory drugs (eg, 400 mg of ibuprofen TID for 4 days, staring day 1 of menses) or no treatment.
If response inadequate, obtain TVUS to identify polyps, myomas, endometrial hyperplasia, adenomyosis.
Oral contraceptive pill-associated bleeding
Menorrhagia. Refer to menorrhagia algorithm above.
Breakthrough bleeding. If breakthrough bleeding occurs during the first 3 months, encourage continued use. If breakthrough bleeding occurs after 3 months of use or patient requests intervention sooner, test for chlamydia and gonorrhea, ask about compliance, consider changing to higher estrogen pill (eg, Necon 1/35, Demulen 1/35, Demulen 1/50, LoOvral). If more than age 35, obtain endometrial biopsy.
Amenorrhea. Rule out pregnancy. Consider higher estrogen pill (eg, Necon 1/35, Demulen 1/35, Demulen 1/50, LoOvral). Or may continue same pill because endometrial hyperplasia should not develop on oral contraceptives.
Depo-medroxyprogesterone or progesterone-only pill-associated bleeding.
Amenorrhea. Advise that amenorrhea or scant bleeding is expected.
If unacceptable irregular bleeding and patient more than age 35 or otherwise at risk for endometrial carcinoma, do endometrial biopsy.
If less than age 35 and not otherwise at high risk for endometrial carcinoma and first 4 to 6 months of use, can encourage continued use or substitute oral contraceptive, or temporarily increase frequency of injections (eg, every 2 months).
If less than age 35 and not otherwise at high risk for endometrial carcinoma and after first 4 to 6 months of use, offer 1.25 mg of Premarin QD for 7 days. Can repeat Premarin course if abnormal bleeding recurs. Consider other methods of contraception if bleeding persists.
IUD-associated bleeding
Uterus tender; 100 mg of doxycycline BID for 10 days. Consider removal.
First 4 to 6 months of use. Encourage continued use. Can offer NSAID (eg, 400 mg of ibuprofen TID for 4 days, starting day 1 of menses).
After 4 to 6 months of use, consider oral contraceptive for one cycle or, if copper IUD, 10 mg of Provera QD for 7 days. If unacceptable bleeding persists, consider removal.
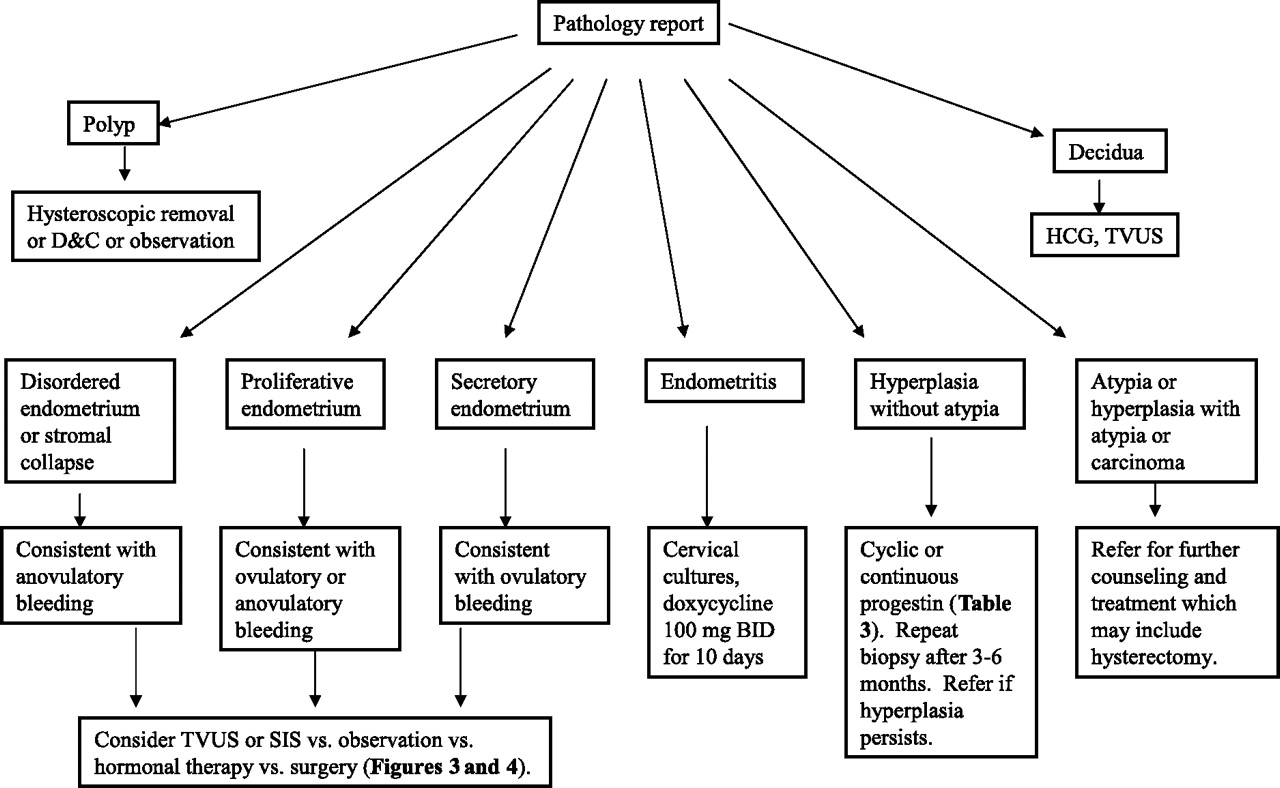
Endometrial biopsy results (eg, pipelle aspiration; Figure 8).
Polyp. Consider hysteroscopic removal or D&C or observation.
Disordered endometrium or stromal collapse or proliferative endometrium or secretory endometrium. Return to appropriate algorithm based on bleeding pattern.
Endometritis; 100 mg of doxycycline BID for 10 days.
Hyperplasia without atypia. Cyclic or continuous progestin (eg, 10 mg of Provera QD for 14 days, off 14 days, on 14 days, and so on). Repeat biopsy after 3 to 6 months. Refer if hyperplasia persists.
Atypia or hyperplasia with atypia or carcinoma. Refer for further counseling and treatment.
Depo-medroxyprogesterone or Progesterone Only Pill-associated Bleeding.
Intrauterine Device-associated Bleeding.
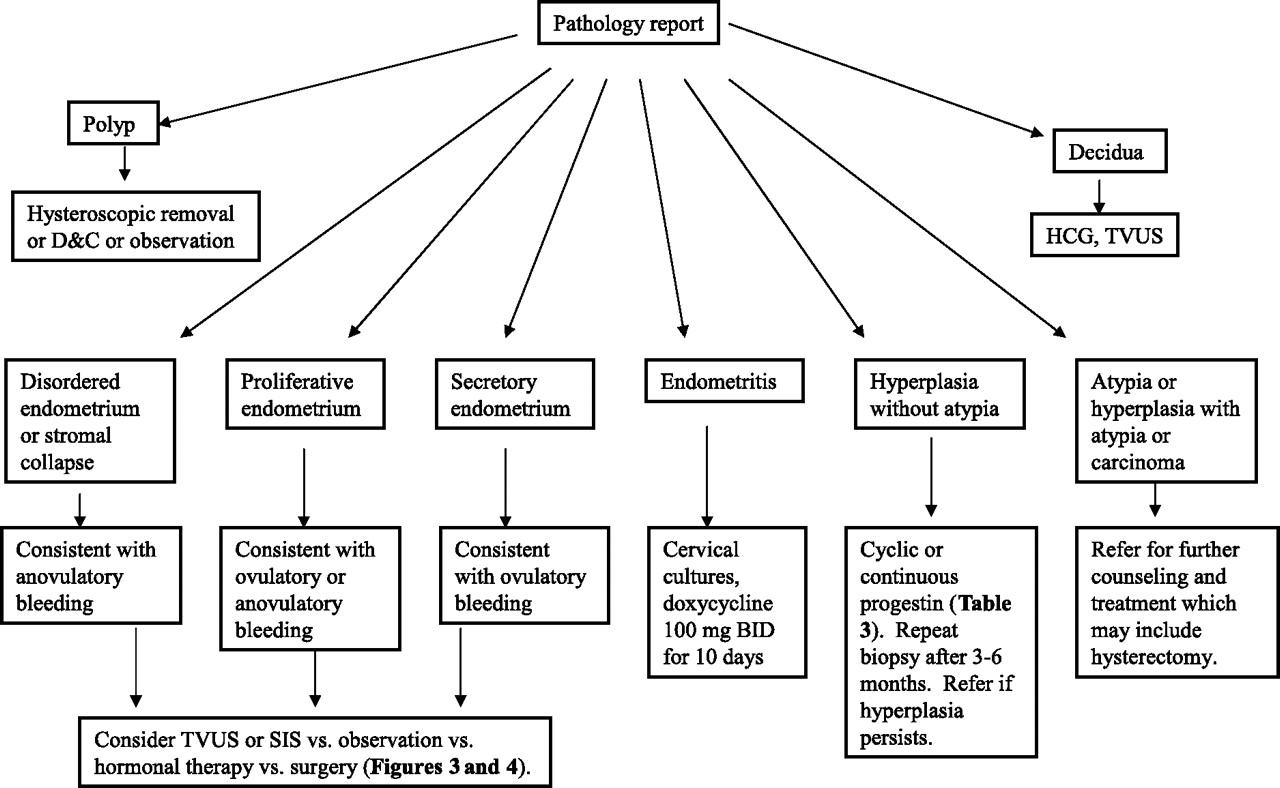
Endometrial Biopsy (Pipelle aspiration).
Notes
This article was externally peer-reviewed.
Conflict of interest: none declared.
- Received for publication April 24, 2006.
- Revision received August 10, 2006.
- Accepted for publication August 24, 2006.
References




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- CLINICAL BLEEDING PATTERNS AND MANAGEMENT TECHNIQUES OF ABNORMAL UTERINE BLEEDING IN WESTERN KENYA.
- Content Usage and the Most Frequently Read Articles of 2018
- Content Usage and the Most Frequently Read Articles in 2010
- Content Usage and the Most Frequently Read Articles in 2009
- Introduction of More Editorial Board Members and New Guest Commentary Feature
- Introduction of More Editorial Board Members and the Most Frequently Read Articles in 2008
- Inside the March/April 2008 Issue and the Most Frequently-Read Articles in 2007
- North American Primary Care Research Group President's Award