
Article Figures & Data
Figures
- Figure 1.
Abnormal Uterine Bleeding between Menarche and Menopause.
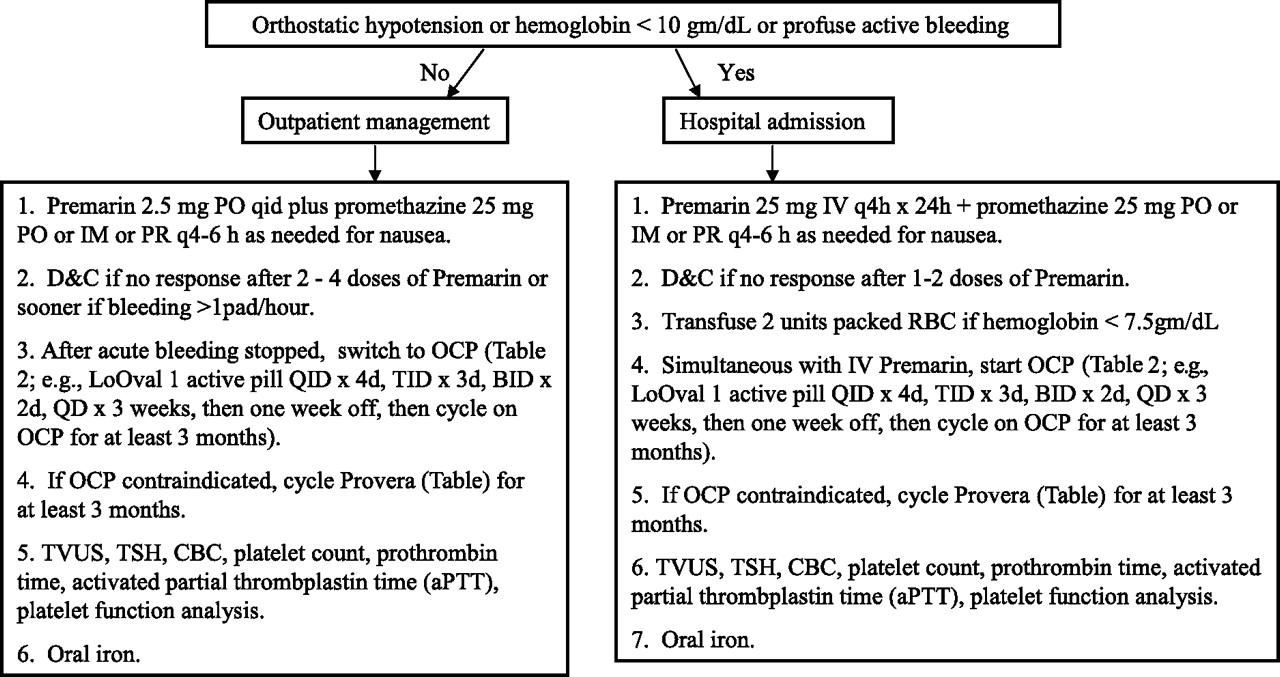
- Figure 2.
Severe Acute Bleeding in the Nonpregnant Patient.
- Figure 3.
Irregular Bleeding in the Nonpregnant Patient.
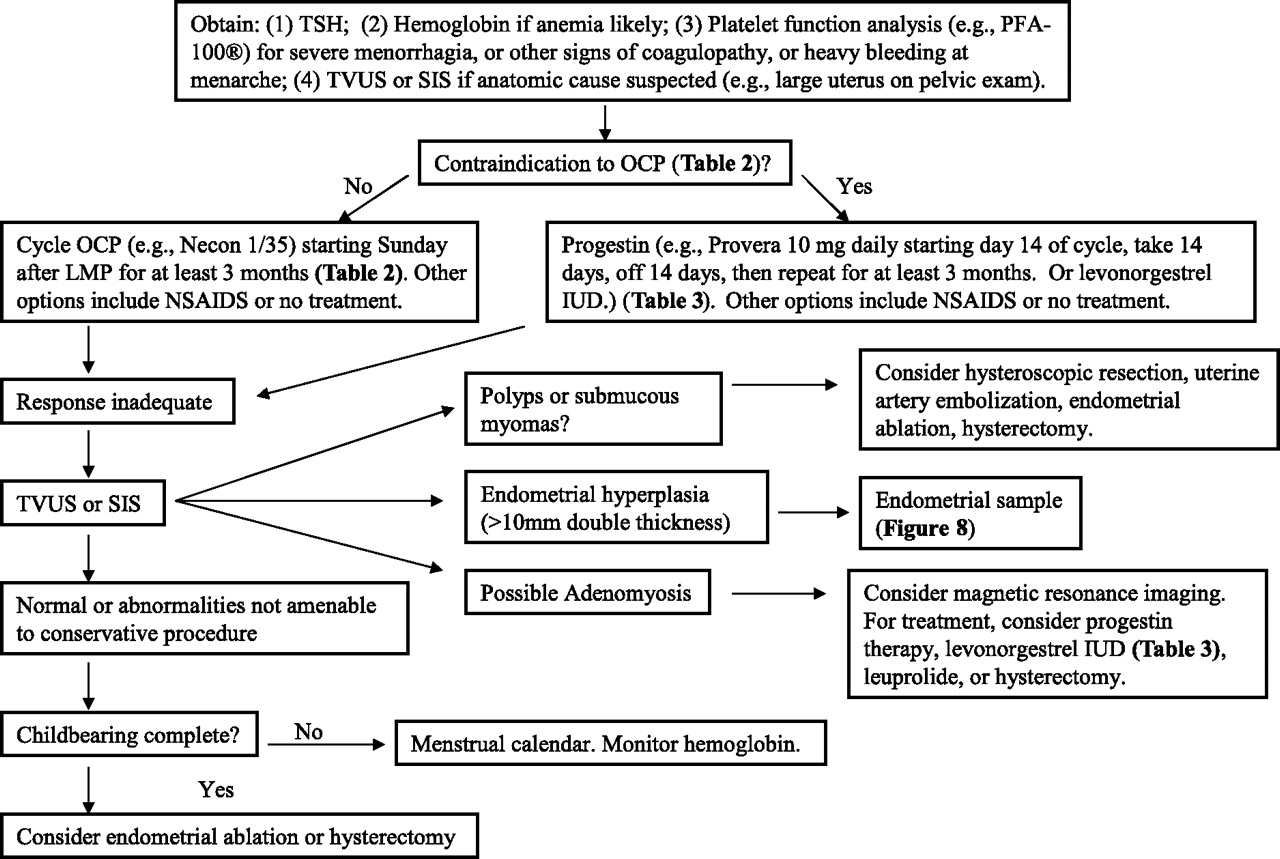
- Figure 4.
Menorrhagia in the Nonpregnant Patient.
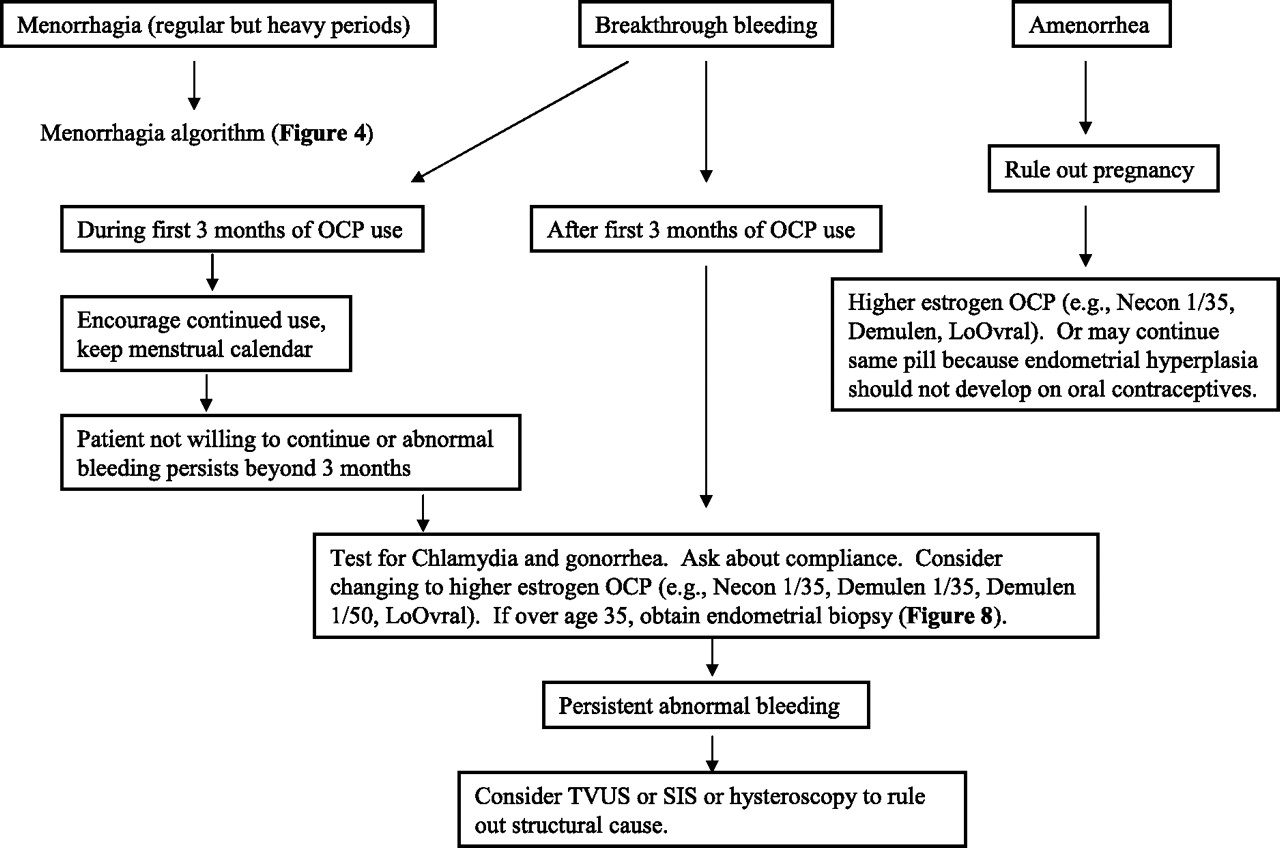
- Figure 5.
Oral Contraceptive Pill-associated Bleeding.
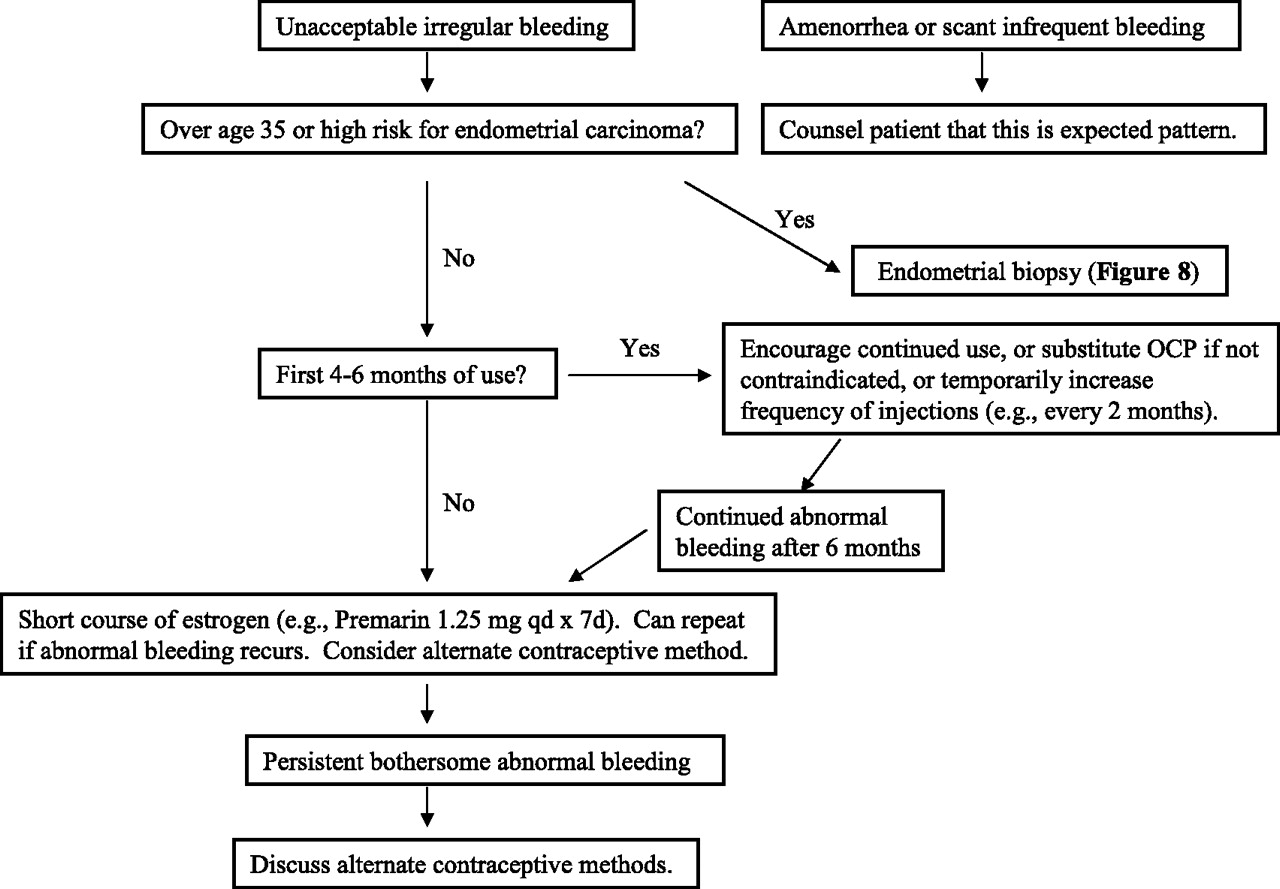
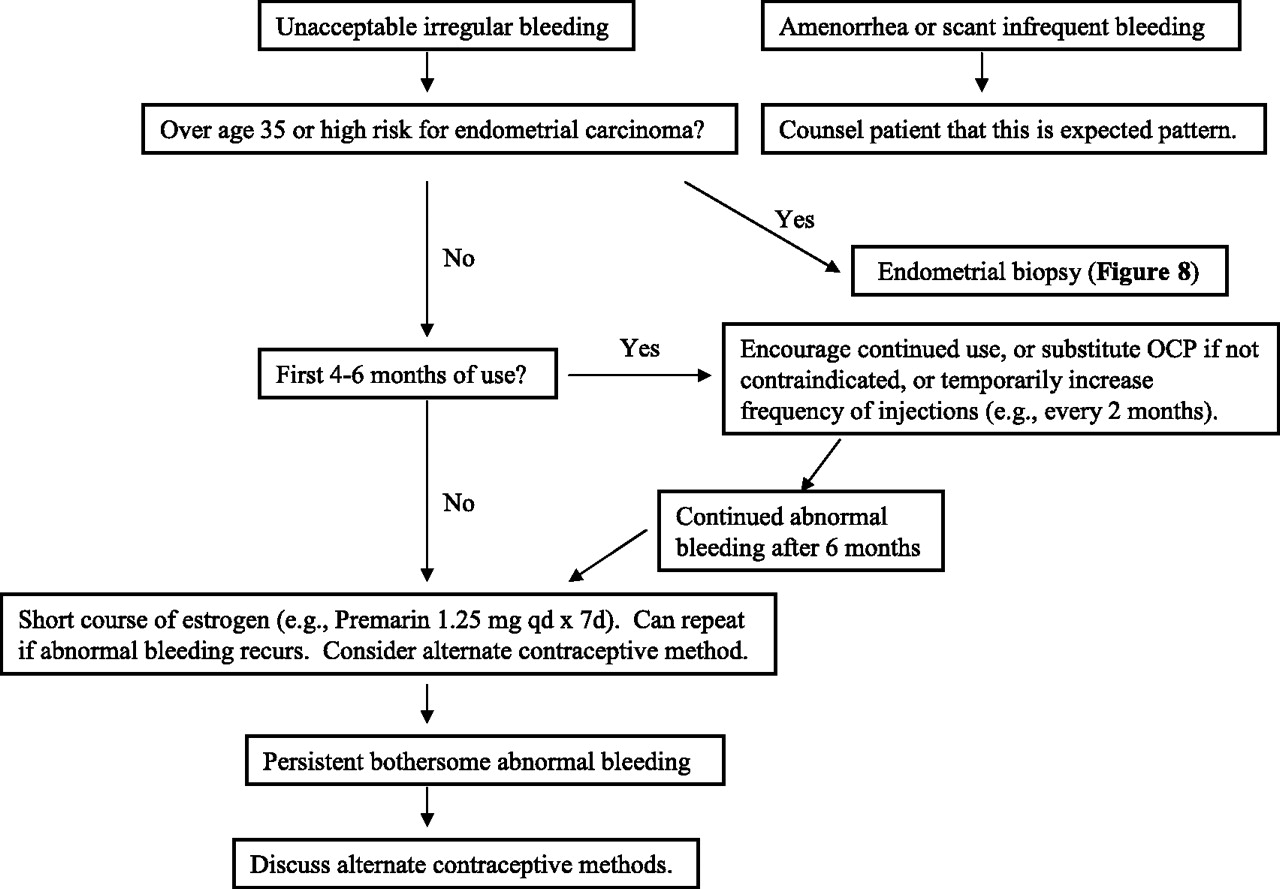
- Figure 6.
Depo-medroxyprogesterone or Progesterone Only Pill-associated Bleeding.
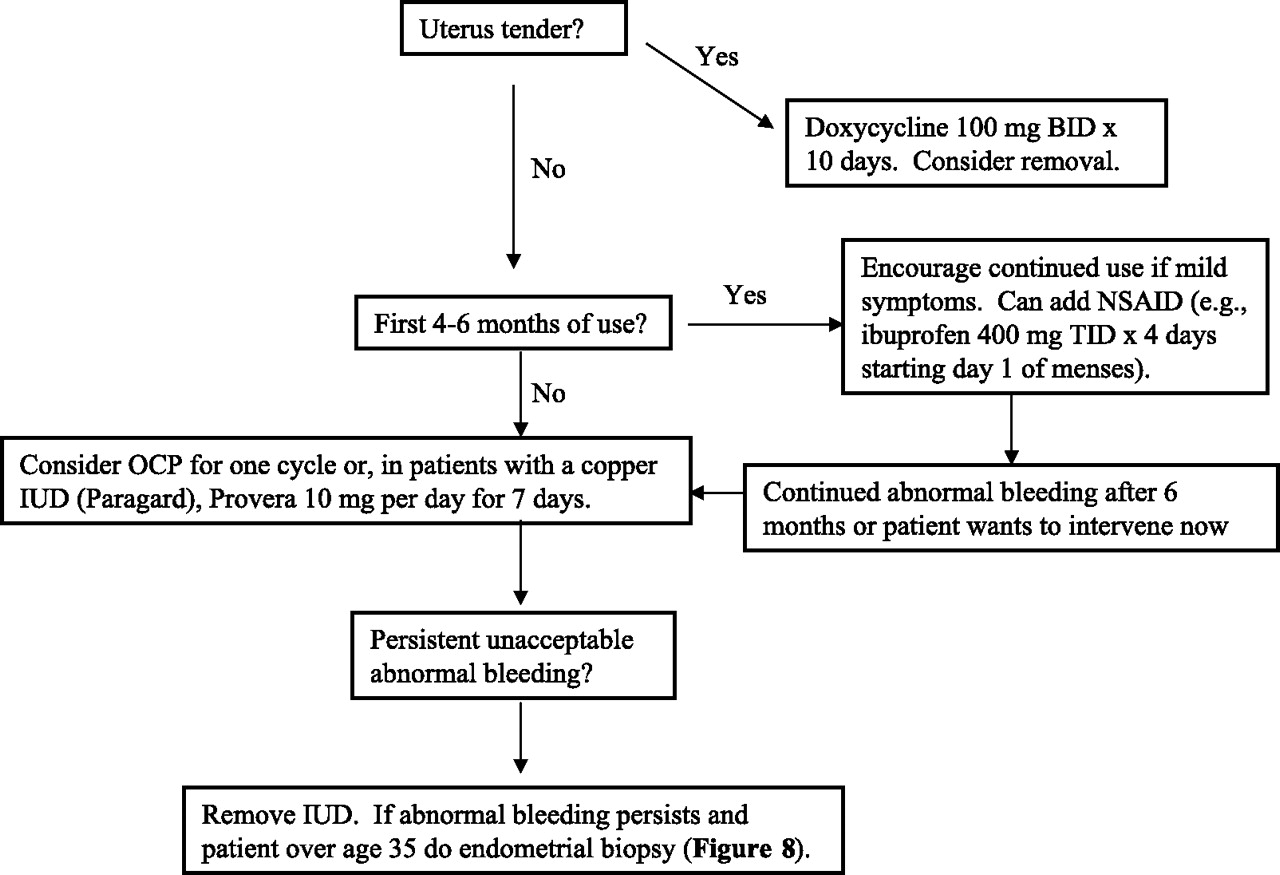
- Figure 7.
Intrauterine Device-associated Bleeding.
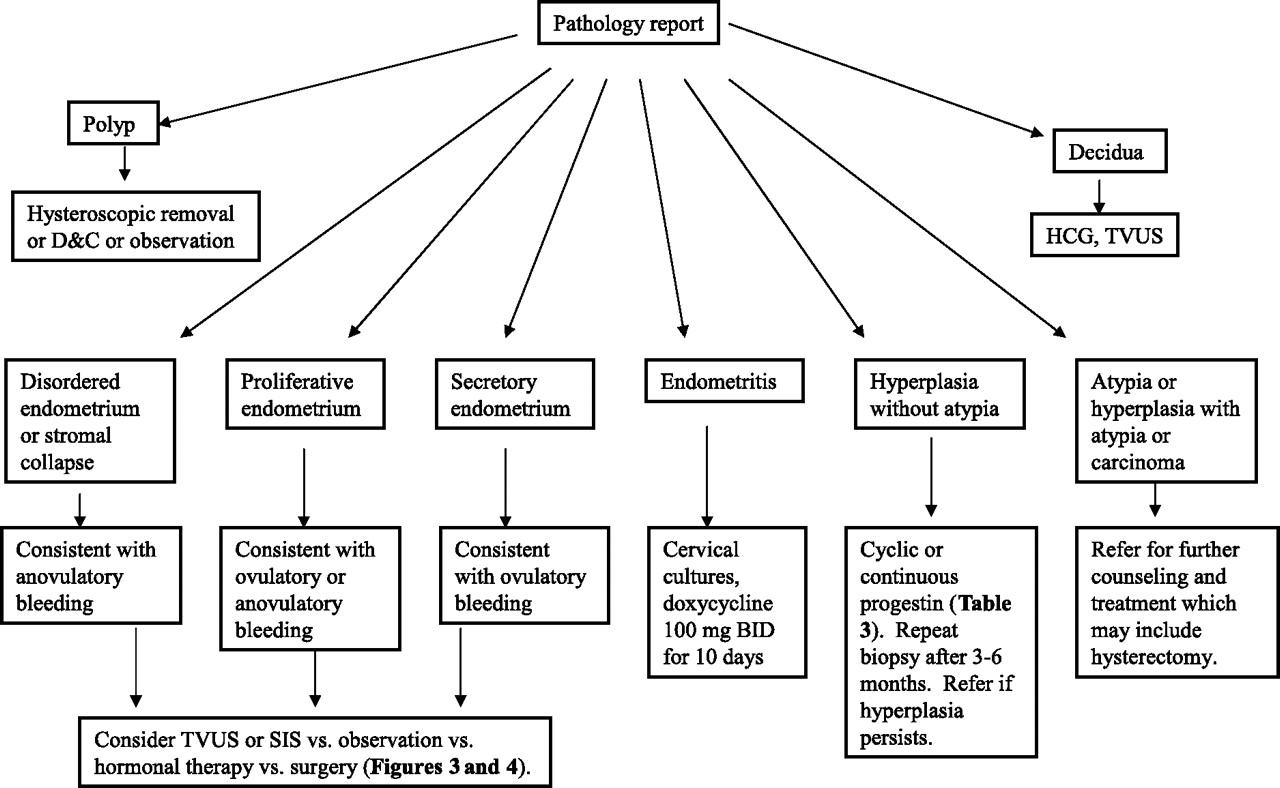
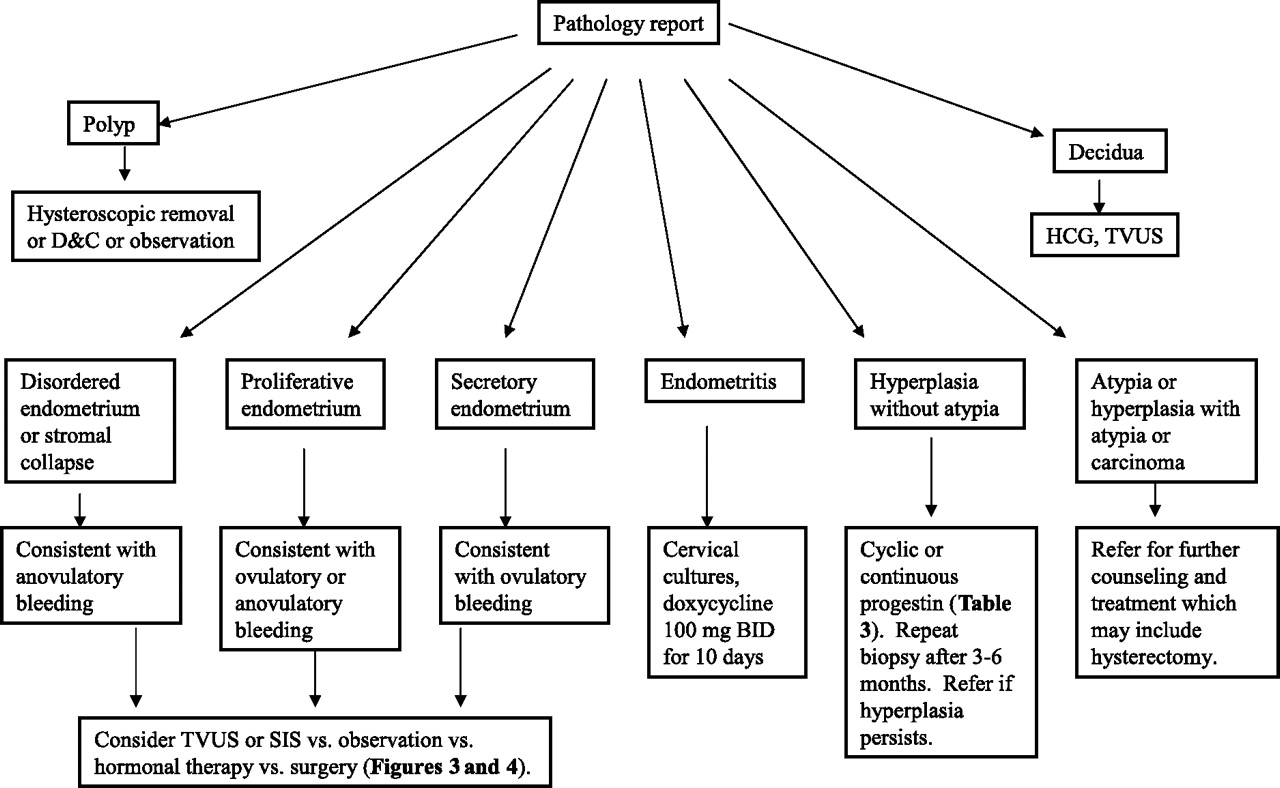
- Figure 8.
Endometrial Biopsy (Pipelle aspiration).



Tables
Normal: The normal interval is 21 to 35 days. The normal duration of bleeding is 1 to 7 days. The amount should be less than 1 pad or tampon per 3-hour period Severe acute bleeding: Bleeding that requires more than one pad/tampon per hour or vital signs indicating hypovolemia. Irregular bleeding: Includes metrorrhagia, menometrorrhagia, oligomenorrhea, prolonged bleeding, intermenstrual bleeding, or other irregular pattern. Menorrhagia: Heavy but regular cyclic bleeding plus >7 days of bleeding or clots or iron deficiency anemia. Prolonged bleeding >12 days should be considered irregular regardless of cyclic pattern. Combination Oral Contraceptive Pill If the goal is to achieve amenorrhea, the OCP can be given continuously, but is usually withdrawn every 3 to 4 months to allow endometrial shedding and avoid irregular bleeding. Irregular bleeding In most women, suspect a thin endometrium and cycle on OCP (eg, Necon 1/35) for at least 3 months. If PCOS is suspected (ie, thick endometrium), consider cyclic progestin (Table 3), and then continue cyclic progestin or switch to OCP. If there is heavy bleeding at the time of the visit, start a moderate-estrogen OCP (eg, LoOvral) one active pill QID × 4 days, then one TID × 3 days, then one BID × 2 days, then daily × 3 weeks, then skip 1 week, then cycle on OCP for at least 3 months. Menorrhagia Can start OCP any time but typically on Sunday following first day of menses. Contraindications to OCP Previous thromboembolic event or stroke History of estrogen-dependent tumor Active liver disease Pregnancy Hypertriglyceridemia Older than 35 years and smokes >15 cigarettes per day Older than 40 years is not a contraindication but many physicians favor progestin for this age group. Progestin therapy In most cases, use a cyclic progestin, usually medroxyprogesterone (Provera) because of its low cost. If PMS-like side effects are unacceptable, consider micronized progesterone (Prometrium), norethindrone (Aygestin), or megestrol (Megace). Cyclic progestins Start medroxyprogesterone 10 mg daily for 14 days, then off 14 days, then on 14 days, and so on without regard to bleeding pattern. If bleeding occurs before completing the 14-day course, the patient can double the dose (20 mg) and ‘reset the clock’ (count the first day of bleeding as day 1 and start medroxyprogesterone on day 14) or not reset the clock and continue the schedule without regard to bleeding pattern. If the patient is bleeding at the time of the visit, start medroxyprogesterone 10 mg daily and increase every 2 days as needed to stop the bleeding (20 mg, 30 mg, 40 mg, 60 mg, 80 mg) until bleeding stops. However, the patient should be warned that intolerable PMS-like side effects may develop with high doses. Continue for 14 days and then cycle 14 days on, 14 days off, and so on. Continuous progestins Continuous progestins may be indicated if the goal is to achieve amenorrhea (eg, busy professional or athlete, intractable menstrual migraine, catamenial seizures, severe mental retardation). Maintaining amenorrhea is often more difficult than cycling a progestin (ie, there may be unpredictable spotting). Options include: — Oral progestin: medroxyprogesterone Provera 10 to 20 mg daily or ‘Minipill’ (eg, 0.35 mg of norethindrone daily) — Depo-medroxyprogesterone (Depo-Provera) 150 mg IM every 13 weeks. Often used in adolescents to improve compliance. Less often used in ages >40 years due to risk of osteoporosis. — Levonorgestrel IUD (Mirena). Recommendation Strength of Recommendation* TSH. Obtain a thyroid-stimulating hormone (TSH) serum level in women with irregular bleeding or menorrhagia.69–73 B Age 35. Obtain an endometrial biopsy in women over age 35 with irregular bleeding.2,74 B Unopposed estrogen. Obtain an endometrial biopsy in women with prolonged unopposed estrogen regardless of age (most commonly, a woman with polycystic ovary syndrome (PCOS) with few or no periods for more than 2 years).2,75 C Transvaginal ultrasound. Consider transvaginal ultrasound or saline-infused sonohysterogram for perimenopausal women with irregular bleeding.4,54,76 C Hormonal therapy for irregular bleeding. Offer oral contraceptives or a progestin for cycle regulation in women with irregular bleeding, after ruling out structural causes, systemic causes, and contraindications to the oral contraceptive.2,8,77 B Hormonal therapy for menorrhagia. Offer oral contraceptives or a progestin to decrease bleeding in women with menorrhagia after ruling out structural causes, systemic causes, and contraindications to the oral contraceptive.8,10,13,77–79 B Nonsteroidal anti-inflammatory drugs for menorrhagia. Offer nonsteroidal anti-inflammatory drugs for women with menorrhagia, after ruling out structural causes and systemic causes.60,61 B * Strength of recommendation classified according to the 3-component SORT system80: A, recommendation based on consistent and good-quality patient-oriented evidence80; B, recommendation based on inconsistent or limited quality patient-oriented evidence80; C, recommendation based on consensus, usual practice, opinion, disease-oriented evidence, or case series for studies of diagnosis, treatment, prevention, or screening.80




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- CLINICAL BLEEDING PATTERNS AND MANAGEMENT TECHNIQUES OF ABNORMAL UTERINE BLEEDING IN WESTERN KENYA.
- Content Usage and the Most Frequently Read Articles of 2018
- Content Usage and the Most Frequently Read Articles in 2010
- Content Usage and the Most Frequently Read Articles in 2009
- Introduction of More Editorial Board Members and New Guest Commentary Feature
- Introduction of More Editorial Board Members and the Most Frequently Read Articles in 2008
- Inside the March/April 2008 Issue and the Most Frequently-Read Articles in 2007
- North American Primary Care Research Group President's Award