
Abstract
Background: There is great interest in intensive primary care interventions to address high utilization among medically and socially complex patients. How patients experience these interventions has received less attention.
Objective: To better understand patients’ experience of intensive primary care, we interviewed patients receiving care from the Streamlined Unified Meaningfully Managed Interdisciplinary Team (SUMMIT), an ambulatory intensive care intervention at an urban federally qualified health center.
Methods: We interviewed 25 participants enrolled in the SUMMIT randomized controlled trial and conducted a Reflective Thematic Analysis using a hybrid inductive-deductive approach.
Results: Patients reported high levels of medical and social needs that outstripped prior levels of care and resources. They perceived multiple benefits of SUMMIT through the following themes: 1) Team-based care with improved access to services. Patients appreciated their medical and social needs being met, through higher-level, multidisciplinary care. 2) Caring relationships. Patients described the SUMMIT team as being like family and felt that team members had a genuine sense of duty and obligation toward them. 3) Overcoming stigma. Patients felt valued and treated with dignity. 4) Evolving self-efficacy. Over time, patients experienced increasing success, including engagement in care and improved health behaviors.
Conclusion: Patients perceived the SUMMIT team as better meeting their health-related needs, compared with traditional primary care. They spoke of the team as family and felt humanized and supported in overcoming barriers to engagement, which led to increased self-efficacy. Evaluations assessing the effectiveness of intensive primary care should measure potential patient-centered benefits beyond short-term utilization and cost reduction.
- Community-Based Participatory Research
- Doctor-Patient Relations
- Homelessness
- Integrated Health Care Systems
- Patient-Centered Care
- Primary Health Care
- Self Efficacy
- Social Support
- Vulnerable Populations
Introduction
Recognition of the fact that a relatively small number of medically and socially complex patients make up a disproportionate number of hospitalizations, emergency department (ED) visits, and share of health care costs, has prompted national efforts to address their needs.1 Many of these efforts have utilized intensive primary care interventions for patients with high utilization. Such interventions have often focused on patients’ social determinants of health (eg, poverty, health literacy, homelessness, food insecurity) that are thought to prevent effective use of “traditional” health care services (eg, attending appointments, completing recommended tests, and engaging in positive health behaviors).2,3 The promise of these interventions was captured in Atul Gawande’s New Yorker article describing the Camden Coalition’s “Hotspotting” program.4,5 These programs vary in intervention design, staffing, and populations served, but all are aimed at intensifying services for select patients in hopes of lowering utilization.
To date, most published studies on the impacts of intensive primary care interventions have had mixed, less-than-promising results.5⇓⇓⇓⇓–10 This raises concerns about whether these programs are a good use of health care resources.11,12 However, most of these evaluations have focused on the single aim of reducing utilization and costs. Intensive primary care programs may provide benefits not reported in these prior studies.13 Notably, few evaluations assess patients’ experience with intensive primary care, an important aspect of the “triple aim,” alongside improved health and lower cost. Several survey-based evaluations of Veteran’s Affairs (VA)-based intensive primary care for homeless veterans have shown improvements in multiple aspects of patient experiences,14,15 though other studies, and our own trial of an “ambulatory intensive care unit” (A-ICU) for medically complex patients experiencing homelessness reported mixed patient experience results.10,16,17 Quantitative measures of patient experience, however, may miss important impacts of these programs that can be elucidated by qualitative inquiry.14,18,19 As part of a randomized controlled trial, we interviewed patients receiving care from the Streamlined Unified Meaningfully Managed Interdisciplinary Team (SUMMIT), an A-ICU intervention for high-need, high-cost patients at an urban, health care-for-the-homeless, federally qualified health center (FQHC), to better understand patients’ experience with the intervention.
Method
Research Design and Participants
This study took place in a FQHC in Portland, Oregon, that serves over 5000 low-income patients with high rates of homelessness and substance use disorders (20.5% reporting alcohol use disorder, 24.8% reporting other use disorders). The SUMMIT A-ICU randomized, waitlist-controlled trial began in 2016 and enrolled participants through 2019.20 Eligible patients were referred from their existing primary care team and had 1 or more hospitalizations in the prior 6 months, with multiple medical or behavioral health conditions or poor engagement in usual primary care. After informed consent and completion of a detailed baseline survey, patients were randomized to either join SUMMIT immediately or be placed on a 6-month wait-list where they stayed with their existing care team before joining SUMMIT. During enrollment, we asked participants whether they would be interested in participating in interviews about their care experiences. Research team members purposefully sampled participants based on duration of time in the intervention to try and capture differences in care experiences throughout the study. Participants were compensated with a $10 gift card to a local grocery store or debit card. This study was approved by the Institutional Review Board at Oregon Health and Science University (OHSU IRB No. 15285).
Description of the SUMMIT A-ICU and Existing Care
The SUMMIT A-ICU is a colocated multi-disciplinary primary care team with reduced panel size (up to 150 patients vs 1000 patients in usual primary care provider [PCP] practice) and flexible scheduling. Staffing consisted of 2 internal medicine physicians (totaling 1 full-time equivalent) with board certification in addiction medicine, 1 complex care nurse, 2 care coordinators, 2 licensed clinical social workers, a pharmacist, team manager, and quality analyst. Clinical team members received didactic training in motivational interviewing, patient goal setting, and palliative care. Core activities included an initial comprehensive patient intake with medical and behavioral team members, patient-driven health goal setting, transitional care protocols when patients experienced hospitalizations, medication management assessment, weekly panel review, and case management to address social determinants of health and other unmet needs.
Patients were referred and transferred care to SUMMIT from their existing care team that consisted of a patient centered medical home (PCMH) model of primary care with access to services including mental health care (staffed by on-site psychiatric nurse practitioners for prescribing and social workers focused on counseling), substance use counseling (brief counseling and referral to treatment completed by certified alcohol and drug counselors), and pharmacy-led interventions (eg, diabetes medication therapy management). In addition, PCPs could refer patients to embedded community health workers (CHWs), who performed short-term (6-month) engagements.21,22
Data Collection
Members of the study team, including 2 experienced qualitative researchers (EH, BC), and a trained research assistant (AG), conducted interviews between 11/29/2017 and 12/30/2020. The interview guide (Appendix A) was designed to address the following overarching questions:
How did SUMMIT impact healthcare experience of participants?
What aspects of SUMMIT did patients find most useful or valuable?
Interviews were audio-recorded, transcribed verbatim, and transferred to Dedoose for analysis.23
Data Analysis
We conducted a Reflexive Thematic Analysis (RTA) of the data.24,25 RTA appreciates the active role researchers bring to the study of a phenomenon, where codes and themes are refined through iterative review and discussion of transcripts. We used a hybrid inductive/deductive approach,26 given that we had a priori theories for how SUMMIT functioned, and for interpretation of data based on the substance of the text. We identified codes at both semantic (ie, sentiments that were explicitly reported by participants) and latent (ie, implicit or inferred) levels. We used the Gelberg Behavioral Model for Vulnerable Populations27 to guide theme development for how predisposing factors intersect with intervention features to address patient needs and health behavior change. After reading each transcript and taking analytic notes, members of the research team (BC, EH, AG, and SE, a clinician-researcher with qualitative expertise) used an iterative process to develop a coding schema. At least 2 team members coded each transcript. The research team met regularly to discuss and resolve coding discrepancies and to identify thematic content. The coding team regularly shared preliminary themes and exemplars with the full study team, and continued to conduct and code additional interviews until thematic saturation was reached (defined as when no new codes or themes were identified). The full team discussed findings to finalize themes.
Results
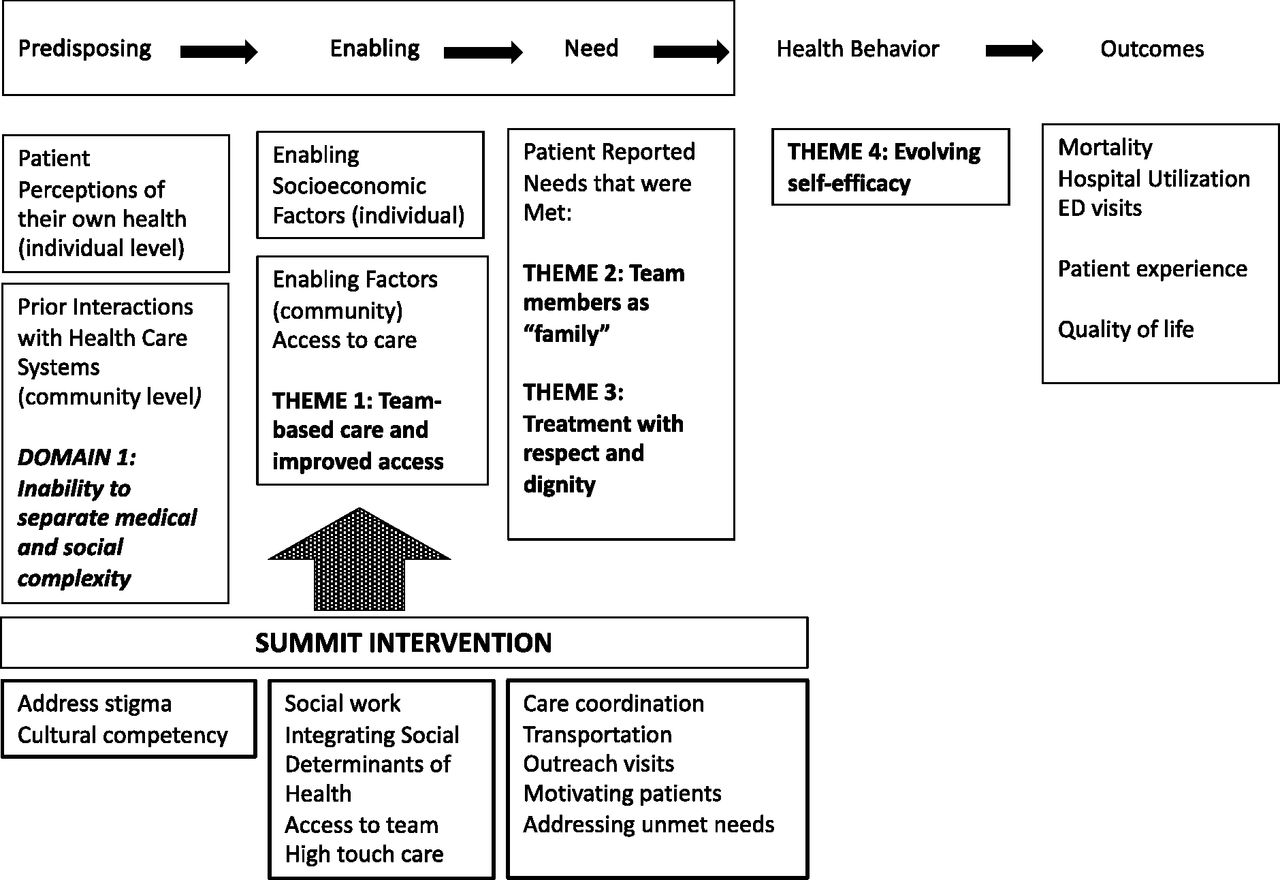
We conducted 25 interviews ranging from 20 to 80 minutes in length. Participants’ average age was 53 (S.D. 8.7) years, 40% self-identified as female, and 32% self-identified as Black, American Indian/Alaska Native, or Hispanic. Duration of SUMMIT enrollment was on average 14 months, with 3 participants interviewed before joining SUMMIT (Table 1). We organized results into 2 broad domains. In the first domain, “Patient Perspectives of Health and Health care,” we present a summary of patient descriptions of their own health and past interactions with the health care system to provide context for better understanding how patients experienced SUMMIT. In the second domain, “What the SUMMIT A-ICU provided,” we present 4 thematic categories describing what patients identified as the most helpful aspects of SUMMIT. (Figure 1 and Table 2)

Qualitative themes of the streamlined unified meaningfully managed interdisciplinary team (SUMMIT) A-icu impact using the Gelberg behavioral model for vulnerable populations framework.
Description of the Interviewed Sample
Description of Themes and Exemplars
Domain 1. Patient Perspectives of Their Own Health and Health Care
Theme 1. Inability to Separate Medical and Social Complexity
SUMMIT patients often reported that their health was poor, citing acute and chronic pain, mental health concerns, functional limitations, substance use, and traumatic experiences. Patients commonly reported pain stemming from injury or long-standing illness as a primary health concern. Patients also often reported multiple health concerns included infection, chronic illness, and cognitive impairments affecting memory and execution of daily tasks. Underlying conditions were sometimes discovered only when patients were hospitalized for other reasons.
“When I went to the hospital for withdrawal of alcohol and then they found out that I might have cancer and that my heart’s not working too good, and they also found that I had a fractured bone in my chest.” (48 yo Female, Pt 115)
Medical problems were compounded by the severe social isolation and poverty faced by many of these patients that contributed to difficulties achieving better health. Patients reported numerous challenges including housing insecurity, difficulty managing medications, food insecurity, and barriers to personal hygiene. There was often a feeling of shame (both explicitly expressed and inferred) in describing how these factors conspired with their health conditions to have cascading effects on the rest of their lives.
“I was in my addiction to alcohol … so I didn’t follow up on medical care, I didn’t go to appointments because … I was ashamed because I smelled like alcohol…” (48 yo Male, pt 119)
One patient told a story about how, after a heart attack and stroke, they found themselves in a nursing home with no ability to pay rent or other bills and subsequently lost their housing. Interwoven in patients’ accounts of their health conditions were stories of past and ongoing trauma stemming from abusive family dynamics, exposure to community violence, physical assaults, injury, and intimate partner violence.
2. What SUMMIT Provided
Theme 1. Patients Valued Team-Based Care with Improved Access to Needed Care
Patients recognized the increased resources available through the SUMMIT program. Patients interviewed after joining SUMMIT noted differences in the structure of SUMMIT compared with their prior primary care teams, and most appreciated the increased availability of multi-disciplinary staff, improved communication between and with their health care team members, and improved access to other aspects of care (eg, linkages to social needs referrals, medication changes, outreach visits).
“I liked the idea of having a whole team of people… I could see [the Social Worker] and she’s part of the Summit Team…I call the Summit Team and whoever answers [can] tell me what is going on … That’s helpful for me to call one number and get my questions answered and get my needs met … that’s something before I never really experienced a team concept with medical stuff… so I didn’t really know how nice it could be…and it does work and that reinforces me to enjoy it, to stay with it. (63 yo Male, Pt 106)
“[It] felt like [before SUMMIT] you were stuck in this quagmire of [being] a number … this team has all these new things, less patients… [there’s] pharmacists, a social worker that will help you, a medical assistant that’s there to correspond with.” (53 yo Female, Pt 118)”
Patients appreciated receiving a level of service they perceived as more than usual care.
“The (complex care nurse) brought. the [bowel prep]. to the house. She brought it with her, went through it with me… Didn’t just go, oh this is what it is, you know… And then they asked me questions about it, you know what I mean? Really went through it with me. [The SUMMIT team] actually really care.” (56 yo Female, Pt 108)
“I’ve even had a home visit. I mean nobody gets home visits anymore… it was real down to earth, [they] came to check on me because at that time I was in my bed and I couldn’t leave my bed.” (44 yo Male, Pt 101)
Patients also valued having more time for appointments and flexibility in scheduling them.
“They have more time for me. If I need an appointment that same day, they would be able to see me.” (29 yo Male, Pt 127)
Theme 2. Patients Perceived SUMMIT Team Members As Family
Many patients reported struggling with low levels of socials support, social isolation, and loneliness that hindered their health, and described feeling that the SUMMIT team held a personal commitment to them and their health. Patients developed positive relationships with SUMMIT team members and described them as de facto family who provided social and emotional support.
“They welcome my dog, they welcome me. They make me feel a part of the family and I have no family. This is all I got.” (59 yo Male, Pt 103)
“I just cling to the Summit team now more or less. They’re all integral in my life and I need people like that. I don’t have no friends.” (58 yo Male, Pt 105)
Patients reported feeling a sense of welcoming and “coming home” to a supportive environment that contributed to positive health care experiences.
“It’s the attitude. The aura around the people, you know. Sometimes I feel like I’m coming home, you know what I mean? I know there’s going to be a smiling face.” (56 yo Female, Pt 108)
Theme 3. Patients Felt Destigmatized and Treated with Respect and Dignity
Patients appreciated that in SUMMIT they were not punished for missed appointments or nonadherence. Multiple patients described how SUMMIT team members displayed nonjudgmental attitudes regarding their health care issues and provided additional support to patients when they had a setback.
“A lot of time though my depression gets in the way, so that will get me into times where I don’t want to take my medicine, but it’s always one of those things where we sit down and we talk about it. And they don’t yell at me. They don’t sit there and say oh you’re bad, you’re horrible because you did this. No, let’s just start over. Let’s figure out what we need to do… I’ve never had a doctor who was ever like that. “(44 yo Male, Pt 101)”
Patients reported that SUMMIT team members valued them as persons, treated them with dignity, and interacted with them in ways that provided hope and improved their sense of well-being.
“My health is better just by being treated better. not even medically treated, but just treated …more human like, they’ve improved my health not only physically, but emotionally.” (56 yo Female, Pt 108)
I think [SUMMIT] has gone to elite now, where for the people who feel disregarded from society, you put me back in society to where I’m happy.” (59 yo Male, Pt 103)
Theme 4. Patients Perceived Evolving Self-Efficacy through Engagement in SUMMIT
Patients described new health-related habits and routines that they directly attributed to SUMMIT, especially when it came to team members’ ability to motivate them and help with care coordination, transportation, and outreach activities.
They perceived involvement with SUMMIT as leading to a variety of successes, including more consistent appointment attendance, increased medication adherence, and improvements in interactions with outside health care systems or social services.
“I’ve gotten to the point where I’m not going to see [the SUMMIT team] for three weeks, which is a good sign that I’m managing on my own…I know enough what to do myself. I know to call if there’s a problem… they trust me now to deal with that.” (63 yo Male, Pt 106)
Responses reflected the impact of addressing structural barriers (ie, poverty, social determinants, transportation) in health care to facilitate self-efficacy.
“I used to get overwhelmed and frustrated with stuff and I would cancel appointments. I wouldn’t go to them. I might make them, but I wouldn’t go to them and that’s changed. If I got an appointment and it’s all done and she arranges the ride for me and everything, so all I have to do is show up. I can do that.” (69 yo Female, Pt 123)
Of note, not all patients thought their physical health improved because of involvement with SUMMIT. While appreciative of the team, patients did not always believe the program would lead to future improved health or physical functioning, citing severity of existing illness, or ongoing skepticism that their health could be improved through medical care.
“My mentality has improved, but my health is shot…But I do got the SUMMIT team and at least I can get some of my needs met in my last days, so I embrace the SUMMIT team.” (58 yo Male, Pt 105)
Discussion
We found that in the context of the SUMMIT A-ICU intervention trial10 for medically and socially complex patients with high rates of poverty and homelessness, patients noted several benefits of the SUMMIT high-touch, low-case load, tailored care-model compared with their previous primary care. Patients experienced higher levels of service and social support and felt less stigmatized and more valued. This support led to changes in behavior and self-efficacy. Our results suggest that intensive primary care interventions may have important benefits beyond the typically measured outcomes of short-term reductions in utilization and cost of care.
There is skepticism about the effectiveness of intensive primary care interventions, as many studies, including the parent trial for this study, have shown few or no reductions in utilization or health care costs.5,6,9⇓⇓–12,28⇓–30 Our analysis echoes what is increasingly being reported in other programs caring for high-needs high-cost patients: that the benefits of intensive primary care go beyond reducing costs and utilization and include improved access to and positive regard for their care team, and increased patient well-being, engagement in care, and positive health behavior change.19
Yet, results have also been mixed regarding intensive primary care impacts on measures of patient experience. For example, in our trial, improvements in Consumer Assessments of Health care Providers and Systems (CAHPS) scores were not significant, though we did see significant increases in patient reported well-being,10 which may reflect the “evolving self-efficacy” SUMMIT patients reported. Other intensive primary care evaluations have found similar mixed findings with positive impacts on relationship based measures of patient experience (ie, trust in clinicians), but no differences in other aspects of patient experience like those measured by CAHPS.16,17 A national study of the Homeless Patient Aligned Care Teams (H-PACT) for homeless veterans found improvements across multiple dimensions of patient experience, but interestingly noted that for highly-vulnerable enrollees, improvements in relationship-based measures of clinician-patient relationship and perception of cooperation among clinicians were most notable.15 Our patient interviews provide additional context on how intensive primary care interventions provide important benefits to patients and health systems and capture aspects of what patients experienced beyond commonly used measures such as CAHPS.
Our findings suggest the experiences patients valued most from SUMMIT were not directly related to traditionally measured aspects of patient experience (eg, care coordination, access), but were more aligned with the concept of relationship-centered care (RCC), a framework founded on 4 principles—1) personhood matters; 2) affect and emotion are important; 3) relationships are reciprocal; and 4) genuine relationships are morally valuable.31 Increasing patient self-efficacy and involvement in primary care, decreasing feelings of stigma, and improving provider trust are meaningful outcomes that are not frequently assessed in clinical trials—qualitative studies provide insight into these benefits,32 and future studies might assess these aspects of the patient experience as important measures of impact and effectiveness.
Acknowledging that reducing inappropriately high utilization and cost are important goals, our study provides insight into how the design of intensive primary care interventions might work to achieve this in the longer term. Patients reported that the support provided by SUMMIT led to a greater sense of well-being and higher self-efficacy, including less reliance on SUMMIT over time. This suggests that intensive primary care interventions may usher patients toward greater self-sufficiency and engagement in primary and preventive care, which might in turn lead to more appropriate and less costly patterns of utilization, and ultimately improved health. Our findings suggest that the path to these outcomes involves investing in multi-disciplinary teams, caring relationships, providing social support, addressing barriers to care, supporting behavior change, and preserving patients’ dignity and sense of self-worth.
Much of what patients reported as beneficial was the social support SUMMIT provided. Social support can be conceptualized as being financial, instrumental, informational, and emotional.33,34 SUMMIT and similar programs are designed to provide additional resources to enhance instrumental and informational support (eg, additional time for care coordination, patient education, arranging transportation, flexible scheduling), and patients did appreciate these features, which is not always the case, as noted in evaluation of the VA Patient Aligned Care Team program.35 However, our themes suggest that emotional support provided by SUMMIT was also important. A qualitative study of multiple intensive primary care interventions in Canada also found that patients, particularly those unable to access strong social support, appreciated the feeling of being cared for, an unanticipated finding that was perceived to be of great benefit.36 Interviews with patients in the Camden Coalitions “Hotspotting” intervention also describe the theme of “authentic healing relationships.”37 The structure of SUMMIT may allow for increased relationship building and trust, which in turn may have beneficial downstream health impacts, including increased patient-provider trust and adoption of positive health behaviors.38 Knowing 1’s care team and feeling known as a person can lead to improved engagement in care, and ultimately in health outcomes.39
Limitations
Our study was limited to 1 urban FQHC serving a very low-income population with high rates of homelessness and substance use. In addition, only patients with a recent hospitalization were included in the SUMMIT trial. Our findings therefore might not be generalizable to other populations with different levels of medical and social complexity.40 Second, patients in our study were referred to SUMMIT by PCPs at the FQHC, and their perspectives may be different from patients without previous active enrollment in primary care. Finally, our sampling strategy may be biased in that those who were more engaged in SUMMIT, or who had more positive experiences, may also have been more likely to participate in the interviews. Our findings may not reflect the perspectives of all SUMMIT participants.
Conclusion
Patients enrolled in the SUMMIT A-ICU intervention valued the additional resources and support they received; the holistic, team-based care and the improved access that SUMMIT provided; and the humanizing interactions with team members who were committed to their well-being, treated them with dignity, and promoted their self-efficacy. These impacts represent potential milestones on the path to improved health care utilization and outcomes and should be considered important patient-centered measures of intervention effectiveness in future evaluations of intensive primary care interventions.
Appendix
Appendix
Interview Guides
SUMMIT Patient Interview Guide:
Overall research questions:
To characterize the healthcare experiences of high-utilizer patients at a FQHC that serves homelessness, substance use, and mental illness
To identify from the patient’s perspectives factors that led to their current health condition/situation/high-utilization
To determine whether SUMMIT or Usual Care is meeting the needs of the patients referred to the program as intended
If not, why is it
To identify which components of SUMMIT or Usual Care that were most helpful for complex patients and why they were helpful
To identify care needs that SUMMIT or Usual Care do not address that may contribute to their utilization and complexity for future intervention improvements
Question(s):
I. To characterize the healthcare experiences of high-utilizer patients at a FQHC that serves homelessness, substance use, and mental illness
Tell us when and how you became a patient at Old Town Clinic
a. Prompt- can you remember who your primary care doctor(s) were before you came to old town?
What was your health care experience like prior to coming to Old Town Clinic?
a. Can you give an example of an interaction you had (hospitalization/ed visit) at that time?
Tell me about the last time you used the Emergency Room/Hospital
Tell me about the last time you went to a specialist’s office (or outpatient substance use program, other mental health program)
How has your experience with doctors and hospitals/emergency rooms been- can you give me an example?
II. To identify from the patient’s perspectives factors that led to their current health condition/situation/high-utilization
Tell me about a really tough day you had recently—what made it so tough?
How do you feel about your overall health? Do you feel you are complex?
Do you experience challenges or barriers to living a healthy life?
a. Prompts: lifestyle, social support, finances, mobility, transportation, chaos, substance use, mental health
Tell me what makes life so complicated for you?
What helps you to be healthy or well?
What does it mean to be healthy or well, in your opinion. Can you tell us a story of the last time you felt well?
III. To determine whether SUMMIT or Usual Care is meeting the needs of the patients referred to the program as intended
a. If not, why is it so?
Please tell me about what your experience has been like with members of your current care team
a. Who are the members of your care team?
Does your doctor and care team talk to you about your health that you can easily understand?
Do you feel that your provider and care team listen to your concerns when they make recommendations for your health care
Do you feel your care team is meeting your needs—why or why not?
a. Tell us a time when the team did meet your needs
b. Tell us a time when the team did not meet your needs
(If patient is new to SUMMIT or on Wait-list, else skip to VI.)
IV. To identify which components of Usual Care that were most helpful for HNHC/complex patients and why they were helpful
V. To identify care needs that Usual Care do not address that may contribute to their utilization and complexity
What has your experience with your care team been like? How are they different from your previous care teams (at other places)
What has been most valuable/helpful to you in your opinion
Can you tell us a story of how the team helped you with an issue
Do you think your health has improved after being involved in Old Town – why or why not?
Do you feel like your health needs are being met with your care team?
If there was anything you could do to improve your current care team, what would that be? Prompts: more case management, help with housing, employment, time to discuss medications, access to specialty referrals/doctors, transportation, healthy food education or access, substance use treatment, mental health
(If patient has been on SUMMIT)
VI. To identify which components of SUMMIT that were most helpful for HNHC/complex patients and why they were helpful
VII. To identify care needs that SUMMIT do not address that may contribute to their utilization and complexity (why aren’t needs being met)
What has your experience with the new SUMMIT team been like? How are they different from your previous care teams.
What has been most valuable to you in your opinion
Can you tell us a story of how the team helped you with an issue
Do you think your health has improved after being involved in SUMMIT/Old Town – why or why not?
Do you feel like your health needs are being met with your care team?
If there was anything you could do to improve your current care team (SUMMIT or Usual Care), what would that be?
Prompts: more case management, help with housing, employment, time to discuss medications, access to specialty referrals/doctors, transportation, healthy food education or access, substance use treatment, mental health
Notes
This article was externally peer reviewed.
This is the Ahead of Print version of the article.
Funding: National Institute on Drug Abuse (NIDA) K23053390-01A1 and Agency for Healthcare Research and Quality (AHRQ) K12HS022981-05 (Dr. Chan). VA Health Services Research & Development grant CDA 16-152 (Dr. Edwards).
Conflict of interest: The authors have no conflicts of interest to declare.
To see this article online, please go to: http://jabfm.org/content/00/00/000.full.
- Received for publication November 4, 2023.
- Revision received February 16, 2024.
- Accepted for publication March 11, 2024.




{kind=link}