
Abstract
Background: Advance care planning (ACP), a process of sharing one’s values and preferences for future medical treatments, can improve quality of life, reduce loved ones’ anxiety, and decrease unwanted medical utilization and costs. Despite benefits to patients and health care systems, ACP uptake often remains low, due partially to lack of knowledge and difficulty initiating discussions. Digital tools may help reduce these barriers to entry.
Methods: We retrospectively examined data from pilot deployment of Koda Health patient-facing ACP among Houston Methodist Coordinated Care patients, for quality improvement (QI) purposes. Patients referred by nurse navigators could access Koda’s digital platform, complete ACP, and share the legal documentation generated. Analyzed measures include usage rates and ACP-related decisions within the platform.
Results: Of eligible patients (n = 203), 52.7% voluntarily completed their plan. Engagement and completion rates were similar across demographics. Patients indicated majority preference (66.4%) toward spending the last days of life at home. Most patients indicated wanting no life-support intervention if quality of life became unacceptable (51 to 71% across 4 treatments). Life-support decisions were similar between demographic categories, excepting CPR and dialysis, wherein a greater portion of Black patients than White patients preferred at least trial intervention, rather than none.
Conclusions: As an observational QI analysis, limitations include bounded geographical reach and lack of data on ACP impacts to subsequent health care utilization, which future studies will address. Findings suggest that digital health tools like Koda can effectively facilitate equitable ACP access and may help support health systems and providers in offering comprehensive ACP.
- Accountable Care Organization
- Advance Care Planning
- Aging
- Health Equity
- Quality Improvement
- Retrospective Studies
Introduction
Advance care planning (ACP) is the process by which individuals of any age or health status learn, decide, and share their values, quality of life priorities, health goals, and future medical treatment preferences.1⇓–3 ACP has been shown to ensure patients’ preferences are fulfilled, decrease anxiety among loved ones, improve patient quality of life, decrease unwanted utilization, and increase hospice utilization when appropriate.4⇓⇓⇓–8 Further, studies have demonstrated health care savings ranging from $345811 to $22,43412 in the past 30 days of life, following discussion of ACP or documentation of those preferences.
Although many patients express interest in engaging in ACP, and up to 89% of patients believe that doctors should initiate ACP conversations, few patients take action to choose a surrogate decision maker (SDM), complete advance directives, or discuss their wishes with a loved one.4,14,15 Only 7% to 17% report having had an ACP conversation with their medical provider.16 The lack of engagement may be partially due to a justified lack of confidence in ACP, which is indeed often badly managed,17,18 with at least 23% to 46.6% of patients receiving medical treatment that is inconsistent with their preferences or goals.19,20 This lack of goal-concordant care leads to an estimated $75.7 billion to $101.2 billion spent on medical overtreatment or low-value care annually in the US.21 Medicare has recognized the problem, and a framework for reimbursement of high-quality ACP is now in place.22 However, the billing rate for Medicare beneficiaries is below 10% in most states.23⇓–25
ACP adoption is often even lower among historically marginalized communities – by a factor of 2 for African Americans.26⇓⇓⇓–30 Studies point toward the delivery of ACP dialog as a bottleneck: there is often a reluctance for patients to raise the topic to their primary care doctor.31 Physicians, in turn, cite time pressure32 and lack of training as impediments to initiating ACP discussions.31 Given these barriers, it is critical to understand how we can better support health systems and their providers in delivering ACP.33
Digital health tools may provide a means to reduce the number of barriers by providing a semistandardized conversation guide, facilitating document completion, and sharing care plans to inform loved ones and health care providers. Digital tools may also facilitate discussions with loved ones and reduce clinical burden to introduce this conversation and, whether a patient needs to begin the conversation or needs to update their preferences from an outdated directive. A recent review found that web-based ACP programs are associated with increased ACP knowledge, improved ACP communication with loved ones and health care providers, increased documentation, and are easy for participants to use.34 Further, prior research on video-guided ACP has shown improvements in documentation, increased hospice utilization, and decreased costs.11
This pilot retrospective analysis examined the feasibility and outcomes of deploying the Koda ACP software platform, built by digital health company Koda Health. The platform enables selection of health care goals, identification of life sustaining medical treatment preferences, and generation of legal documentation. The Koda platform aims to support health organizations and patients by easing the burden and encouraging informed ACP conversations. This retrospective review was conducted for quality improvement and health equity purposes to determine whether Koda facilitated ACP engagement to a greater and more equitable degree than commonly reported participation. We also describe specific ACP choices (eg, surrogate decision makers' relationship to patients, acceptable quality of life) for the respondents who completed these items and assess whether these selections differed between racial and socioeconomic categories.
Methods
For the purpose of quality improvement (QI), this retrospective observational analysis examined advance care planning, using utilization reports from the Koda Health digital ACP platform, with patients of Houston Methodist Coordinated Care (HMCC) Accountable Care Organization (ACO).
The Koda Health ACP platform is a web-application portal that provides patients with the tools to explore and define their ACP preferences. The platform can be accessed from any internet-connected device, including computers, phones, and tablets. The patient-facing Koda ACP platform is guided by a simple, easy to navigate interface that includes embedded videos with captions to provide evidence-based educational content to guide patients through the prompts. Patients first have the option to define their values, what they would consider unacceptable quality of life (eg, unable to dress themselves, in a coma, living in a nursing facility), and what is most important to them (eg, family, religion, hobbies). Users then learn about and select whether they would want to undergo different life support treatment options, in 2 different scenarios: in their current health state and if their quality of life became unacceptable. After writing in any additional preferences, patients can then identify at least 1 surrogate decision maker. The platform then auto-generates state-specific advance directives that can be signed or notarized electronically depending on state regulations. Patients are then able to share these documents with loved ones, as well as ensure that they are accessible in their referring health system’s electronic medical record (EMR). Users are able to make changes to their plan and send these updates to loved ones and health care providers at any time. Koda Health also employs trained, nonclinical advance care planning navigators to provide additional support for partner health systems and their patients. These navigators provide text, e-mail, and phone support to ensure patients can navigate the Koda ACP platform.
Houston Methodist Coordinated Care (HMCC) is an ACO participating in an Enhanced Track Medicare Shared Savings Program (MSSP) with approximately 50,800 Medicare fee-for-service patients attributed to more than 300 Primary Care physicians. Based on a predictive risk model,38 higher risk Medicare Shared Savings Program patients are stratified into HMCC nursing outreach programs, including Complex Care and Advanced Illness (AIC). For patients in these higher risk groups, HMCC nurse navigators conduct routine telephonic outreach to provide patient education and longitudinal health care navigation. In the time frame of data included in this analysis, 6097 patients were identified by HMCC risk stratification to be included in their nurse navigator outreach. HMCC nurse navigators were trained on introducing Koda Health ACP tools and introduced Koda to a subset of this population when appropriate (eg, if the patient had not completed ACP or were at higher health risk). If patients who were introduced expressed interest, they were referred to Koda. As this was a pilot of Koda as a service, nurses in the value-based care program did not intend to refer all contacted patients to Koda. Inclusion criteria included HMCC patients, age 18 or older, who had decision making capacity, and who were English-speaking, as the Koda platform was only available in English at the time. Patients with moderate to severe dementia, severe hearing loss, or blindness were excluded for these particular analyses. Nurse navigators only referred patients who did not already have advance directives on file.
Referred patients were sent a link to the Koda ACP platform and were able to access and complete the Koda ACP platform asynchronously on any internet-connected device (eg, smartphone, tablet, desktop computer). When patients were referred from HMCC, Koda navigators sent the patients initial information about ACP and the Koda platform. Koda Navigators would call or e-mail once a week if patients had not taken any action on the platform, if they had started but not completed their plan, or if they had any questions. If after 8 weeks, there was no response or further action taken by the patient, the navigator support team would end regular contact. Data were collected from November 2020 to April 2022 as part of standard utilization reports.
Measures and Materials
Patient information and ACP preferences were assessed with usage data within the Koda platform wherein patients selected their values, life circumstances, quality of life preferences, and their preferences for future medical treatments in different possible scenarios. Completion of ACP was defined as completion of each section of the Koda platform, with the exception of official documentation. Completion of executed documents required signing or notarization of advance directives based on state requirements.
Neighborhood-level socioeconomic status was assessed using the Area Deprivation Index (ADI),35 a validated measure which provides a rank from 1 to 100, with 1 indicating lowest level of disadvantage and 100 indicating highest level of disadvantage. Patients were assigned a national ADI ranking geocoded via US census data for each residential block in aggregate. Analyses were conducted with quintiles of ADI ranks.
We used descriptive statistics to assess the characteristics of the patient portal users and expressed them as central tendencies or frequencies with percentages. We used Chi-square tests to test for statistically significant distribution differences in categorical variables (race and ADI rank) for patients’ ACP platform choices. A Bonferroni correction was applied to adjust for multiple comparisons. For all inferential statistics, a p value < 0.05 was considered statistically significant. Analyses were performed using R version 4.2.36
Results
Over the 17-month data collection period, 203 patients were screened as eligible and enrolled into Koda Health ACP by the HMCC nursing team (see Figure 1). Enrolled patients were 75.5 (S.D. = 11.3) years of age on average, ranging from 30 to 102 years, 62.6% were Female and 37.4% Male. Based on ADI classification, 13.3% (27) were from the lowest SES, 22.2% (45) were from the lower-mid SES, 29.1% (59) were from the mid SES, 19.7% (40) are from the upper-mid SES, and 15.8% (32) are from the highest S.E. areas. See Table 1 for additional demographic characteristics.

Patient engagement and completion workflow.
Participant Demographic Characteristics (n = 203)
Of the enrolled patients, 60.1% (122) patients logged on to the Koda platform and took at least some action to begin planning for their care. Of those who did not participate, many were not able to be reached, already had ACP documentation prepared, were not interested at the time, or passed away. Of the 122 patients who logged in to the platform 87.7% (n = 107, 52.7% of total enrollees) completed the Koda ACP platform, and 62.3% (n = 76, 37.4% of enrollees) executed advance directive documentation.
Examining completion rates for participants identifying within the 2 main race categories in this data (n = 186), we found that 50% of Black (n = 30 of 60) and 56.4% of White patients (n = 71 of 126) completed advance care planning through the platform. Further, 38.3% of Black (n = 23) and 39.7% of White patients (n = 50) completed executed documents. Completion rates were also similar across ADI levels.
Patients who completed the Koda ACP platform and executed their documents, spent 40.9 minutes on average on Koda ACP platform, with Black patients spending 34.3 minutes on average and White spending 43.8 minutes on average. Koda ACP navigators, who provided support and guidance for enrolled patients, averaged 99.3 minutes per enrolled patient and 130.1 minute per patient who completed the ACP platform. The median time to ACP completion was 21.7 days and median time to execute documents was 52.3 days.
Of the patients who logged in to the platform, 91.0% (n = 111) identified a surrogate decision maker (SDM) and 45.1% (n = 55) shared their selected preferences with their SDM by e-mail via the platform. The relationship of SDMs to patients included: spouse/partner (n = 50, 45% of respondents), son/daughter (n = 39, 35.1%), sibling (n = 12, 35.1%), friend (n = 3, 2.7%), and other family, like nieces, nephews, or cousins (n = 7, 6.3%). The types of relationship between SDM and patient did not significantly differ between race or ADI rank.
Quality of Life Preferences
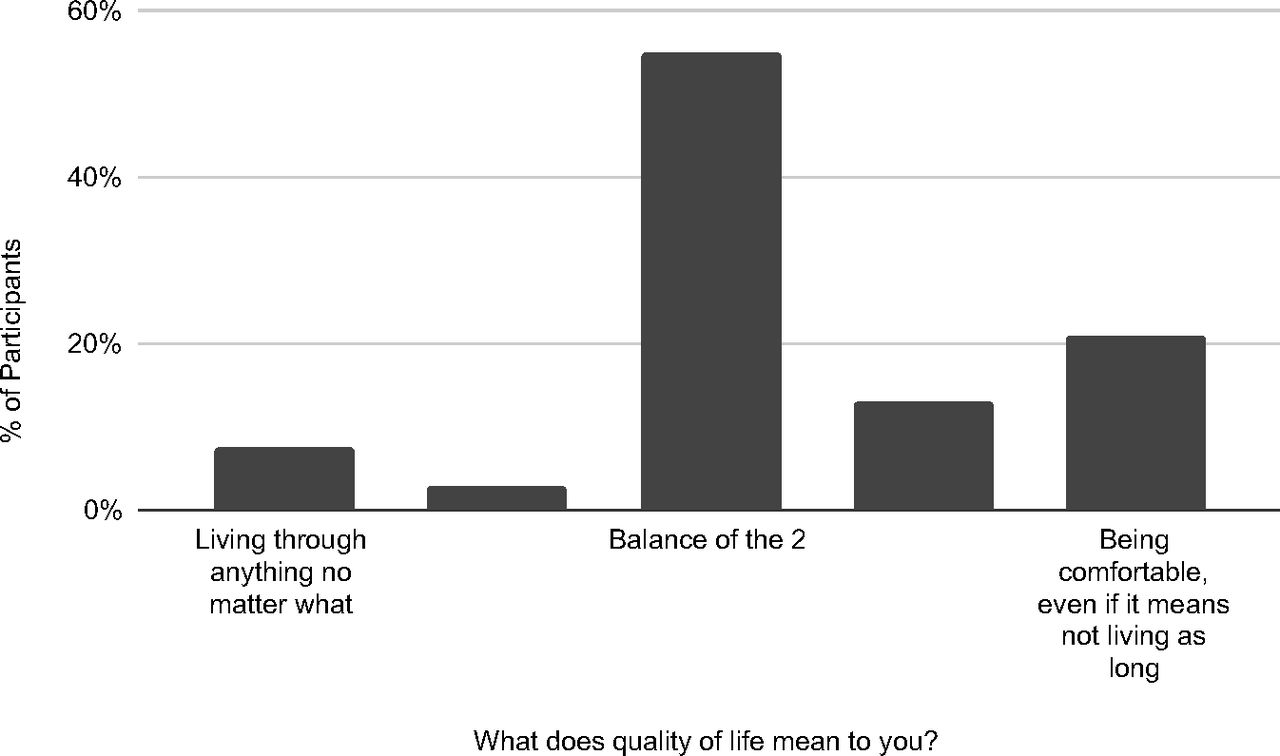
Patients were also asked to select their opinions on what they would prioritize in regard to quality of life and what would be unacceptable for them. In answer to “What does quality of life mean to you?” (see Figure 2), the majority of participants selected the option equidistant between “Living through anything, no matter what” (ie, having a longer life at all costs) and “Being comfortable, even if it means not living as long” (ie, prioritizing quality over length of life), indicating that most patients fall between these 2 extremes. This was not significantly different depending on race or ADI rank.

Percent of participants indicating their opinion on the spectrum of answers to the question “What does quality of life mean to you?” (n = 105 respondents).
Participants were asked to select which scenarios would severely impact their quality of life in a way that they would consider unacceptable (see Figure 3). The scenarios were related to ability to communicate, mobility, and independence. The responses to these items were not significantly different depending on race or ADI rank.

Number of participants’ indicating which circumstances would severely impact their quality of life in a way that they would consider unacceptable (n = 114 respondents, multi-select items).
In answer to the question “If you became very ill and only had a few hours or days to live, where would you want to spend them?”, the majority of participants selected “home” (n = 75, 66.4% of respondents), followed by hospital (n = 23, 20.4% of respondents) and care facility (n = 11, 9.7% of respondents), whereas 24 participants (21.2% of respondents) indicated that they were not sure. The location item options were multi-selectable, so some participants indicated more than 1 option. However, “home” was the most common single choice, with 60 participants selecting this as their only answer, out of the 113 who answered the question. Responses to these items did not significantly differ between race or ADI rank.
Life Support Medical Treatment Preferences
Patients were then asked about their preferences regarding the use of life-support treatments, including CPR, Mechanical Ventilation, Artificial Nutrition via Feeding Tubes, and Dialysis. Respondents answered whether they would/would not prefer each intervention under 2 types of circumstances: 1) if required in their current state of health and 2) if their quality of life became unacceptable. When asked about life-support interventions, more than half of all respondents indicated wanting limited or no intervention if they had an unacceptable quality of life. See Table 2 for the number and percentage chosen for each intervention.
Participants’ Koda ACP Platform Choices Regarding Common Life Support Treatments Under Two Possible Circumstances: Current State of Health and Unacceptable Quality of Life
There were no significant differences in the medical treatment preferences between SES, as measured by ADI ranking. Differences between Black and White patients were only seen with respect to CPR and dialysis. When asked about CPR preferences, there were significant differences between White and Black respondents, with 9.4% of Black patients vs 19.2% of White patients wanting no CPR at all, and 25% of Black patients vs 7% of White patients reporting “not sure,” if CPR were required in their current state of health. If quality of life became unacceptable, 37.5% of Black patients and 72.6% of White patients reported wanting no CPR. Similarly, if quality of life were unacceptable, 28.1% of Black patients and 65.8% of White patients would not want dialysis treatment.
Discussion
Our observational analysis demonstrates that the Koda digital platform may increase access to and engagement in ACP with more studies to follow. The Koda platform provided patients easy access to complete ACP within their own environment, with patient engagement rates from this pilot well above published ACP rate completion nationally from traditional processes. Of the eligible participants referred to Koda during this retrospective analysis, 60.1% took at least some action toward ACP and 52.7% completed the platform. Studies have indicated numerous barriers in the traditional ACP process, from initiating the conversation, documenting the preferences, and ensuring these preferences are known and followed when needed.18 Further, health care provider turnover and worsening staffing limitations in health care settings make the delivery of services like ACP much more difficult.37 Given the engagement seen in this retrospective review, tools such as Koda Health’s digital platform might help provide increased access to important ACP services by facilitating ACP decision, conversations, and documentation.
A key finding from this analysis is similar rates of ACP engagement and completion across race and SES demographics. Studies have previously demonstrated inequities in rates of ACP discussions and documentation among historically marginalized groups, notably among African Americans.26,28⇓–30 Accordingly, there has been an important focus from national organizations to understand how to promote equitable access to ACP. For sensitive conversations, such as end of life care planning, technology may provide a way to access these services and explore values without judgment or bias of a provider. Our analysis supports the position that digital tools might be effective at promoting equity in ACP.
Exploratory analyses of patients’ ACP selections observed in this sample showed that the majority of patients defined quality of life as being the midpoint between living through anything, no matter the pain and being comfortable, even if it means not living as long, indicating that they do not necessarily prioritize living at all costs nor comfort at all costs, but quality and quantity are equally important. Though not a validated measure of quality of life, this item is a starting point for patients to indicate what they value most for themselves. Patients also indicated a majority preference toward spending the last hours or days of life at home. These variables, as well as indications of which scenarios would impact quality of life in a way that they would consider unacceptable, were similar across race and SES categories.
When asked about life-support interventions, decisions on potential future life support treatments were also similar across demographic categories, with the exception of CPR and dialysis treatments, wherein a greater portion of Black patients than White patients indicated a preference for at least a trial medical intervention, as opposed to none at all. This finding is similar to a recent study of end-of-life care among Medicare beneficiaries.27 Across all participants, more than half selected wanting limited or no medical intervention if quality of life became unacceptable.
As this was an observational review of a quality improvement pilot, limitations of the current analysis include convenience sampling and a limited geographical reach. The HMCC nurse navigators referred patients who might benefit most – including if they did not already have advance directive documentation on file within the hospital system, but nurses’ unconsciousness reasoning for referring particular patients and not others may have introduced unconscious biases. Future research using more rigorous prospective case-control designs across larger populations and in different geographic regions would be informative in understanding the impact digital tools have on increasing ACP access. At the time of data collection, the Koda platform was only available in English, which may have limited the accessibility for some patients. The application is now fully available in Spanish as well, so improvements in accessibility will be tested subsequently. Future studies should also assess the use of digital ACP by patients with dementia and the unique factors that may be involved. Further, although this analysis measured the number of patients who shared their Koda plan with a surrogate decision maker (SDM) and the relationship of the SDM to the patient, we cannot speak to the understanding or motivations of the appointed decision makers. Studies focused on determining the impact digital tools have on patient and SDM understanding of ACP and patient-SDM alignment using digital tools would be important to ensure these tools are providing a valuable ACP experience. In addition, longer-term studies assessing the impact digital tools have on driving goal-concordant care and caregiver burden are vital in increasing more widespread adoption of these tools.
Overall, this work indicates that digital tools like Koda Health’s platform might be effective at increasing access to ACP to populations in an equitable manner. Given the challenges of administering ACP in traditional health care settings, health care systems should consider the use of technology and new tools to effectively engage their patients in ACP to improve quality of care.
Notes
This article was externally peer reviewed.
This is the Ahead of Print version of the article.
Conflict of interest: DM, RLR, KC, TF, SS, TH, CL, AC, and DH were each affiliated with Koda Health at the time of work on this project. ZM and JDA have no conflicts of interest to report.
Funding: None.
Data availability statement: De-identified data are available upon reasonable request. All requests for de-identified data should be made to the corresponding author, RLR.
To see this article online, please go to: http://jabfm.org/content/00/00/000.full.
- Received for publication April 4, 2023.
- Revision received June 26, 2023.
- Revision received July 6, 2023.
- Accepted for publication July 18, 2023.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.