
Article Figures & Data
Figures
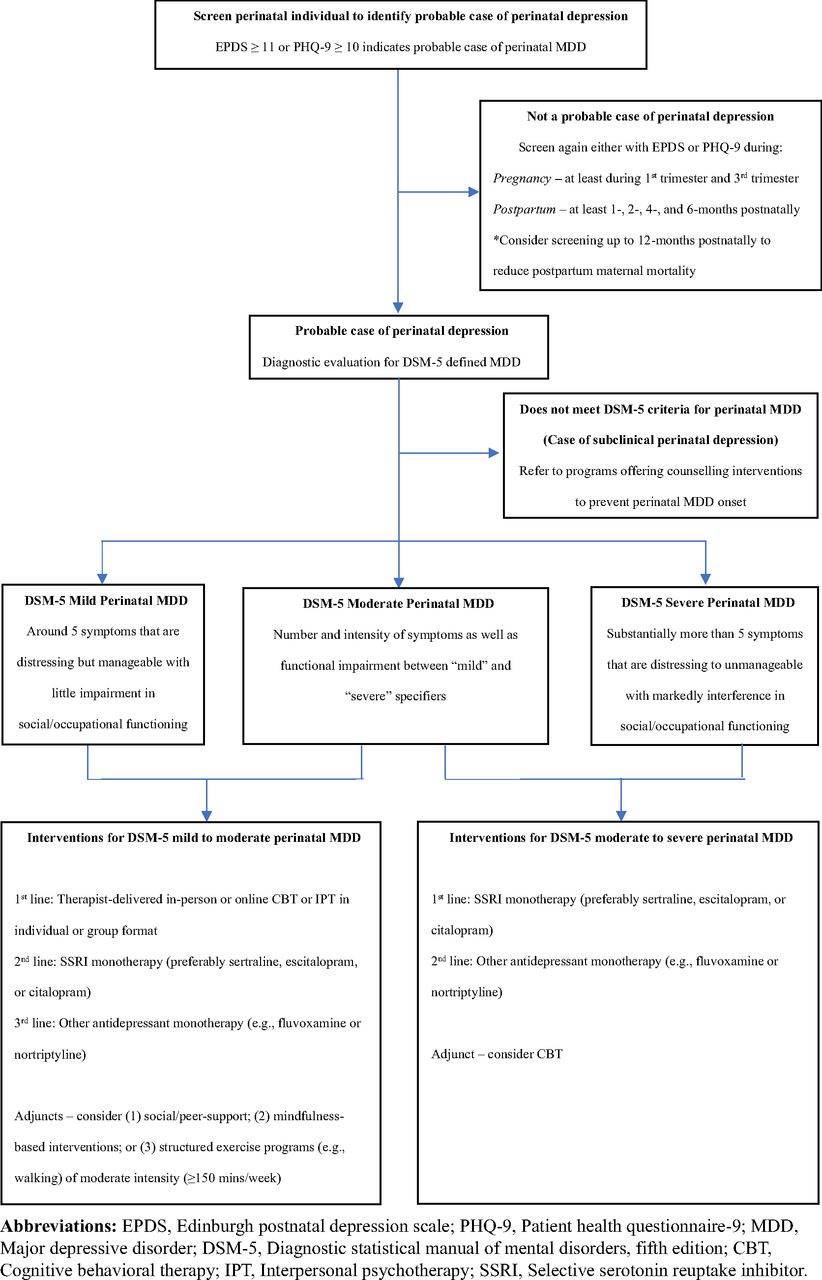
- Figure 1.
Suggested algorithm for detection and management of perinatal depression within primary care.

Tables
- Table 1.
Strength of Recommendation Taxonomy Criteria for Recommendations of Screening and Managing Perinatal Depression
Recommendations Evidence Rating Comments Recommendations for screening of perinatal depression Screen all perinatal individuals with EPDS or PHQ-9 to identify probable cases of perinatal depression B USPSTF guidelines gave a grade of “B” for the recommendation of screening all perinatal individuals for depression in primary care34 6 controlled studies (5 RCTs and 1 controlled trial) included in this systematic review demonstrates that screening programs were more effective than controlled interventions in reducing the absolute risk of developing depression later on in the perinatal period (Absolute Risk Reduction: 2.1% to 9.1%), but majority of these trials had low-quality study designs;39 NICE and AAP guidelines suggest that the PHQ-9 is a suitable instrument to investigate for perinatal depression41,50 Use an EPDS cut-off score ≥ 11 to screen for probable cases of major depressive disorder during the perinatal period B A recent meta-analysis of individual participant data (n = 58 studies; 15,557 participants) suggest that an EPDS cut-off score of ≥ 11 has the best combination of sensitivity (0.81–0.90) and specificity (0.83–0.88) for identifying perinatal major depression in reference to either a semi- or fully-structured diagnostic interview.42 A cut-off score ≥ 10 on the PHQ-9 can also be used to screen for probable cases of major depressive disorder during the perinatal period B One meta-analysis (n = 7 studies) suggests that a PHQ-9 cut-off score of ≥ 10 has a good level of sensitivity (0.84, 95%CI: 0.75–0.90) and specificity (0.81, 95%CI: 0.74–0.86) for identifying perinatal major depression in reference to a diagnostic interview51 Screen for antenatal depression in the first trimester and again in the third trimester C A consensus-based recommendation made by COPE guidelines; COPE recommends to screen for depression at the first antenatal visit (first trimester) and again either at or around 30 weeks gestation (third trimester)53 Screen for postpartum depression at 1-, 2-, 4-, and 6-months postnatally C Screening for PPD at 1-, 2-, 4-, and 6-months postnatally is a consensus-based recommendation made by the AAP guidelines41 Consider screening for postpartum depression up to 12-months postnatally to help reduce postnatal maternal mortality Screening for PPD up to 12-months postnatally is suggested based on the CDC identifying that a large proportion of maternal deaths postnatally occur between 6 to 12 months postpartum and mental health conditions are the leading cause of postnatal maternal mortality54 Recommendations for managing perinatal depression Therapist-delivered online or in-person CBT or IPT in individual or group format should be considered as a first-line intervention for perinatal depression of mild to moderate severity B Guidelines including USPSTF, CANMAT, COPE, and NICE supports therapist-delivered CBT and IPT as first-line interventions for PD of mild to moderate severity;34,50,53,67,68 One recent meta-analysis of RCTs indicated that psychotherapies are efficacious in reducing perinatal depressive symptoms (Hedge’s g = 0.67, 95%CI: 0.45–0.89; NNT: 4.4) and the results from most of the RCTs are consistent with the direction of the overall effect measure (25/43 RCTs), but a large proportion of these trials had low-quality study designs69 Social/peer-support, mindfulness-based interventions, and structured exercise programs with moderate intensity (≥150 minutes/week) can each be considered as a possible adjunct to therapist-delivered CBT/IPT or antidepressant monotherapy in the management of perinatal depression of mild to moderate severity B Despite each of these interventions described below receiving a SORT evidence rating of “B”, there is substantially more evidence examining therapist-delivered CBT/IPT and antidepressant monotherapy in the management of major depressive disorder. Therefore, these interventions should only be considered as adjuncts to therapist-delivered CBT/IPT or antidepressant monotherapy in the management of perinatal depression of mild to moderate severity. Social/peer support: Supported by COPE guidelines to use as an intervention for perinatal individuals with depressive symptoms;53 Although this meta-analysis of RCTs found that social/peer-support programs are efficacious in reducing perinatal depressive symptoms (SMD: −0.37, 95%CI: −0.66 to −0.08), the individual results from most of these RCTs are inconsistent with the direction of the overall effect measure (5/9 RCTs)80 Mindfulness-based intervention: Supported by CANMAT guidelines to use as an intervention for perinatal depression of mild to moderate severity;67 One meta-analysis of RCTs indicated that mindfulness-based interventions are efficacious in reducing depressive symptoms among perinatal individuals with mental health issues (SMD: −1.03, 95%CI: −1.48 to −0.58) and the individual results from most of these RCTs are consistent with the direction of the overall effect measure (7/9 RCTs), but some of these trials have low-quality study designs81 Structured exercise: Supported by CANMAT guidelines to use for managing perinatal depression of mild to moderate severity;67 Although this meta-analysis of RCTs demonstrated that structured exercise programs are efficacious in reducing perinatal depressive symptoms (SMD: −0.21, 95%CI: −0.31 to −0.11), the individual results from most of these RCTs are inconsistent with the direction of the overall effect measure (11/14 RCTs)82 Antenatal Depression: SSRI monotherapy should be considered as a first-line intervention for moderate to severe major depressive disorder C A consensus-based recommendation from multiple guidelines including CANMAT, COPE, and NICE;50,53,67,68 there are no existing RCTs testing SSRIs against placebo among depressed pregnant individuals. Postpartum Depression: SSRI monotherapy should be considered as a first-line intervention for moderate to severe major depressive disorder B Guidelines including CANMAT, COPE, and NICE support SSRI monotherapy as a first-line intervention for moderate to severe postpartum depression;50,53,67,68
A recent Cochrane review demonstrated that SSRIs are superior to placebo in improving depressive symptoms among postnatal individuals with a depressive disorder (SMD: −0.30, 95%CI: −0.55 to −0.05) after 5 to 12 weeks of treatment, but the certainty of the evidence is low83CBT can be considered as an adjunct after a clinical response to SSRI monotherapy in moderate to severe perinatal depression C A consensus-based recommendation from COPE guidelines; COPE recommends structured psychological interventions (e.g., CBT) as an adjunct once medications have taken effect in moderate to severe PD53 Abbreviations: EPDS, Edinburgh Postnatal Depression Scale; PHQ-9, Patient Health Questionnaire-9; USPSTF, United States Preventative Service Task Force; NICE, National Institute of Health and Care Excellence; AAP, American Academy of Pediatricians; COPE, Centre of Perinatal Excellence; CDC, Centers for Disease Control and Prevention; CBT, Cognitive Behavioral Therapy; IPT, Interpersonal Psychotherapy; RR, Risk ratio; NNT, Number needed to treat; RCTs, Randomized controlled trials; SMD, Standardized mean difference; SORT, Strength of Recommendation Taxonomy; CANMAT, Canadian Network for Mood and Anxiety Treatments; SSRIs, Selective serotonin reuptake inhibitors.
Outcome Class of antidepressants Magnitude of risk RCT Study Design Comparator Group of pregnant individuals with clinical indication for antidepressant use Statistical Adjustment for other potential confounds Congenital malformations SSRIs Relative risk ∼ 1.175 X X X Congenital cardiovascular malformations SSRIs Relative risk ∼ 1.2 to 1.375,76 X X X Spontaneous abortion – Relative risk ∼ 1.591 X X X Stillbirth – Relative risk ∼ 1.291 X X X Pre-eclampsia SSRIs Relative risk ∼ 1.492 X X X Mean gestational age at birth SSRIs Mean difference: −0.36 weeks94 (3 days earlier) X ✓ X Mean 5-minute APGAR score SSRIs Mean difference: −0.3294 (APGAR score of 0.3 less) X ✓ X Low birthweight – Relative risk ∼ 1.491 X ✓ X Preterm birth SSRIs Relative risk ∼ 1.612 X ✓ ✓ (Race/ethnicity, parity and gestational tobacco use) Postpartum hemorrhage SSRIs Relative risk ∼ 1.295 X X X Persistent pulmonary hypertension of newborn SSRI or SNRIs Relative risk ∼ 1.5 to 1.899,100 X X X Abbreviations: SSRIs, Selective serotonin reuptake inhibitors; SNRIs, Serotonin norepinephrine reuptake inhibitors; RCTs, Randomized controlled trials; Relative risk, risk ratio and/or odds ratio.
Notes: Risk refers to risk ratio or odds ratios from studies included in this review; Superscripts indicate citations describing the magnitude of the relative risk; A relative risk of two-fold or more (Risk ≥2.0) is generally accepted as being clinically significant at the level of an individual patient.36 The Symbol “X” refers to “No” and the symbol “✓” refers to “Yes”.
- Table 3.
Potential Adverse Events in Breastfed Infants Exposed to Selective Serotonin Reuptake Inhibitors During Lactation
Individual SSRI Prevalence Rate* Reported Adverse Events* Sertraline 2/280 cases (∼0.7%) Sleep myoclonus, agitation, restlessness, poor feeding, insomnia Paroxetine 2/228 cases (∼0.9%) Irritability, lethargy, poor weight gain, hypotonia Citalopram 6/112 cases (∼5.4%) Colic, decreased feeding, irritability/restlessness, sleep disturbances, hypo/hypertonia, irregular breathing Fluoxetine 11/280 cases (∼3.9%) Colic, seizures, irritability/restlessness, somnolence, lethargy, fever, unresponsiveness, watery stool, uncontrollable crying, vomiting, poor sleep Escitalopram 1/37 cases (∼2.7%) Necrotizing enterocolitis Fluvoxamine 1/18 cases (∼5.6%) Jaundice Abbreviation: SSRIs, Selective serotonin reuptake inhibitors.
*Data obtained from: Orsolini L, Bellantuono C. Serotonin reuptake inhibitors and breastfeeding: a systematic review. Hum Psychopharmacol. 2015;30(1):4-20. doi:10.1002/hup.2451.
Outcomes Magnitude of risk Maternal and Offspring Mortality Perinatal suicide Relative risk ∼ 2.29 Stillbirth Relative risk ∼ 1.510 Postnatal mortality of offspring Relative risk ∼ 1.97 Pregnancy and Delivery Complications Gestational hypertensive disorders Relative risk ∼ 1.35 Pre-eclampsia Relative risk ∼ 1.56 Pre-term birth Relative risk ∼ 1.4 to 2.412–16 Low birthweight Relative risk ∼ 1.7 to 2.014,15 Intrauterine growth restriction Relative risk ∼ 4.416 Head growth Mean difference: −0.08 mm/week17 Body growth Mean difference: −4.4g/week17 Low 5-minute APGAR score Relative risk ∼ 1.512 Postpartum Complications Infant malnutrition Relative risk ∼ 1.48 Infant physical illness Relative risk ∼ 1.7 to 2.67,8 Infant hospitalization Relative risk ∼ 1.47 Childhood maltreatment Relative risk ∼ 3.0116 Exclusively breastfeeding Relative risk ∼ 0.5-0.819,20 Partner depression Relative risk ∼ 1.2 to 1.726,27 Offspring depression Relative risk ∼ 1.724 Abbreviation: APGAR score, Apgar srtands for “Appearance, Pulse, Grimace, Activity, and Respiration.” In the test, these five things are used to check a baby’s health. Relative risk, risk ratio and/or odds ratio.
Notes: Superscripts indicate citations describing the magnitude of the relative risk; A relative risk of two-fold or more (Risk ≥2.0) is generally accepted as being clinically significant at the level of an individual patient.36
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.