
Abstract
With the passage of the MAT act (Mainstreaming Addiction Treatment) and the MATE Act (Medication Training and Expansion), the Drug Enforcement Agency “X-waiver” program governing the office-based prescription of buprenorphine for opioid use disorder has been immediately eliminated. The move was championed by vocal organizations with a rightful concern about buprenorphine access but was opposed by most physicians. Nonetheless, buprenorphine can now be prescribed like any schedule 3 medication. Studies show that despite rising opioid overdoses, buprenorphine prescription increases have been slow to rise and are particularly absent in rural communities. The elimination of the X-waiver may theoretically improve buprenorphine prescribing rates for opioid use disorder in rural areas, by nurse practitioners and physician assistants, and by resident physicians in teaching programs. It may also help decrease discrimination against individuals with opioid use disorder in postacute-care settings like nursing homes, physical rehabilitation centers, and in prisons and jails. Concerns include the elimination of the only focused opioid use disorder education many physicians receive (X-waiver courses) and a literature base showing that interest, rather than the X-waiver itself, remains the biggest barrier to recruiting more buprenorphine prescribers. Concerns also exist over the harms of precipitated withdrawal when buprenorphine is initiated inappropriately. The change of the elimination of the X-waiver brings about a new opportunity for Family Medicine and its parent organizations to champion the inclusion of opioid use disorder treatment within the chronic disease care models well-known to our integrated care settings.
The End of the X-waiver
The end of the X-waiver program has arrived. It happened suddenly, packed into an end-of-year spending bill addressing a host of mental health issues. The authors collectively represented here are all graduates of a single family medicine residency program that has demonstrated above-average outcomes in training physicians who go on to prescribe buprenorphine as medication for opioid use disorder (MOUD).1 Having scattered around the country since graduation, each has often found themselves on an island as one of the very few experienced MOUD prescribers among their peers. Frequently discussing cases, system challenges, and MOUD issues in both the literature and the news on a group messaging platform, the authors have collectively dubbed themselves the Bupe Troop. Now, more than ever, the time for the family medicine community at large to join the Bupe Troop has arrived.
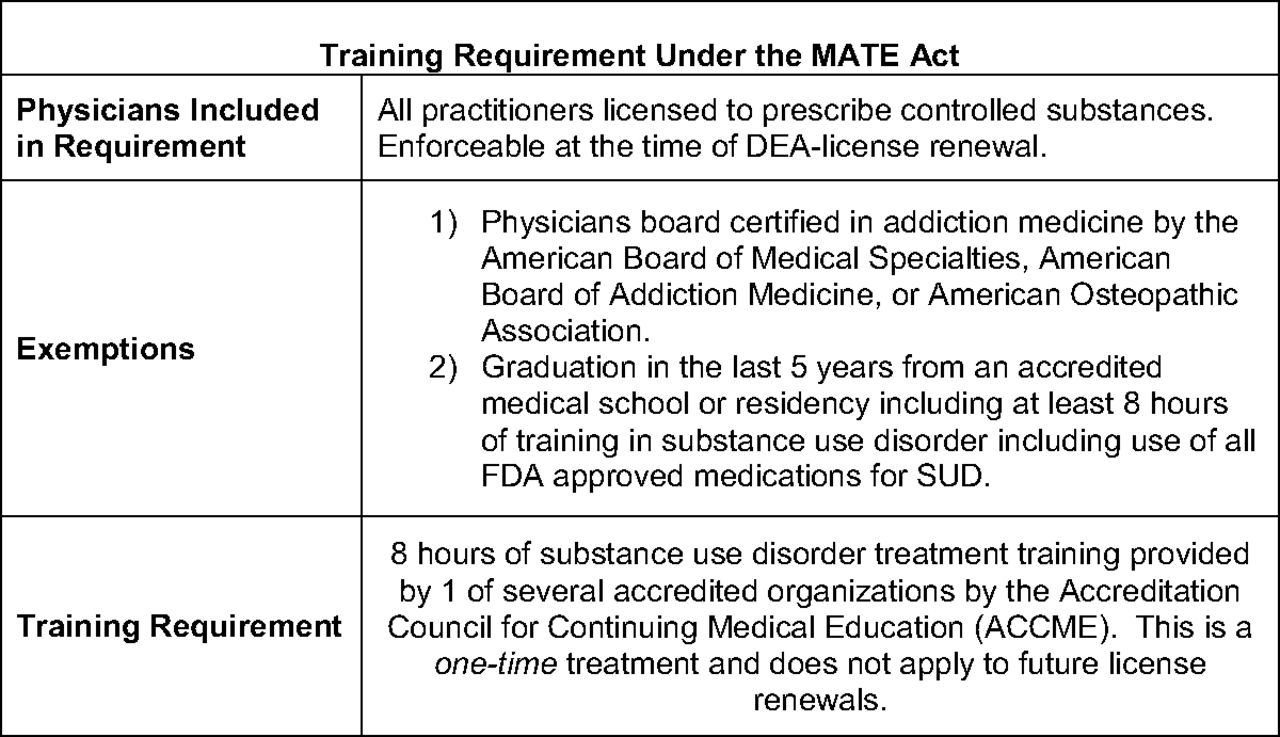
In the year 2000, the Drug Addiction Treatment Act (DATA 2000) bill was passed, introducing the “X-waiver” for the first time. Physicians were required to complete an official 8-hour training and submit a notice of intent application to the Drug Enforcement Agency (DEA) to prescribe buprenorphine as MOUD. A special “X” number on their DEA license had to be transmitted to pharmacies and detailed patient logs kept in preparation for the possibility of DEA audit. In the years 2000 to 2022, opioid overdose deaths continued to spike2 and incremental legislation chipped away at the task of expanding the buprenorphine workforce to address it (Table 1). At the end of 2022, 2 simultaneous bills were passed: the MAT act3 (Mainstreaming Addiction Treatment) and the MATE Act4 (Medication Training and Expansion). Clinicians holding X-waiver were mailed new DEA licenses in January of 2022 without X numbers. Buprenorphine can now be prescribed as MOUD by any clinician (physician, resident, NP, or PA) holding a DEA license with schedule 3 medication prescribing privileges. At the time of DEA license renewal, all clinicians will have to submit evidence of an 8-hour training in addiction medicine (Figure 1). Unlike the previous X-waiver qualifying trainings, the new license requirement is notably not specific to buprenorphine.

Training requirements for Drug Enforcement Agency (DEA) license renewal under the Medication Training and Expansion (MATE) act. Information from reference.4 Abbreviations: FDA, US food and drug administration; SUD, Substance use disorder.
Timeline of Buprenorphine as Medication for Opioid Use Disorder (MOUD) Regulatory Changes
The current state of buprenorphine prescribing certainly calls for change. Although 16% of psychiatrists (largely concentrated in urban areas) had received an X-waiver in 2015, only 2% of primary care physicians had.5 More than half of rural counties nationally still lack a single buprenorphine prescriber and 30% of all rural Americans live in a county with no buprenorphine access.6 Despite progressive relaxation in regulations (Table 1), expansions in the national volume of patients eligible for MOUD under waivered clinicians have largely been driven by those clinicians already possessing waivers applying for increases in their MOUD patient limits from 30 to 100 and 100 to 275 and not by expansions in the volume of newly waivered clinicians.7 A 2019 national survey of primary care clinicians found that only 20% had interest in treating OUD and 11% in obtaining an X-waiver, with only 38% expressing support for its elimination.8 Prior data has indicated that family physicians practicing in environments with more supportive mental health resources were more likely to be buprenorphine prescribers, but those in solo or rural practices were not.9 Despite these concerning trends, the single largest contributor to buprenorphine access in the years 2010 to 2018 still came from an expansion in the primary care MOUD workforce,10 mirroring declines in psychiatry-specialty prescriptions. Our collective views mirror the views of the physician community at large about these changes—through windows of excitement, apprehension, and opportunity.
Excitement
The elimination of the X-waiver has been a result of growing calls to action from patients and clinicians who see it as a step toward increased access. Removal of what many felt to be an unnecessary barrier to buprenorphine prescribing may encourage clinicians who may have otherwise hesitated to prescribe this “high risk” medication to take up providing MOUD. The elimination of limitations on the number of patients an individual clinician can treat for OUD will allow those clinicians already providing MOUD in higher-volume settings to care for even more patients in need. The removal of an onerous 24-hour training requirement for advanced practice providers may result in more primary care access particularly in rural communities. All emergency department physicians will also now be able to prescribe without a 3-day dispensing limitation, allowing for more acute-care starts and outpatient transitions. Importantly, residents will now be able to prescribe buprenorphine under the regulations of any other controlled substance including institutional DEA licenses, no longer reliant on an X-waivered faculty member to write prescriptions on their behalf. This may facilitate the expansion of residency-based MOUD prescribing. This alone is a critical change as residency training clinics are known to serve more vulnerable populations,11 and a prior study showed only 36.2% of family medicine residencies having a single X-waivered faculty member.12 Residents who are motivated to treat OUD will be able to educate themselves and provide this care during and after graduation even in the absence of motivated, educated faculty in their training programs.
Although expansion of buprenorphine access in community settings like primary care clinics and emergency departments is critical, it is not enough. We know that failure to offer MOUD in institutional settings such as jails, prisons, and skilled nursing facilities often leaves patients vulnerable to disrupted or inadequate care during critical periods of transition. Overdose is the leading cause of death for formerly incarcerated individuals with risks highest in the 2 weeks after release. There is strong evidence that risk can be mitigated by offering MOUD in jails and prisons; however, only a small proportion of correctional institutions nationwide offer buprenorphine or methadone.13 Similarly, hospitalized patients with OUD are disproportionately rejected from skilled nursing facilities, often because they are taking MOUD.14 Though the Department of Justice has clarified that blanket policies against provision of MOUD in correctional and skilled nursing facilities constitute a violation of the Americans with Disabilities Act,15 even efforts by State Attorney Generals to enforce antidiscrimination settlements have resulted in minimal or incremental progress.14 We are hopeful that elimination of the X-waiver will remove real and perceived barriers to the provision of buprenorphine in institutional settings and help patients get necessary, legally protected care for opioid use disorder.
Apprehension
Despite our enthusiasm for the elimination of the X-waiver and our strong interest in ensuring equitable and broad access to buprenorphine for treatment of OUD, we do have reservations that this step is not enough. Studies have shown time and again that physician interest in treating OUD is low across many specialties including Family Medicine and that hesitance to do so is unrelated to the barriers represented by the X-waiver’s required 8-hour training.8 The assumption that removal of the X-waiver will lead to an increase in physicians, NPs, and PAs prescribing buprenorphine is unfounded and not well-supported by the literature. Furthermore, federal policy changes like this do not remove state-level regulatory barriers to prescribing buprenorphine that vary across the country. A review from 2022 noted 10 states with additional buprenorphine laws or regulations16 including nonevidence-based counseling requirements.17,18
Furthermore, surveyed physicians report a lack of expertise and comfort related to addiction medicine broadly and buprenorphine specifically,19 likely related to the inadequacy of medical school and residency education around addiction medicine, which has likewise been well-documented elsewhere. By removing the requirement for 8 hours of training, which is focused on key concepts in addiction medicine in addition to the specifics of buprenorphine, we may have removed the only formal training in addiction medicine that many physicians would have otherwise received. For this any many other reasons, widespread stigma toward opioid use disorder will remain as a challenging barrier to overcome.
Finally, although buprenorphine is a remarkably safe medicine with exceptional efficacy,20 it does require some specific knowledge to ensure proper initiation. Giving buprenorphine at standard doses to a patient who has not yet reached mild to moderate withdrawal symptoms may lead to precipitated opioid withdrawal. Patients who are subjected to this unpleasant outcome are often unwilling to attempt induction of the medicine again in the future. This has become more complex in the era of fentanyl, which has made buprenorphine induction even more challenging with higher risks for precipitated withdrawal with conventional initiation regimens.21 We worry that uninformed clinicians could subject patients to harm without adequate training around the use of this medicine. Somewhat more complex “microdosing” or “macro-dosing” regimens may need to become standard of care. As of yet, these regimens are not traditionally taught even in existing waiver courses.
Opportunity
The X-waiver is X’ed, a moment that should call Family Medicine to action. Now more than ever, treatment of OUD can sit within the chronic disease care models known to family physicians without undue regulatory burden. We support 3 responses: maintenance and expansion of existing undergraduate and graduate medical education training in OUD management, continuing education for practicing Family Physicians and residency faculty, and widespread availability of real-time clinical support services.
In response to the previous DEA-mandated buprenorphine training requirements, some medical schools and family medicine residencies made buprenorphine training a required part of their curriculum.1,22 The 2022 ACGME Family Medicine Program Requirements update includes substance use disorder as a core curricular competency. Residency program surveys demonstrate significant work is needed to meet this training competency for opioid use disorder treatment: a minority of programs have specific training in buprenorphine management, and a lack of qualified preceptors was a commonly cited barrier.12,23 Although X-waiver elimination will not fully remove these barriers, it will afford new opportunities for creative and longitudinally integrated training in buprenorphine management. Undergraduate and graduate medical educators should use this change to deepen, not trim, required training in SUD and buprenorphine management.
Practicing Family Physicians are acutely aware that patients with a need for buprenorphine initiation or continuation are already in their examination rooms. Faculty know their trainees encounter patients with treated and untreated OUD. As with the treatment of any condition, the complexity of OUD cases and buprenorphine treatment varies, as does the comfort and experience of any individual Family Physician. The AAFP should lead by providing a focused and up-to-date buprenorphine training course that will meet the 8-hour CME requirement for treatment of patients with substance use disorder that is newly required for DEA license renewal beginning June 2023, as well as with shorter on-demand courses and “just-in-time” educational resources.
In their daily practice, Family Physicians will encounter complex OUD cases in real time. Although informal networks such as our Bupe Troop are invaluable, more systemic support is urgently needed. Even after waiver training, physicians face systemic barriers, specifically time restraints and lack of staff and leadership support, to prescribing that result in most newly trained physicians not subsequently prescribing buprenorphine.24 State-wide programs such as the Massachusetts Consultation Service for Treatment of Addiction and Pain (MCSTAP) and the National Substance Use Warmline provide real-time phone consultation with experts to guide practicing clinicians dealing with challenging cases.25,26 Health systems have successfully implemented similar internal clinical support services.27 These models should be expanded in reach and depth, with a focus on rural and underserved areas, and for physicians new to the prescription of buprenorphine navigating initial or complex patient cases. This could take the form of clinical preceptorships or mentoring opportunities for experienced clinicians to support those newer to MOUD work. The AAFP should advocate for health-systems-level-support that enables physicians and the teams they work in to manage buprenorphine safely and effectively. Family Medicine has an opportunity to lead by showing that our specialty’s commitment to high-quality and comprehensive health care across the lifespan includes widely available and appropriately supported medication treatment of OUD within our patients’ trusted family care home.
Notes
This article was externally peer reviewed.
This is the Ahead of Print version of the article.
Funding: None.
Conflict of interest: All authors report no relevant conflicts of interest. Dr. LeFevre reports consulting for the Missouri Department of Mental Health as a treatment consultant through the State Opioid Response grant.
To see this article online, please go to: http://jabfm.org/content/00/00/000.full.
- Received for publication February 12, 2023.
- Revision received May 19, 2023.
- Accepted for publication May 25, 2023.




{kind=link}