
Article Figures & Data
Figures
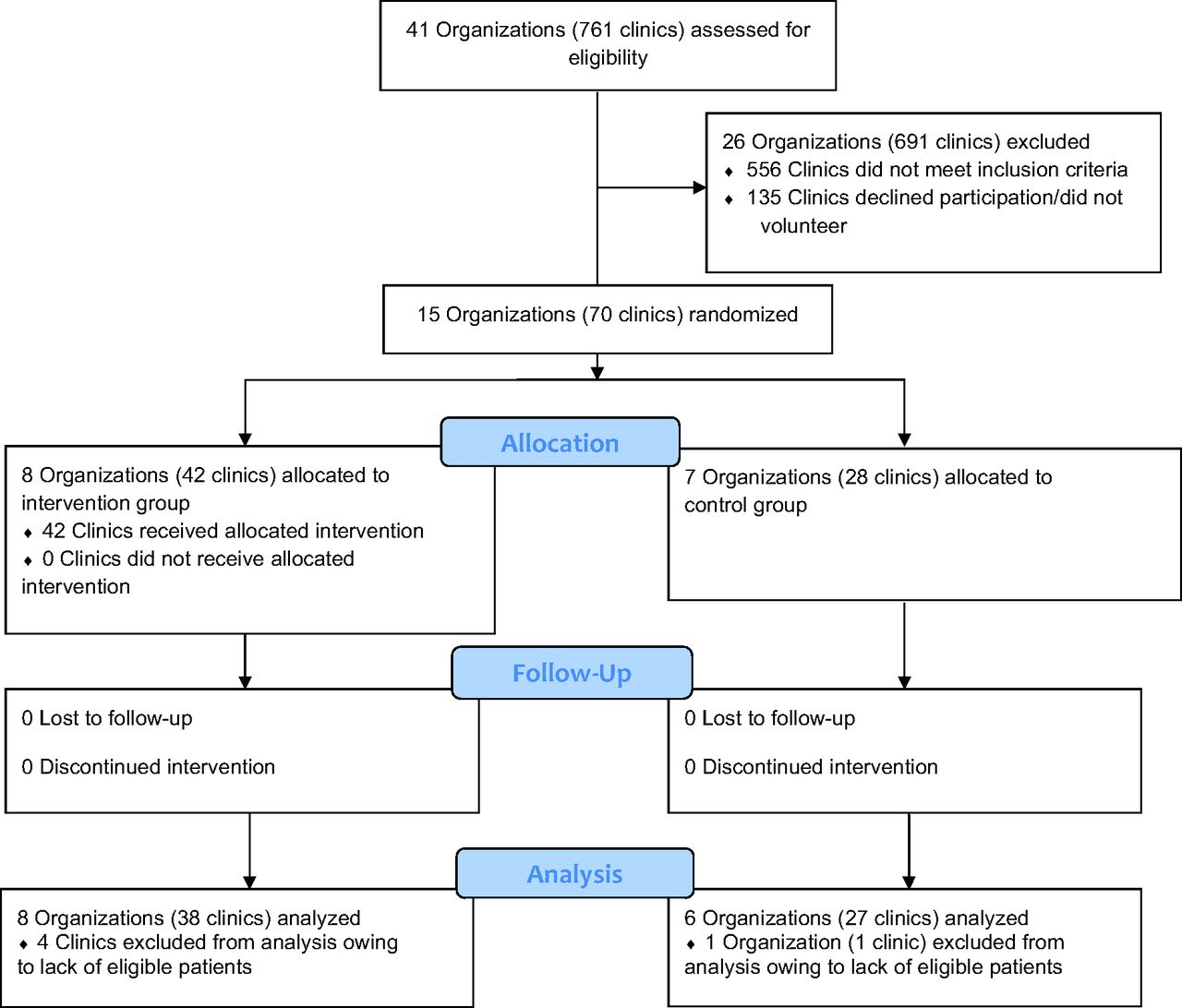
- Figure 1.
CV Wizard CONSORT flow diagram.
- Figure 2.
Predicted probability of receiving a prescription for recommended medication. Abbreviation: CDS, Clinical decision support.


Tables
- Table 1.
Encounters with a Recommendation to Start a Hypertension, Diabetes, Statin, or Tobacco Cessation Medication Stratified by Those Where a Prescription Was versus Was Not Written Within 1 Week of Encounter
All CDS-Eligible Encounters (n = 106,769) Intervention CDS Eligible Encounters (n = 61,219) Control CDS Eligible Encounters (n = 45,550) p-Value Encounter Risk Avg. Reversible Risk (SD) 10.4 (10.3) 9.7 (10.2) 11.3 (10.5) <0.001 Avg. 10-Year ASCVD Risk (SD) 17.2 (12.8) 16.5 (12.5) 18.1 (13.0) <0.001 Average Age at Encounter (SD) 58.5 (8.8) 58.0 (8.8) 59.2 (8.7) <0.001 Avg # Visits During Study (SD) 7.1 (6.2) 11.1 (9.8) 10.5 (8.7) <0.001 Gender <0.001 Woman 56,388 (52.2%) 33,232 (54.3%) 23,156 (50.8%) Ethnicity <0.001 Hispanic 27,269 (25.5%) 19,615 (32.0%) 7654 (16.8%) Non-Hispanic 75,680 (70.9%) 38,854 (63.5%) 36,826 (80.9%) Unknown Ethnicity 3820 (3.6%) 2750 (4.5%) 7654 (16.8%) Race <0.001 Asian 4262 (4.0%) 2721 (4.4%) 1541 (3.4%) Black 21,056 (19.7%) 13,002 (21.2%) 8054 (17.7%) Other* 3110 (2.9%) 2026 (3.3%) 1084 (2.4%) White 70,151 (65.7%) 36,810 (60.1%) 33,341 (73.2%) Unknown 8190 (7.7%) 6660 (10.9%) 1530 (3.4%) Insurance at Encounter <0.001 Medicaid 36,451 (34.1%) 22,543 (36.8%) 13,908 (30.5%) Medicare 37,270 (34.9%) 19,311 (31.5%) 17,959 (39.4%) Other Public 3175 (3.0%) 2771 (4.5%) 404 (0.9%) Private 14,097 (13.2%) 6768 (11.1%) 7329 (16.1%) Uninsured 15,776 (14.8%) 9826 (16.1%) 5950 (13.1%) FPL at Encounter <0.001 <138% 56,554 (53.0%) 38,051 (62.2%) 18,503 (40.6%) ≥138% 18,079 (16.9%) 12,287 (20.1%) 5792 (12.7%) Missing 32,136 (30.1%) 10,881 (17.8%) 21,255 (46.7%) Avg Appt Length (mins) <0.001 5 to 15 minutes 18,943 (17.7%) 12,851 (21.0%) 6092 (13.4%) ≥20 minutes 87,508 (82.0%) 48,086 (78.6%) 39,422 (86.6%) Missing 318 (0.3%) 282 (0.5%) 36 (0.1%) Avg Time Behind Schedule (mins) 0.272 ≤10 minutes 81,166 (76.0%) 46,463 (75.9%) 34,703 (76.2%) Abbreviations: CDS, Clinical decision support; SD, Standard deviation; FPL, Federal poverty level; ASCVD, Atherosclerotic cardiovascular disease.
*Other race includes American Indian, Alaska Native, Native Hawaiian, Pacific Islander, those who selected more than one race, and all other race.
- Table 2.
Encounters with a Recommendation to Start a Hypertension, Diabetes, Statin, or Tobacco Cessation Medication Stratified by Those Where a Prescription Was versus Was Not Written Within 1 Week of Encounter
All Encounters with a Recommendation (n = 106,769) Recommendations with a Prescription Within 1 Week (n = 35,078) Recommendations with No Prescription Within 1 Week (n = 71,691) p-Value Group <0.001 Intervention - CDS Used 15.2 16.2 14.7 Intervention - CDS Not Used 42.2 41.2 42.6 Control 42.7 42.6 42.7 Encounter Risk Avg. Reversible Risk (SD) 10.4 (10.3) 11.5 (11.4) 9.8 (9.7) <0.001 Avg. 10-Year ASCVD Risk (SD) 17.2 (12.8) 17.9 (13.4) 16.8 (12.4) <0.001 Avg. Age at Encounter, years (SD) 58.5 (8.8) 57.9 (8.7) 58.8 (8.8) <0.001 Avg. No. Visits During Study (SD) 7.1 (6.2) 7.1 (5.8) 7.1 (6.3) <0.001 Gender <0.001 Woman 52.2 51.3 53.6 Ethnicity <0.001 Hispanic 25.5 30.4 23.2 Non-Hispanic 70.9 66.2 73.2 Unknown Ethnicity 3.6 3.4 3.7 Race <0.001 Asian 4.0 4.4 3.8 Black 19.7 23.6 17.8 Other* 2.9 2.6 3.1 White 65.7 61.2 67.9 Unknown 7.7 8.2 7.4 Insurance at Encounter <0.001 Medicaid 34.1 33.5 34.5 Medicare 34.9 29.3 37.7 Other Public 3.0 3.5 2.7 Private 13.2 13.4 13.1 Uninsured 14.8 20.3 12.1 FPL at Encounter <0.001 <138% 53.0 55.1 51.9 ≥138% 16.9 16.8 17.0 Missing 30.1 28.2 31.0 Avg Appt Length (mins) <0.001 5 to 15 minutes 17.7 17.4 17.9 ≥20 minutes 82.0 82.2 81.9 Missing 0.3 0.4 0.2 Avg Time Behind Schedule (mins) 0.024 ≤10 minutes 76.0 75.6 76.2 >10 minutes 24.0 24.4 23.8 Abbreviations: CDS, Clinical decision support; SD, Standard deviation; FPL, Federal poverty level; ASCVD, Atherosclerotic cardiovascular disease.
*Other race includes American Indian, Alaska Native, Native Hawaiian, Pacific Islander, those who selected more than one race, and all other race.
- Table 3.
Unadjusted Frequency of Provider Action Taken Related to Encounters in Which CDS Recommended New Medication
Intervention Clinic Encs, Tool Used (CDS+) Intervention Clinic Encs, Tool Not Used (CDS-) Control Clinic Encs (CDSc) BP Meds (n = 6820) (n = 18,265) (n = 23,267) Any BP Rx Recommendation 34.9 32.7 33.7 Recommendation High Priority (1 to 2) 40.4 37.1 37.4 Recommendation Low Priority (3 to 6) 26.1 24.6 25.7 Between rec p-value <0.001 <0.001 <0.001 Diabetes (DM) Meds (n = 1354) (n = 3951) (n = 2994) Any DM Rx Recommendation 36.0 34.5 32.9 Recommendation High Priority (1 to 2) 45.5 44.8 43.9 Recommendation Low Priority (3 to 6) 23.5 18.5 20.6 Between rec p-value <0.001 <0.001 <0.001 Dyslipidemia Meds (n = 4383) (n = 10,186) (n = 12,704) Any Dyslipidemia Rx Recommendation 10.3 6.6 6.5 Recommendation High Priority (1 to 2) 11.6 6.9 6.6 Recommendation Low Priority (3 to 6) 17.0 14.6 14.2 Between rec p-value 0.140 <0.001 <0.001 Tobacco Cessation Meds (n = 3006) (n = 7110) (n = 9543) Any Tobacco Cessation Rx Recommendation 9.1 6.9 6.7 Priority 1 9.4 7.0 6.8 Priority 2 6.3 6.0 5.9 Abbreviations: CDS, Clinical decision support; BP, Blood pressure.
Notes: N = count of encounters for patients with a recommendation to start a medication who were not prescribed any type of that medication in the past 6 months. Two-tailed, unpaired t test with significance level set at 0.05 assuming unequal variances.




{kind=link}
{kind=link}