
Abstract
Background: Declining COVID-19 vaccination rates have led to implementation of monetary incentives to increase vaccine uptake. The Ohio Vax-a-Million lottery and subsequent $100 incentives were created to encourage individuals to become vaccinated. The purpose of this survey was to determine the efficacy of these monetary incentives on vaccination rates.
Methods: A 38-item questionnaire was given to outpatients at MetroHealth and Cleveland Veteran Affairs Hospitals between August 2021 and February 2022 who either waited 2 or more months to receive the COVID-19 vaccination or have not yet been vaccinated. The survey contained questions regarding demographics and perceptions of COVID-19 monetary incentives on vaccination likelihood.
Results: Of the 471 participants surveyed, 0.95% reported that the Ohio Vax-a-Million lottery increased their vaccination likelihood, while 29.7% reported that it decreased their likelihood. 6.8% of respondents reported the $100 incentive increased their vaccination likelihood while 17.4% reported it decreased their vaccination chances. 20.6% of participants stated news of the Delta (δ) variant increased their vaccination likelihood.
Conclusion: Our study results suggest that monetary incentives were not associated with increased COVID-19 vaccination rates. Instead, more participants believed that these incentives decreased their vaccination likelihood. Expansion of the survey across a wider sociodemographic range can provide further evidence of the efficacy of these programs before reimplementation.
- COVID-19
- Health Policy
- Monetary Incentives
- Ohio
- Qualitative Research
- Surveys and Questionnaires
- Vaccination Hesitancy
Introduction
Suboptimal COVID-19 vaccination rates have led policy makers to implement incentive systems. On May 12, 2021, the state of Ohio created the Vax-a-Million lottery, offering COVID-19 vaccinated individuals an opportunity to win $1 million or college tuition scholarships1. Recent studies using administrative data and simulation models report conflicting results regarding the efficacy of the lottery on increasing vaccination rates2,3. Given continued investment in financial incentives despite inconsistent findings, there is an urgent need determine their efficacy among persons both vaccinated and unvaccinated.
Studies of financial incentives in the context of other diseases have shown mixed results. Patel et al found that financial incentives to physical activity were only effective when framed as a loss incentive (eg, losing money when certain goals are not achieved), rather than using a gain or lottery incentive5. Reviewed evidence suggests that financial incentives to undergo influenza and pneumococcal vaccination are effective when targeted at patients or clinicians6. A comparative effectiveness study of use of an educational brochure versus a lottery type incentive found that both strategies were similarly effective7.
Following the perceived success of the lottery, Ohio began offering $100 gift cards to vaccinated enrollees of Ohio Medicaid and MyCare8. We directly assessed the impact of COVID-19 vaccination initiatives by asking Northeast Ohio residents about the influence of these financial incentives on vaccination likelihood.
Methods
A 38-item written questionnaire was administered to English-speaking medical outpatients in Cuyahoga County between August 2021 and February 2022. Participants were recruited at the MetroHealth System (95.3%) and the Cleveland Veterans Affairs Hospital (4.7%). Participants were eligible if they had either delayed initial COVID-19 vaccination by at least 2 months following vaccine eligibility or were not yet vaccinated. Vaccination status was self-reported and confirmed in the electronic health record. Patients were recruited during their visits to their primary care and rheumatology providers. Surveys were administered in person by members of the study team. The survey contained questions regarding demographics, COVID-19 vaccination intention, and any influence of 1) emerging viral variants 2) financial incentives on COVID-19 vaccination decisions. Human subject approval was obtained from the MetroHealth System and Cleveland Veterans Affairs Hospital. All data were entered and managed in REDCap, hosted by the MetroHealth System9. Statistical analyses (Pearson chi-sqaure tests) were performed comparing vaccination likelihood and financial incentives using SPSS version 28. Comparisons were re-estimated including “not applicable” responses as a nominal category and treating indicators as ordinal (Somer’s d) and results of these analyses were nearly identical.
Results
The median age of participants was 51. The majority of patients were female (74.9%) and 56.2% had some college education or higher (Table 1). The racial and ethnic diversity of the sample mirrors that of the participating health systems in that racial and ethnic minorities (specifically African Americans and Hispanics) are slightly overrepresented relative the population distribution in Northeast Ohio. Most of the study population was unvaccinated (60.7%), while 39.3% of participants delayed vaccination for at least 2 months following vaccine eligibility. Of the 518 patients who were approached, 471 (90.9%) agreed to participate in the survey.
Demographics
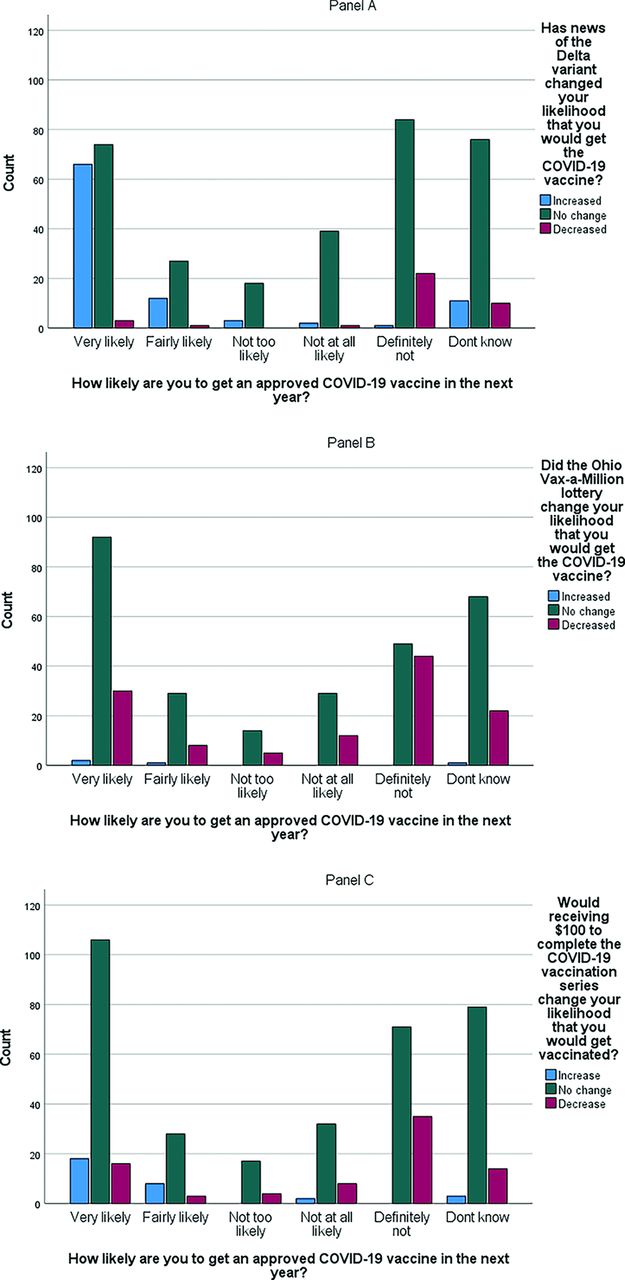
For 20.6% of respondents, news of the δ variant increased their vaccination likelihood. For the majority of participants reporting this increase, they stated they were already likely to become vaccinated (Figure 1 Panel A). News of the δ variant increased vaccination likelihood among those who delayed vaccination compared with unvaccinated (36.0% vs 11.6%, P < .001).

Comparison of 3 factors associated with likelihood of getting an approved dose of COVID-19 vaccine next year. A. Reported change in COVID-19 vaccination likelihood after news of the Delta variant by current vaccination likelihood. Chi-square=20.8, df 10, p=0.022; N=450, accounting for 21 not applicable/missing responses. B. Reported change in COVID-19 vaccination likelihood following implementation of the Vax-a-Million lottery by current vaccination likelihood. Chi-square=119.3, df 10, p<0.001. N=406, accounting for 65 not applicable/missing responses. C. The bar graphs represent changes in vaccination likelihood following implementation of $100 incentives, stratified by current vaccination likelihood. Chi-square=49.7, df 10, p<0.001. N=444, accounting for 27 not applicable/missing responses.
Just 0.8% of respondents reported that the Vax-a-Million lottery increased vaccination intention, while 26.5% reported the lottery decreased their chances (Figure 1 Panel B). A higher proportion of unvaccinated participants than those who delayed vaccination stated the lottery decreased their vaccination likelihood (38.1% vs 15.0%, P < .001).
The $100 incentive increased vaccination likelihood in 6.8% of respondents while 17.4% reported it decreased their enthusiasm (Figure 1 Panel C). Unvaccinated participants reported the $100 incentive decreased their vaccination likelihood more than those who delayed (25.3% vs 6.1%, P < .001). No differences in vaccine hesitancy were found when comparing groups by age, race, sex, or education level.
Discussion
Multiple states implemented incentive systems to increase COVID-19 vaccination rates. While several studies have used administrative datasets and simulation models to determine the efficacies of these initiatives, their analyses are limited by multiple confounders and variable data quality. To our knowledge, we report the first prospective study directly asking Ohio residents their opinions on financial incentives for becoming vaccinated.
Financial incentives were not positively associated with increased self-reported vaccination likelihood in our study population. Only a small percentage of participants reported these programs increased their likelihood, most of whom were already likely to become vaccinated. A far higher percentage felt that these incentives decreased their vaccination likelihood, even among those who delayed vaccination. In contrast, Sehgal’s study found that the Ohio Vax-a-Million lottery was responsible for a significant increase in state-wide vaccination rates when compared with a synthetic control state without these incentives2. Our study suggests that this discrepancy can be explained by one major reason: the initial rise in vaccination rates may have been driven by individuals already planning on receiving vaccine. Notably, Walkey et al. found that the timing of the lottery coincided with expansion in vaccine eligibility to adolescents. When excluding adolescent vaccination rates, the decline in the rate of adult COVID-19 vaccination was higher in Ohio compared with the national population following lottery implementation. This suggests that a large portion of the perceived increase in Ohio vaccination rates was in part due to the expansion of vaccine eligibility to adolescents.
Multiple types of monetary incentives for vaccination have been trialed ranging from lottery incentives to cash payments and noncash rewards. A comparison of lottery and nonlottery states revealed that vaccine administrations did not significantly increase following lottery implementation10. Guaranteed cash payments have been as promising and estimated to increase vaccination uptake by 8%11. A pilot program in North Carolina gave $25 cash cards to those getting vaccinated and their respective drivers4. It is unclear whether the success of this initiative was primarily due to monetary incentives or removal of transportation barriers. Financial incentives alone do not address the underlying concerns that individuals have regarding vaccination. COVID-19 vaccine hesitancy consists of several concerns such as the rapid development of vaccines and politicization of government response to the pandemic12. Our study suggests that monetary incentives alone, without addressing other vaccination concerns, will not increase trust in the vaccine.
Behavioral economics has generally regarded financial incentives as a mechanism for overcoming “present bias” whereby individuals disproportionately weigh present, rather than future costs in their decision making (eg, the certain inconvenience of a vaccination appointment and possible side effects are weighed higher than the longer term, uncertain risk of contracting an infectious disease)13. Rather than improving health literacy and promoting health aligned decisions, financial incentives actually exploit “present bias” by creating near term favorable conditions intended to outweigh other factors in vaccination decision making. However, in our study we found evidence of a form of reactivity to financial incentives not previously highlighted. The precise mechanism of this reactivity is unknown, but we hypothesize that the asymmetric paternalism of the lottery and cash incentives resulted in a form of negative confirmation bias14. We infer that patients with limited trust in public officials or concerns about side effects, effectiveness, and/or risks of being vaccinated against COVID-19 had these negative perceptions and concerns strengthened by the observation that policy makers felt the need to offer a financial incentive. The direct generalizability of this study is limited to residents of Northeast Ohio who use health services. In addition, the timing of our survey did not correspond immediately with the initiation of the lottery. We did not collect insurance type, and we were thus unable examine differences by insurance type. These limitations necessitate that future surveys include persons who do not routinely use health care from a wider range of sociodemographic backgrounds and regions. In light of the manner that our results contradict those of other studies of incentives, use of prespecified experimental designs should be prioritized to provide further evidence of the efficacy of financial incentives on increasing vaccine acceptance before reestablishment of or further investments in these programs.
These limitations are balanced by several notable strengths of our work compared with other studies on financial incentives to vaccination: a high response rate, direct survey of a racially diverse population of medical patients who have not been vaccinated or have delayed vaccination, and examination of the association between self-reported vaccination intentions and financial incentives. In this study, we found that financial incentives can have a polarizing influence on vaccination decision making and policy makers need to acknowledge this possibility when selecting among public health strategies. While our findings do not fully discard the potential value of financial incentives to vaccination, they suggest that a broader range of strategies will be necessary.
Notes
This is the Ahead of Print version of the article.
This article was externally peer reviewed.
This project was funded in part by the Veteran Affairs Merit funding grants CX001791 and BX005480. This project was also supported by the Clinical and Translational Science Collaborative (CTSC) of Cleveland which is funded by the National Institutes of Health (NIH), National Center for Advancing Translational Science (NCTAS), Clinical and Translational Science Award (CTSA) grant, UL1TR002548. The content is solely the responsibility of the authors and do not necessarily represent the official view of the NIH.
The authors have no conflicts of interest to declare.
To see this article online, please go to: http://jabfm.org/content/00/00/000.full.
- Received for publication August 1, 2022.
- Revision received October 6, 2022.
- Accepted for publication October 7, 2022.




{kind=link}