
Article Figures & Data
Figures
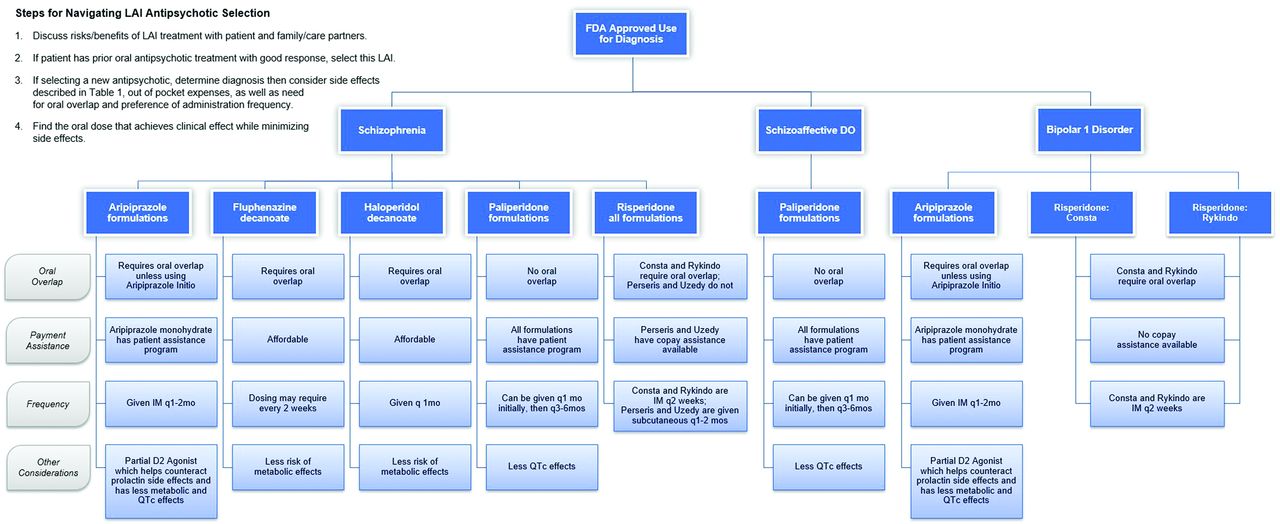
- Figure 1.
Typical treatment approaches of first identifying FDA approved uses, then key characteristics driving possible choice.

Tables
Frequency Monitoring Management Metabolic Syndrome 4 months after initiation, annually thereafter Weight, circumference, lipid panel, fasting glucose or HbA1C Lifestyle changes with diet and exercise are a first-line treatment, consider switching to antipsychotic with lower propensity for metabolic side effects if this will not destabilize the patient (d), medical treatment of metabolic syndrome may be necessary. Antipsychotics that have the lowest risk of metabolic syndrome are asenapine, aripiprazole (LAI available), lurasidone, ziprasidone, haloperidol (LAI available), cariprazine, brexpiprazole, and lumetaperone.24 Movement Disorders Each visit clinically, formally q6 months-annually Abnormal Involuntary Movement Scale, etc. Lower dose or switch to lower potency antipsychotic if it will not destabilize the patient, such as clozapine or quetiapine. If unable to change/switch, first choice medication is a VMAT2 inhibitor for Tardive Dyskinesia and anticholinergic drugs for drug-induced parkinsonism.25 Agranulocytosis First visit after initiation, then annually ANC, discontinue if ANC <1000 Discontinue if ANC <1000.23 and initiate broad spectrum antibiotics. Switch to another antipsychotic if it will not destabilize the patient, the antipsychotics with highest risk are clozapine, quetiapine, and olanzapine. If the patient must be re-trialed on the same medication, obtain a hematology consultation, wait until ANC normalizes above 1000.23, and consider only the oral form.26 Prolonged QTc After initiation in patients with sudden cardiac events in family or known risk for QT prolongation (ie, metabolic derangements, on other medications known to prolong QTc, etc.) 12-lead EKG If QTc is greater than 500 ms, consider dose reduction or switch to alternate medication with low QTc prolongation and a referral to cardiology. If QTc greater than 470 ms in women or 440 in men but less than 500, decrease the dose of the medication or switch to drug with lower risk of prolongation if this will not destabilize the patient. Antipsychotics with the lowest risk of QTc prolongation are perphenazine, aripiprazole, paliperidone, asenapine (no LAI available), and lurasidone (no LAI available).27 Abbreviations: QTc, heart rate–corrected QT interval; ANC, absolute neutrophil count; LAI, long-acting injectable antipsychotics.
Medication FDA Approval Cost Patient Assistance Program Available Initial Oral Supplementation Required Dosing Special Characteristics Aripiprazole lauroxil, Aristada Schizophrenia $2,945-$3,320 No, but copay assistance available Oral overlap for 21 days, or no overlap if given 30 mg oral plus Aristada Initio 675 mg 441 mg-1064 mg monthly to every 2 months depending on dose Also has partial D2 Agonism; CYP3A4 and CYP2D6 substrate Aripiprazole monohydrate, Abilify Maintena and Abilify Asimtufii Schizophrenia, Bipolar 1 Disorder Maintenance $2,010-$3,009 Yes Yes, 2 week oral overlap Maintena 300-400 mg IM monthly
Asimtufii 720-960 mg IM every 2 monthsAlso has partial D2 Agonism Fluphenazine decanoate, Prolixin Dec Psychosis $47.18-$159.60 No Yes 6.25 mg to 25 mg IM or subcutaneously every 2 to 4 weeks approximately 1.25 times the oral dose CYP2D6 substrate Haloperidol decanoate, Haldol Dec Chronic Psychosis $19.62-$60.48 No Yes 10 to 15 times the oral haloperidol equivalents IM monthly; if the amount exceeds 100 mg, the first injection should be limited to 100 mg and the remaining balance injected 3 to 7 days later CYP3A and CYP2D6 substrate Paliperidone Palmitate (Invega Sustenna) Schizophrenia, Schizoaffective Disorder $518.80-$11,416 covered by most insurances Yes No Pending CrCl, 78 mg-234 mg IM Monthly Contraindicated in severe renal impairment; CYP3A4 substrate Paliperidone Palmitate (Invega Trinza) Schizophrenia $3,203-$11,075 every 3 months, covered by most insurances Yes No, following 4 months of Invega Sustenna 273 mg-819 mg IM every 3 months Contraindicated in severe renal impairment; CYP3A4 substrate Paliperidone Palmitate (Invega Hafyera) Schizophrenia $13,991-$20,981 every 6 months, covered by most insurances Yes No, following 4 months of Invega Sustenna or one 3 month cycle of Invega Trinza 1092 mg-1560 mg IM every 6 months Contraindicated in severe renal impairment; CYP3A4 substrate Risperidone Consta Schizophrenia, Bipolar 1 Disorder Maintenance $1,157-1,303 covered by most insurances No Oral overlap for first 3 weeks 25-50 mg every 2 weeks CYP3A4 and CYP2D6 substrate Risperidone Perseris Schizophrenia $2,189-$2916 No, but copay assistance available No Subcutaneous monthly CYP3A4 and CYP2D6 substrate Risperidone Rykindo Schizophrenia, Bipolar 1 Disorder Pricing unavailable at this time No Yes, oral overlap for 7 days IM every 2 weeks CYP3A4 and CYP2D6 substrate Risperidone Uzedy Schizophrenia $1,306-$6495 No, but copay assistance available No Subcutaneous every 2 months CYP3A4 and CYP2D6 substrate *Olanzapine decanoate was not included in the paper because of its infrequent use possibly because of its risk of Post-Injection Delirium/Sedation Syndrome (0.07%) and with need for extensive monitoring post injection (approximately 3 hours).24
Abbreviation: FDA, food and drug administration.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.