
Abstract
Background: Climate change poses a threat to the health of people worldwide. Little is known about the awareness of primary care clinicians toward climate change and if they are open and prepared to address climate change issues with their patients. As pharmaceuticals are the main source of carbon emissions in primary care, avoiding the prescription of particular climate-harmful medications is a meaningful contribution to the reduction of greenhouse gases.
Methods: This is a cross-sectional questionnaire survey among primary care clinicians in West Michigan conducted in November 2022.
Results: One hundred three primary care clinicians responded (response rate 22.5%). Nearly 1/3 (29.1%) were classified as climate change unaware clinicians who perceived that global warming is not happening, or expressed that it is happening but not caused by human activities or is affecting the weather. In a theoretical scenario on a prescription of a new drug, clinicians tended to prescribe the less harmful drug without discussing options with patients. Although 75.5% of clinicians agreed that climate change aspects have its place in shared decision-making, 76.6% of clinicians expressed a lack of knowledge to advise patients in this regard. In addition, 60.3% of clinicians feared that raising climate change issues in consultations may adversely affect the relationship with the patient.
Discussion: Although many primary care clinicians are open to addressing climate change in their working environment and with their patients, they lack knowledge and confidence to do so. In contrast, the majority of the US population is willing to do more to mitigate climate change. Although curricula on climate change topics are increasingly implemented in student education, programs to educate mid- and late-career clinicians are lacking.
Introduction
Climate change is threatening the health of millions of people worldwide.1 Recently the United Nations Intergovernmental Panel on Climate Change (IPCC) emphasized that climate change is happening faster than expected. Ironically, the health care sector whose duty includes the prevention from harm is a major contributor to carbon emissions: in the US, an estimated 10% of national greenhouse gases are emitted by the health care sector.2 In the US, greenhouse gas and toxic air pollutants have been associated with an estimated loss of 388,000 disability-adjusted life years in 2018.3 The health care sector has become an increasingly important target for action in mitigating climate change for policy makers on the federal level.4,5 However, little is known about the obstacles and challenges in addressing climate change in the actual provision of patient care. Pharmaceuticals have been described as the major source of greenhouse gases in primary care,6 and changing prescription practice is likely to reduce carbon footprints.7 For example, recent publications stressed that reducing the prescription of hydrofluoroalkane (HFA) metered dose inhalers in asthma and COPD patients in favor of dry powder and soft mist inhaler formulations would reduce carbon emissions in outpatient care considerably.8⇓⇓⇓–12 The hydrofluorocarbon-based propellant gases in metered dose inhalers slowly disintegrate in the atmosphere over decades and trap solar radiation reflected from the earth and thus heat up the atmosphere.13 As the role of medical professionals entails an ethical obligation to maintain health and support healing at its core, mitigating climate change and its consequences will support health now and for generations in the future. Primary care clinicians especially can exert influence through their entrusted status in the communities and patients that they serve by providing education on climate-change-related health concerns (eg, heat waves, air quality and respiratory illness, food insecurity), by supporting favorable policies for example, by introducing planetary health education and training concepts, or by including climate change aspects in their decision-making.14 Although some studies have surveyed the awareness and self-perceived knowledge of various medical clinicians15,16 including family physicians,17 perception and willingness to address climate-change in shared decision-making has not yet been a subject of study.
This study aims to assess (1) the awareness of climate change, and (2) the willingness to include climate change-related aspects in shared decision-making with patients among primary care clinicians.
Methods
This is a cross-sectional survey study among primary care clinicians in West Michigan conducted in November 2022.
Setting and Recruitment
Corewell Health is a nonprofit managed care health organization with 14 hospitals and multiple outpatient facilities and is the largest health care clinician in the West Michigan area with more than 1.4 million residents.18 For the study, we identified all 457 primary care clinicians in the Corewell Health West network that regularly provide primary care to patients in family medicine, general internal medicine, internal medicine/pediatrics and pediatric clinics. This clinician pool comprises resident and attending physicians, clinical psychologists, nurse practitioners, and physician assistants. External contractors and administrative staff without patient contact were excluded. We set up a self-administered questionnaire with 28 close-ended questions using the online survey tool Alchemer (Widgix, LLC dba Alchemer, Boulder CO) and invited eligible persons to participate. Invitation e-mails to participate in a “Survey on Climate and Medical Practice” were sent on October 12, 2022, and a follow-up reminder was sent on November 23, 2022. The survey was closed on December 6, 2022. Participants did not receive compensation for participation. Survey data were retrieved and processed in a deidentified manner.
Questionnaire Development
The 28-item questionnaire used for this survey consisted of 3 parts (see Online Appendix):
Questions on climate change awareness, risk perception, policy support, and behaviors (Questions 1-10). These items were selected from the questionnaire used for the Yale Project on Climate Change Communication.19
Questions on the medical system’s contributions to climate change, opinions on addressing climate change issues in shared decision-making for drug treatment (Questions 11-22). These aspects were deemed as highly important, as literature showed that a significant proportion of carbon emissions in the health care sector can be attributed to pharmaceuticals. Other research highlighted that a changing of prescription habits in favor of more greenhouse friendly medications would have a considerable impact in mitigating climate change. The key questions in this part are preceded by a thought exercise:
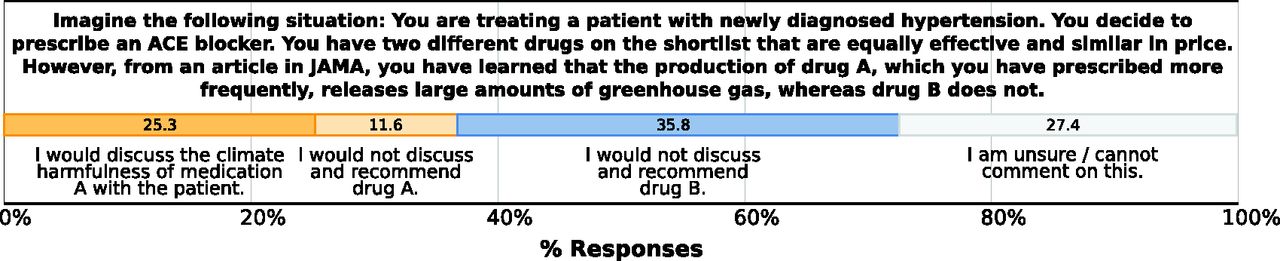
Imagine the following situation: You are treating a patient with newly diagnosed hypertension. You decide to prescribe an ACE blocker. You have two different drugs on the shortlist that are equally effective and similar in price. However, from an article in JAMA, you have learned that the production of drug A, which you have prescribed more frequently, releases large amounts of greenhouse gas, whereas drug B does not.
In the following, clinicians are asked not only which drug they would prescribe, but whether they would discuss this aspect with the patient, and if they think that these considerations have any place in the shared decision-making process.
c. Questions on participants’ sociodemographics (age, gender, occupation, years of clinical experience, clinic setting [urban, suburban, rural]).
The questionnaire contains closed-ended questions and no free-text entries. Most of the questions can be answered on 4- or 5-point Likert scales (eg, strongly agree, somewhat agree, somewhat disagree, strongly disagree). The questions were developed in a discursive process involving all authors following both deductive (literature research) and inductive approaches (group discussions). A preliminary questionnaire was then pretested to 5 3rd-year medical students and refined. The estimated time needed to complete the survey was 6 to 12 minutes.
Statistical Analysis
Survey results were exported from Alchemer as CSV data and subsequently imported to SPSS 28 (IBM, Armonk, NY) with which all statistical analyses were conducted. Descriptive statistics including absolute and relative frequencies, mean, and standard deviation (S.D.) are used to describe responses. Chi-Square, Fisher’s exact test, and Fisher-Freeman-Halton test, where appropriate, were used to test for independence between categorical variables. Mann-Whitney U, or Kruskal-Wallis test was used to test categorical data with numeric variables including variables with a staged Likert scale. Correlations between clinician’s age and answers on a Likert scale were assessed using Spearman’s rho. Clinicians’ age was also grouped in 3 generation cohorts: “Baby Boomer” (with birthyear before 1964 and thus currently 58 years or older), “Generation X” (with birthyear between 1965 and 1982, thus currently 40 to 57 years old), “Millennials/Gen Z” (with birthyears after 1983 and thus currently <40 years old). P-values <0.05 were considered as significant.
Research Ethics
This project received approval from the Institutional Review Board of Corewell Health (IRB# 2022-334). Before answering the questionnaire, participants were asked to declare consent to participate.
Results
Response Rate and Sociodemographics
We received 103 responses out of 457 eligible participants (response rate of 22.5%) with lower response rates among nurse practitioners and physician assistants (P = .027) (Table 1). However, gender imbalance between survey respondents and nonrespondents was not found (P = .113).
Response Rate
Those who completed the questionnaire were on average 44.3 years old (min 24, max 65, S.D. 10.8), predominantly female (59.1%) and had on average 15.8 years of working experience (min 1, max 39, S.D. 9.9). Gender imbalance was found in favor of NPs and PAs, with more females (P = .003). Gender imbalance was not found among clinicians age or age-group (P = .241). Most clinicians (42.2%) worked in a suburban clinical setting. More information is provided in Table 2.
Participants' Demographic
Clinicians’ Climate Change Awareness
The vast majority of clinicians acknowledged that global warming is happening (97.9%), is a result of human activities (76.5%) and already affecting the weather in the US (90.1% strongly agree & somewhat agree). A total of 29.1% (n = 30) of surveyed clinicians stated that global warming is not happening or expressed that it is happening but not caused by human activities or is not affecting the weather. This group was a priori defined as climate change unaware clinicians. This group was significantly older than those aware of climate change (mean, 47.7 years [S.D. 11.5 vs mean 43.0 years [S.D. 10.3], P = .047) and more often male (53.8% vs 34.8%, P = .038). Significant differences between unaware and aware clinicians were not found based on clinicians’ qualification (physician/NPs/PAs/other) or the clinic location (urban/suburban/rural).
More results on clinicians perception on climate beliefs, risk perception and policy support are displayed in Figure 1. Results are reported as percentages.

Clinician's beliefs, risk perception and views on policy support toward climate change issues.
Clinicians’ Perceptions Based on Sociodemographics
Clinicians’ gender played a significant role on how climate matters were perceived: Female clinicians more often attributed global warming to human activities (85.5% vs 70.3%, P = .012) and agreed more often to the statement that global warming is affecting the weather in the United States (65.5% vs 48.6% strongly agree, P = .014). In addition, female clinicians were more often very or somewhat worried about global warming (92.7% vs 72.9%) then male clinicians (P = .004). The question “How much do you think global warming will harm people in the US?” was more often answered by women with “a moderate amount” or “a great deal” than by men (89.1% vs 70.2%, P = .028). Similarly, female clinicians were more often expressing concerns about personally being harmed by climate change (68.6% vs 44.5% “a moderate amount” or “a great deal,” P = .002). However, 78.4% of male clinicians were convinced that climate change already harms people in the US whereas 61.8% of female clinicians stated so (P = .002). Female respondents were more likely to want to see more engagement of government to address global warming than males (89.1% vs 75.7% do “more” or “much more,” P = .012).
Clinicians from “Generation X” stated that they discuss global warming with friends and family (79.5%) more often than “Baby-Boomers” (58.9%), and “Millennials/Gen Z” (48.6%) (P = .027). In addition, “Generation X” clinicians thought more often that global warming will harm US citizens (“is a great deal”/“a moderate amount”: 90.9%) whereas 77.1% of “Millennials/Gen Z” clinicians and 53.9% of Baby-Boomer clinicians thought so (P = .019). The vast majority (77.2%) of “Generation X” clinicians stated that global warming will harm them personally (“a great deal”/“a moderate amount”), versus 50% of “Millennials/Gen Z” clinicians and 8.3% of “Baby-Boomer” clinicians (P < .001).
Although clinicians from urban clinics were more in favor that the government should do “much more” (75%) to mitigate global warming, this was less the case for clinicians working in suburban (57.5%), and rural (45.2%) clinics (P = .004). However, highest rates that the government should do much less was also found among urban clinicians (12.5%) and less often among suburban (7.5%) and rural (0%) clinicians.
Clinician’s degree was not associated with survey responses.
Raising Climate Change Issues in Decision-Making
A small portion of clinicians (30.3%) thought about how they can avoid CO2-emissions in their work routine. More male clinicians than female clinicians expressed this thought (43.2% vs 25.5%, P = .012). Half of the clinicians mentioned that their patients never raised any concerns about climate change in consultations, 41.8% of clinicians indicated that this happened rarely, 6.1% sometimes, and 0% often.
Figure 2 depicts the responses to the thought exercise on the decision-making process for 2 pharmaceuticals available for prescribing of which 1 (drug A) has a considerably worse impact on the climate than the other (drug B).

Result on drug prescription scenario.
Climate change unaware clinicians tended to answer “unsure/cannot comment on this” (42.9% vs 20.9% for aware clinicians) or recommend drug A (25% vs 6% for aware clinicians, P = .001). Clinicians’ gender, age-group, degree (physician/NPs/PAs/other) or the setting of the clinic was not significantly associated with responses.
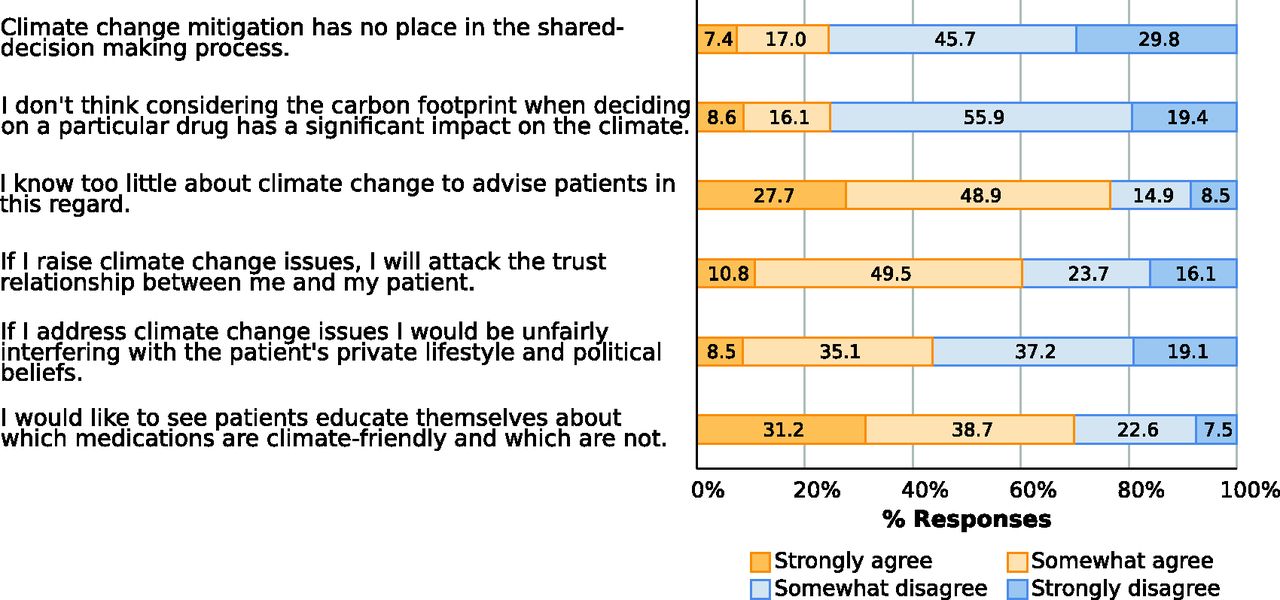
Figure 3 shows responses on the questions related to how clinicians perceive adding climate change issues in the shared decision-making process with their patients. The vast majority strongly or somewhat disagreed that climate change has no place in decision-making (75.5%) or that considering climate-harmfulness in prescriptions does not have a significant impact on climate (75.3%). Many clinicians (76.6%) agreed strongly or somewhat that they knew too little to provide advice to patients in climate change matters, and 60.3% of clinicians agreed strongly or somewhat that they would attack the trust relationship with their patient when addressing climate change issues with the patient.

Perception on including climate change issues in shared decision-making.
Clinicians’ gender was not significantly correlated with the responses. Younger clinicians tended to be concerned that raising climate change issues negatively impacts the relationship with the patient (r = −0.22, P = .036); however, when age was categorized into generational groups, we did not find significant differences (P = .096). Clinicians from urban clinics considered themselves more proficient on climate change topics (42.5%) than clinicians from suburban (20%) or rural (12.9%) clinics (P = .008). We did not find any correlation between clinicians’ degree (physician/NPs/PAs/other) on the responses.
Discussion
Climate Change Awareness
Our survey found that although most primary care clinicians acknowledged the existence and the actual threat of climate change, there are many climate change unaware clinicians (29%) that either doubt the existence of global warming, the human impact on climate change, or that climate change will impact weather patterns. This is somewhat surprising given the science required in health care, and the clear evidence behind climate change. A complete denial that climate change is happening was only present in 2% of the studied clinicians. This is similar to the results of another study from Wisconsin where 2% of family medicine physicians responded “no” to the question “Is global climate change occurring?”.17 The Yale University survey studied climate change beliefs, risk perceptions and policy preferences and provides estimates on local levels based on a dataset of more than 28,000 participants.20 Compared with their 2021 survey results,19 the clinicians in our study were much less prone to denial climate change (2% vs 17%) and more worried about global warming (82% vs 59%) than the local West Michigan population.
We detected a significant difference in gender where respondents identifying as female were much more concerned with climate change, were more convinced that climate change already has an impact on people in the US and are more often in favor of seeing the government doing more to address global warming. This finding is in line with previous studies highlighting a gender gap in environmental concerns with women being more likely expressing concerns about environmental hazards then men.21 Although we have not systematically obtained clinicians’ race, ethnicity and political beliefs, research suggests that White men and especially conservatives are likely to express less concerns on climate change issues and endorse more denialist beliefs than any other gender, ethnic or racial group.22
Contrary to other studies of the general population, surveyed clinicians from “Generation X” were the generation that most likely identified climate change as a threat, compared with clinicians from the younger “Millennials/Gen Z” generation and the “Baby-Boomer” clinician group. Other studies using a representative US sample with a similar question set showed that “Millennials/Gen Z” were significantly more concerned about climate change than “Generations X” and “Baby Boomers”.23 Other researchers indicated that climate change-associated feelings of worrying, anger and guilt were highest among Millennials/Gen Z and increased considerably within the last decade.24
Other studies showed that medical students' perceptions of climate change are similar to those of “Generation X” clinicians in our study.25 For the next generations of clinicians, it remains to be confirmed whether these opinions will change. It is also not clear what the impact of more noticeable climate change, and new curricula on climate change, which are still not very widespread,26 may have on clinicians perceptions.
Lastly, it is noteworthy that clinician’s awareness and perception of climate change did not differ among different degrees such as physician, nurse practitioner and physician assistants.
Addressing Climate Change Issues in Decision Making
To our knowledge, this is the first study of primary care clinicians attitudes on the willingness and readiness to include climate change aspects in their shared decision-making process. We developed a theoretical scenario where primary care clinicians could use shared decision-making to change a medication that would considerably reduce carbon emissions.
The response to this scenario was highly varied. First, it is noteworthy that only a minority of clinicians (11.6%) would knowingly prescribe a medication that is harmful to the climate. A quarter of clinicians would discuss the climate-harmfulness of the medication with the patient in the sense of shared decision-making. However, this is opposed by the feeling of interfering too much with the patient's personal attitudes or jeopardizing the trust relationship. Nevertheless, many patients may welcome this conversation as the Yale climate opinion map suggests that 65% of the West Michigan population is willing to do more to combat climate change.19
Many clinicians (35.8%) take the approach of prescribing the more climate-friendly drug without informing the patient about the climate-damaging alternative. This reveals the fundamental will to act in a climate-friendly way once a clinician attained knowledge about a climate harmful drug, but does not bring the patient on board as an ally and thus misses the opportunity to make climate protection a topic in health care and to set oneself up as a trustworthy person for discussions. This decision seems reasonable in light of the fact that the vast majority of clinicians confirmed that they do not know enough to advise patients about climate change, its health impacts and the possibility of climate-friendly action through shared decision-making. Structured training curricula for clinicians at all career levels would be advisable, especially because only a small minority of clinicians felt that climate change aspects should not be a topic in an office visit. Interestingly, rural clinicians were more prone to state a lack of knowledge about climate change. The American Medical Association recently passed a resolution on including climate change in the medical curriculum.27 Although a framework for a residency curriculum on climate change has been proposed,28 it remains unknown how widespread those curricula were implemented especially among nonphysician clinicians. Those curricula might add to the knowledge of clinicians who stated they know too little about climate change to advise patients if a situation arose.
We investigated differences in the hazard perception and awareness of climate change among clinicians’ genders. When discussing climate change aspects with patients, no gender differences were found. However, male clinicians were more likely to consider reducing CO2 emissions in their work environment than female clinicians. This could possibly be due to gender imbalance toward male clinicians in more senior ranks29 who can be considered more likely to discuss and decide on measures applied to the workplace.
Although our scenario was fictional, there are drugs with significant climate-damaging potential, notably HFA propellant MDIs and anesthetic gasses, where guidelines have been developed for using more climate-friendly but equally effective drugs.11,30,31 However, most of these guidelines are being discussed in other countries and may be new to primary care clinicians in the US.7,32,33
Currently, primary care clinicians see most of the ambulatory visits in the United States. In their role, primary care clinicians can address climate change considerably by discussing these opportunities with their patients. However, only 30.3% of clinicians considered reducing CO2 emissions at their workplace. As half of all clinicians reported having never been approached by patients concerned about climate change, it is likely that climate change has not become a topic at their clinics. In addition, it seems uncertain if medical professionals and their patients perceive medical care as an opportunity to mitigate climate change.
Strengths and Limitations
Our study has limitations that need to be considered when interpreting the results. First, our clinicians are only located within a single health system in the West Michigan area, where climate change disasters haven’t impacted weather as much as some US locations. However, the Yale study on climate change perception showed that, overall, the West Michigan region population’s was similar to the US general population’s attitudes and perceptions on the matter of climate change.19 The use of a similar question set allows comparisons with the Yale data and other studies using these questions.
Another limitation was our response rate of 22.5% that limits the generalizability. The resulting sample size precluded multivariable analyses which might have introduced a confounding bias. This survey was done during a busy season, where clinicians were dealing with a surge in the RSV virus, along with other health system changes. A low participation rate could also indicate that clinicians do not consider climate change as sufficiently important for the provision of medical care in their clinics. Other surveys on climate change awareness among clinicians had similar17 or even lower response rate.15,16 However, results indicated that not all respondents were climate change aware, suggesting that our sample was not necessarily biased. Finally, although we created a scenario to assess clinician behaviors, we are not sure if this scenario would be similar to an actual patient encounter where clinicians were given a choice with actual medications. There are many factors in medication prescribing, often most importantly cost and insurance coverage. Our team plans to repeat this survey in a more representative sample of Primary Care Clinicians across the US.
In summary, this study provides a starting point for assessing primary care clinicians’ thoughts on climate change. Further investigations should include qualitative research methods to gain a deeper understanding about the feelings and considerations of clinicians regarding discussing climate change aspects with patients. To reduce the carbon footprint of our health care industry, clinicians, patients, pharmaceutical and insurance companies will all need to work together using evidence-based strategies.
Conclusions
Our survey suggests that the vast majority of primary care clinicians know that climate change is occurring, but they are unsure what to do about it in their role as medical professionals. In accordance with studies on the general population, female clinicians were more concerned about the threats of climate change. Despite a large proportion of clinicians concerned with climate change, clinicians lack the knowledge to advise patients in the shared decision-making process.
This can be complicated by the feeling that clinicians are unfairly interfering with the patient's political and personal convictions and jeopardizing the relationship of trust. In contrast, a majority of people in the US want to do more to combat climate change. We strongly advocate that knowledge about climate change should be included in continuing education curricula in primary care, for the good of our patients and our planet.
Acknowledgments
Dr. Müller and Dr. Holman had full access to all the data in the study and take responsibility for the data's integrity and the data analysis's accuracy. Concept and design: Müller, Holman, Bouthillier. Acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript: Skok, Müller. Critical revision of the manuscript for important intellectual content: All authors. Statistical analysis: Müller. Administrative, technical, or material support: Holman, Bouthillier.
Due to the decision of the responsible institutional review board, survey raw data are not published, however, can be obtained from the authors on a reasonable request within a data sharing agreement.
The authors want to express thanks to the Scholarly Activity and Scientific Support Office (SASS) at Corewell Health for their assistance in drafting the study protocol and enabling access to the online survey tool.
Appendix
Notes
This article was externally peer reviewed.
Funding: Frank Müller received the Peter C. and Pat Cook Endowed Clinical Research Fellowship 2022/2023. The funding organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Conflict of interest: The authors have no conflicts of interest.
To see this article online, please go to: http://jabfm.org/content/37/1/25.full.
- Received for publication January 23, 2023.
- Revision received March 18, 2023.
- Accepted for publication March 27, 2023.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Integrating environmental sustainability in clinical counselling: a randomised, double-blinded, experimental vignette study of satisfaction with care
- Implementation of decarbonisation actions in general practice: a systematic review and narrative synthesis
- A Focus on Climate Change and How It Impacts Family Medicine