
Article Figures & Data
Figures
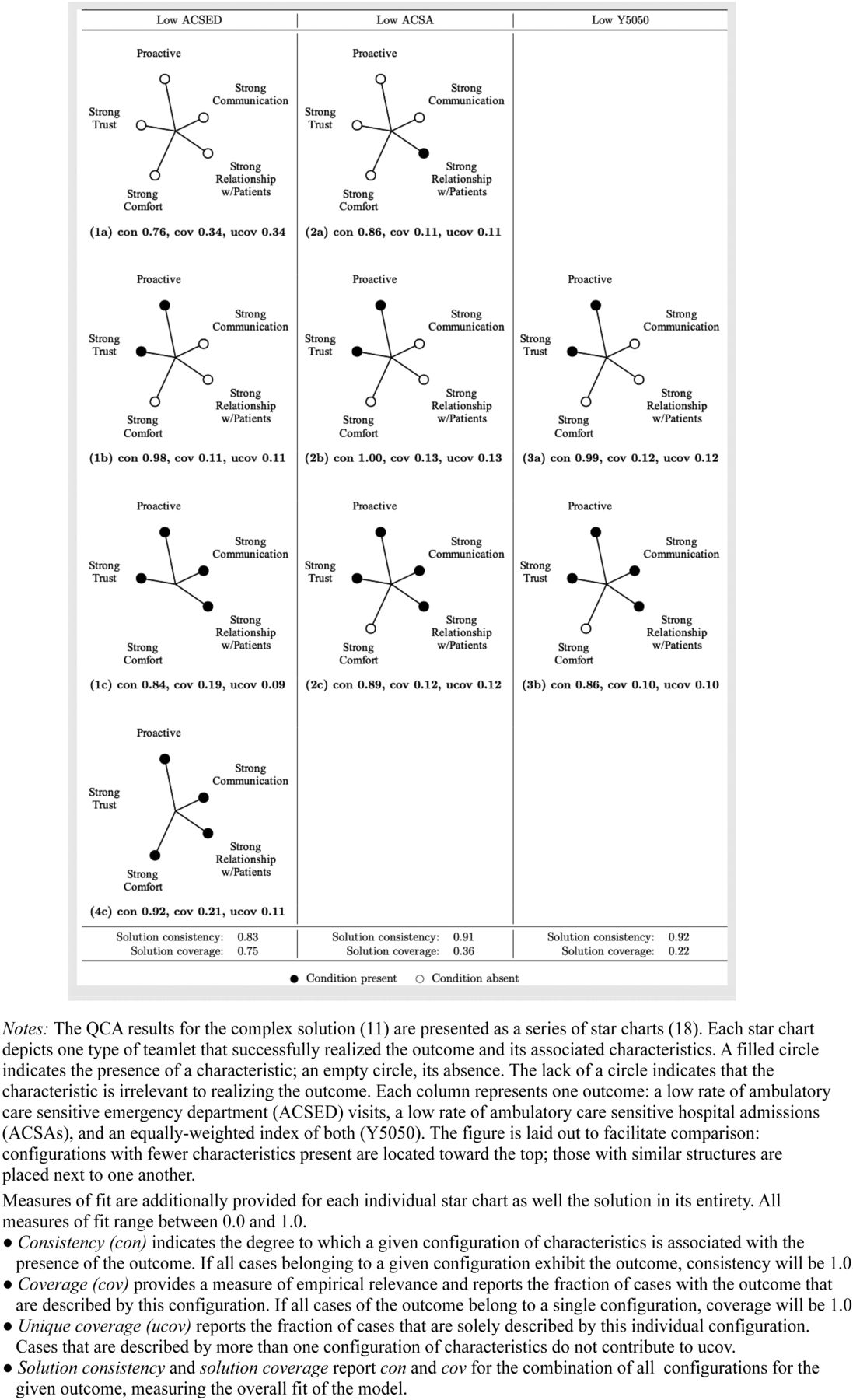
- Figure 1.
Star chart of teamlet types with low rates of ambulatory care sensitive emergency department visits and hospital admissions.

Tables
Characteristic Description Calibration Rules Outcomes Ambulatory Care Sensitive Emergency Department (ACSED) visits Low ratio of observed-to-predicted ACSED visits, with “low” defined as ≤ half as many observed visits as predicted (i.e., a 1:2 ratio) A continuous measure ranging from 0.0 to 1.0, where 0.0 represents ≥ 2:1 ratio, 0.5 = 1:1 ratio and 1.0 ≤ 1:2 ratio Ambulatory Care Sensitive Hospital Admissions (ACSA) Low ratio of observed-to-predicted ACSA, with “low” defined as ≤ half as many observed visits as predicted (i.e., a 1:2 ratio) A continuous measure ranging from 0.0 to 1.0, where 0.0 represents ≥ 2:1 ratio, 0.5 = 1:1 ratio and 1.0 ≤ 1:2 ratio Y5050 (composite measure defined under description) Mean of ACSED visits and ACSA (ACSED visits + ACSA)/2 Explanatory Characteristics Trust Physician reports high degree of trust in the staff member’s judgment 1.0 = Trusts staff member very enthusiastically 0.75 = Trusts staff member but not very enthusiastically OR survey indicates a great deal of trust but not discussed in interview 0.25 =Trusts staff member only moderately 0.0 = Low level of trust Relationship (rel) Physician and staff member both report that the staff member has a good relationship with patients 1.0 = High level of trust, comfort, or rapport from patients 0.75 = Moderate level of trust, comfort, or rapport from patients 0.0 = Low level of trust, comfort, or rapport from patients Communication (comm) Physician and staff member both report good communication in the teamlet Composite-value from 0.0 to 1.0 calculated by: (“good communication” score x 0.5) + (“can the staff member speak up when they think the physician made a mistake” score x 0.3) + (“respect for each other” score x 0.2) Proactiveness of the staff member (proactive) Staff member is highly proactive in anticipating the physician’s needs 1.0 = Staff nearly always proactive and anticipates physician needs 0.75 = Staff proactive and anticipates physician needs more often than not 0.0 = Staff has little or no knowledge of physician preferences and is not proactive Comfort Physician and staff member both report feeling comfortable and familiar with the other 1.0 = Expresses comfort and familiarity very enthusiastically 0.75 = Expresses comfort and familiarity 0.0 = Expresses significant discomfort and unfamiliarity - Table 2.
Key Qualitative Comparative Analysis Characteristics and Sample Quotes from Qualitative Interviews
Quotes from Physicians Quotes from Staff Members Proactiveness of staff member in anticipating physician needs “I very much prefer the one-on-one. I have my staff person, and she has one physician. You really get to know the person. You get to know how they work, how they operate after years. They kind of read your mind at times and know what you want before you want it.”
“We know each other well enough to anticipate what the next move is. For example, if I'm going to take a lesion off of somebody's skin, she… has all the instruments that I need, and they are all in the room when I go in… She knows exactly the kind of help I need when I'm doing something like that without having to say.”“In the beginning, of course, we were strangers. We didn't really know how each other worked. But, as time progressed, I learned more of how she works as a doctor… And then it helps a lot with patient care… We know right away what we or she needs me to do for the patient.”
“I'm one step ahead of him. I help him out before he sees the patient… If a patient comes with a urinary tract infection, I give them the cup [to check the urine]… For chest discomfort, I would do an EKG, so I'm one step ahead… So I start doing all of that… so he could take more time with the other patients that are coming in.”Good relationships between staff member and patients “She takes the best social history on my patients. She knows the names of the pets of my patients. She knows if they've had a major loss, if they lost their job or a loved one… I think [the patients] see her each time, and she takes a personal interest in them. I think they feel a strong relationship with her. That makes my job easier. The patients are coming in more relaxed… I think seeing the same faces each time gives them comfort and confidence in what we're doing.”
“The patients not only trust her but like her. And that really helps a lot. They know that if they tell her something, it's as good as telling me. They know if they pass something on to her, it will get to me.”“I can't take a vacation without them yelling at me when I get back. [They say], “You weren't here when [the patient] called and the receptionist can't get a word out of them.” Bottom line, [the patients] won't tell the receptionist a darn thing. If they're having a heart attack, they need to talk to me. I've sent several and saved several since by demanding that they go to the ER.” Good communication between staff member and physician “When we mess up, we're both very direct about it. For example, let's say that she forgot to follow up with the patient. She’ll follow up, and we’ll move on… We communicate through computer, through phone, [or] in person. We have all lines of communication open… She understands when to respect my boundaries… So I think our relationship is built upon mutual respect and anticipating what the other needs and it makes a big difference when you work with somebody who understands those things about you.” “We are very real and true to each other. If I snap, I will make sure I acknowledge and apologize for snapping. If she's had a crappy day, she'll do the same. I think having that mutual developed respect and appreciation and also accountability for each other and what we need to do to make the practice run smoothly has made us have a better relationship throughout the years.” Comfort and familiarity between staff member and physician “We try our best to convey that it's not just a workplace. We use it as a second home environment. I tell them all the time. I spend more time with them than my children and my wife. I respect their time, and they respect mine. We have a healthy relationship in the office.” “This is kind of my home away from home… We have kind of like a family relationship where I look forward to coming to work and working for him.” Physician-reported trust in the staff member “I give my medical assistant tremendous latitude. If patients are running late and she wants to move them around [because of] who is sick or who I'm going to be able to catch up with, I don't correct her… I'm not going to second guess. I think that conveys a respect for the person that you trust their judgment. I think [in] any relationship, communication and respect are important. People also want to feel that they're growing in the role, learning new things, or getting additional responsibilities.” Not applicable Low Rate of ACSED visits Low Rate of ACSAs Low Rate of both ACSED visits and ACSAs trust rel comm proactive comfort N scon pri out scon pri out scon pri out 1 1 1 1 1 1 0.86 0.83 1 0.29 0.00 0 0.57 0.25 0 1 1 1 1 0 1 0.83 0.79 1 0.89 0.87 1 0.86 0.83 1 1 1 1 0 1 1 0.75 0.66 0 0.75 0.66 0 0.75 0.66 0 1 0 0 1 0 1 0.98 0.98 1 1.00 1.00 1 0.99 0.99 1 0 1 1 1 1 1 0.98 0.98 1 0.34 0.00 0 0.66 0.49 0 0 1 1 1 0 2 0.46 0.25 0 0.50 0.50 0 0.48 0.39 0 0 1 0 0 1 1 0.02 0.00 0 0.44 0.00 0 0.23 0.00 0 0 1 0 0 0 1 0.54 0.16 0 0.86 0.84 1 0.70 0.57 0 0 0 0 0 0 4 0.76 0.75 1 0.49 0.48 0 0.62 0.56 0 Notes. Nine combinations of characteristics describe 13 teamlets. Rows lacking empirical instances (remainders) are omitted. Three outcomes are reported: ambulatory care sensitive emergency department (ACSED) visit rate, ambulatory care sensitive hospital admission (ACSA) rate, and a composite measure of the ACSED and ACSA rates of equal weighting. The presence of the characteristic is indicated by a 1; its absence, by a 0. Degree of consistency with the presence of the outcome is reported as scon. Pri is a more conservative measure of consistency that removes the influence of ambiguous observations that exhibit consistency with both the presence and absence of the outcome. For a teamlet type to be classified as consistently associated with the presence of the outcome, both scon and pri must exceed 0.75, marked by a 1 in the corresponding outcome (out) column.




{kind=link}