
Abstract
Background: Physician departure causes considerable disruption for patients, colleagues, and staff. The cost of finding a new physician to replace the loss coupled with lost productivity as they build their practice can cost as much as $1 million per departure. Therefore, we sought to characterize drivers of departure from practice with the goal of informing retention efforts (with a special emphasis on the connection between electronic health record (EHR)-related stress and physician departure).
Methods: This qualitative study of semistructured interviews was conducted between October 2021 and April 2022 among 13 attending physicians who had voluntarily departed their position from 2018 to 2021 in a large multispecialty, productivity-based, ambulatory practice network in the Northeast with a 5% annual turnover rate to understand their reasons for departing practice.
Results: Among the 13 participants, 8 were women (61.5%), 3 retired (23.1%), and 6 (46.2%) left for new positions. Major domains surrounding the decision to depart included current features of the health care delivery landscape, leadership/local practice culture, and personal considerations. Major factors within these domains included the EHR, compensation model, emphasis on metrics, leadership support, teamwork/staffing, burnout, and work-life integration.
Conclusions: Opportunities for medical practices to prevent ambulatory physicians’ turnover include: (1) addressing workflow by distributing responsibility across team members to better address patient expectations and documentation requirements, (2) ensuring adequate staffing across disciplines and roles, and (3) considering alternative care or payment models.
- Electronic Health Records
- Leadership
- Personnel Retention
- Physicians
- Psychological Burnout
- Qualitative Research
- Workforce
Introduction
Physician turnover is costly, compromises care quality, and is associated with lower patient satisfaction and poorer quality measure performance, health outcomes, and increased acute care utilization.1⇓⇓⇓⇓–6 Physician professional burnout has been identified as a major driver of physician turnover.6⇓⇓–9 Burnout and dissatisfaction are both independent predictors of plans to leave practice. With burnout rates now dramatically increasing in the setting of the COVID-19 pandemic,10 up to 54% of physicians report changing their employment plans.11 Burnout involves a complex interplay of multiple interdependent factors related to practice efficiency, culture, and personal resilience.12,13 In the domain of practice efficiency, there is growing evidence supporting the association of physician burnout with electronic health records (EHR) use and usability.14⇓⇓⇓⇓⇓⇓–21 Currently, practice leaders have few evidence-based strategies to prevent physician turnover. To understand factors that drive physician departure, we conducted a series of in-depth interviews with physicians who had recently departed from a large, multispecialty ambulatory practice network.
Methods
A descriptive qualitative study of semistructured interviews was performed using thematic analysis to identify factors leading to physician departure.22 The study protocol was approved by our institution’s IRB (protocol #072105). Verbal and written electronic consent were obtained from all participants. Reporting followed the Standards for Reporting Qualitative Research (SRQR) guidelines.23
Participants were recruited from a human resources roster of physicians who voluntarily left employment between 2018 and 2021 from a large, multispecialty ambulatory practice (that uses a productivity-based compensation model) including in the Northeast region of the United States with more than 300 ambulatory physicians and a turnover rate of approximately 5% per year. Eligible participants were contacted by e-mail, phone call, and text message. Enrollment continued until thematic saturation was achieved.22
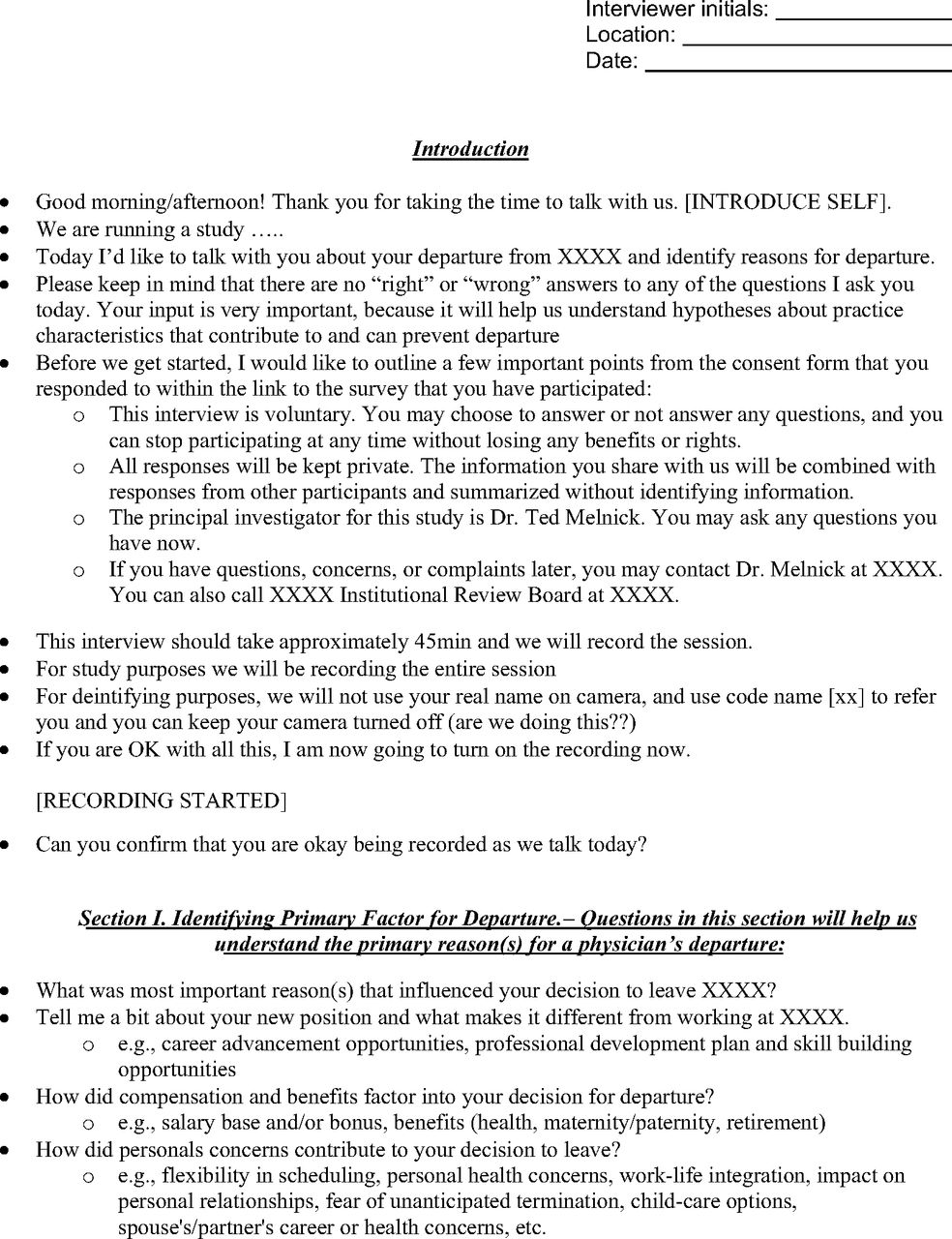
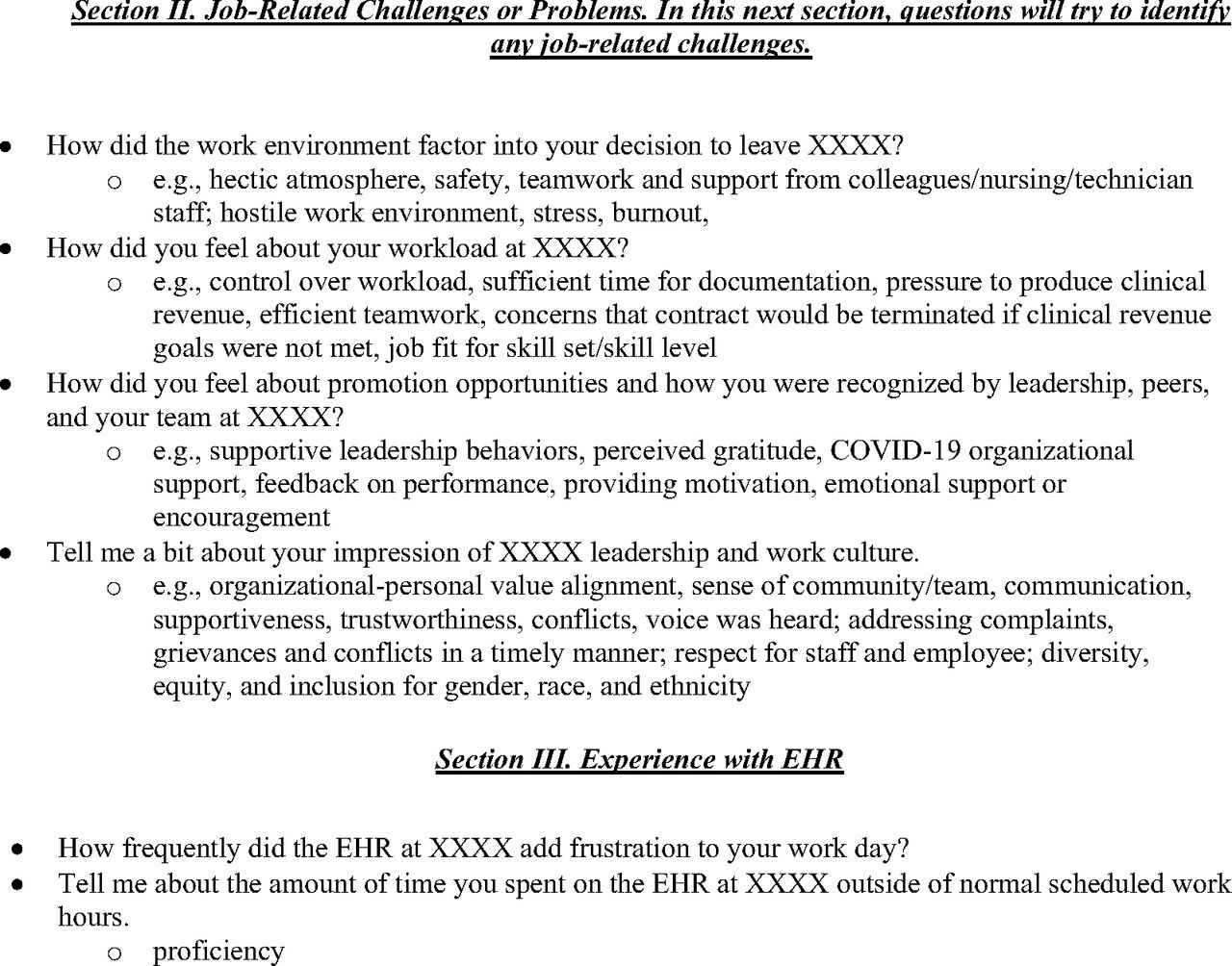
Each interview followed a semistructured interview guide developed and field tested (2 mock interviews conducted before data collection) by our multidisciplinary team. The interview guide (Appendix) included questions about primary reason for departure, job-related challenges, work environment and leadership support, and the EHR. All interview sessions were deidentified, audio-recorded, and professionally transcribed.
Audio-recordings and transcripts were analyzed using the constant comparative method:24 essential concepts from interview data were coded and compared over successive interviews to extract recurrent themes. Qualitative analysis software (ATLAS.ti) was used to organize, sort, and code the data. Two investigators reviewed the audio files for each interview independently, discussed salient themes, then agreed on a set of codes to capture these themes. Initial themes were based on the Stanford Model of Professional Fulfillment, through 3 domains of culture of wellness, efficiency of practice, and personal resilience.25 Transcripts were independently coded with interrater reliability (kappa) 0.94. Discrepancies were adjudicated and resolved by a third investigator. Themes were revised iteratively as patterns within the data emerged and grouped into discrete domains.
Results
The 27 physicians who had most recently voluntarily departed the practice network with sufficient contact information available were contacted. Of these 27, 14 (51.8%) responded and 13 interviews were conducted between October 2021 and April 2022. One respondent declined to participate because they felt their perspective was no longer relevant as they had departed practice before the pandemic. Out of the 13 participants, 8 (61.5%) were female, 5 (38.5%) were ages 35 to 44, 3 (23.0%) were age 65 and over, 6 (46.2%) were White Non-Hispanic, 2 (15.4%) were Asian, 1 (7.7%) was Hispanic, and 6 (46.2%) specialized in internal medicine. Approximately half (54%) of the participants left their practice for a new position, whereas approximately 1 quarter (23.0%) left because they were retiring.
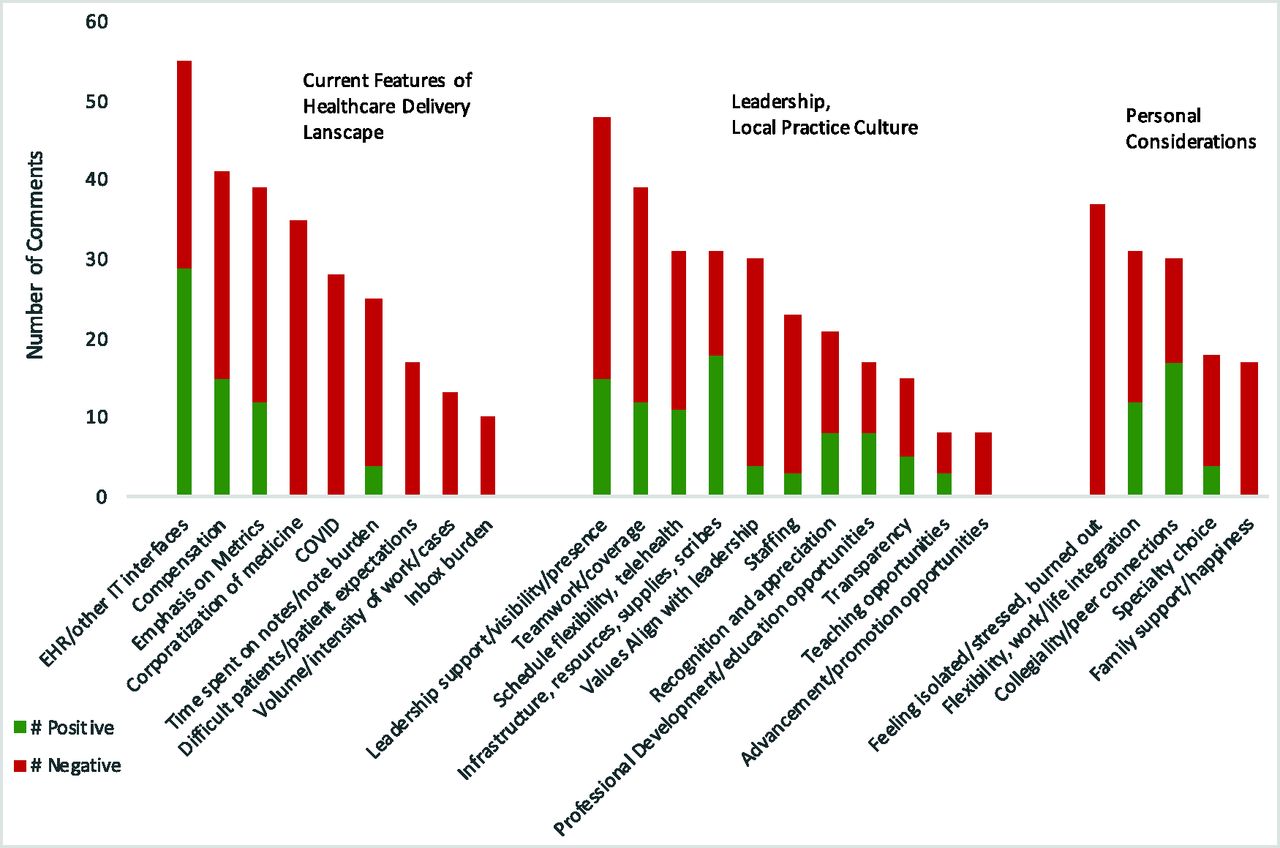
Participants identified factors that contributed to their decision to depart their practice within 3 domains (Table 1): the current features of the health care delivery landscape, leadership/local practice culture, and personal considerations. Aspects from each domain were identified by all participants indicating that—like professional burnout—the decision to depart practice is complex with multiple interdependent factors contributing to it. Major themes affecting the decision to leave included the EHR, compensation model, emphasis on metrics, leadership support, teamwork/staffing, burnout, and work-life integration. Although burnout and EHR-related burden contributed to clinicians’ decision to leave in many cases,26 no participants reported either as the primary driver of their departure. Participants shared that they valued more time off, flexibility, or autonomy over higher earnings with some stating that additional compensation would not have convinced them to stay.
Domains, Themes, and Representative Quotes
Of note, the 3 themes of EHR/other IT interfaces, infrastructure/resources/supplies/scribes, and collegiality/peer connections were noted to have overall more positive than negative quotations associated with them (Figure 1); whereas the following themes had only negative quotations: isolation/burnout, corporatization of medicine, COVID and inbox burden, difficult patients/patient expectations, family support, volume/intensity of work, and advancement/promotion opportunities.

Top 25 most common themes identified, organized by domain.
Discussion
The major domains reported in this qualitative study have similarities to a 2004 review of 14 studies on physician turnover that identified reasons for physician departure in the following domains: financial issues, characteristics of the physician’s practice (as it relates to professional alignment between the physician and their organization's expectations), and personal issues.27 More recent cross-sectional survey studies have also reported burnout, leadership behavior, and COVID-related stress as related to an intention to leave 1’s practice.28⇓–30 However, intention to leave practice may be more of a proxy for job dissatisfaction than an accurate predictor of actual behavior.31 A 2019 longitudinal cohort study of 740 primary care clinicians based on survey data and human resources rosters of actual turnover also noted the contribution of burnout and concluded that solutions must recognize that turnover is multifactorial.9 Self-reported survey data are subject to the limitations of self-report, including response fatigue and bias.21 We are unaware of other qualitative studies that have explored drivers affecting a physician’s decision to leave practice after their departure from a large, multispecialty ambulatory practice network. Postdeparture interviews could be a more reliable approach—given that interview responses no longer affect employment and individuals may provide more unfiltered feedback. Our qualitative approach allowed identification of a broad set of themes beyond those defined a priori by the investigators. To our knowledge, this study is the most comprehensive and up-to-date report on reasons why ambulatory physicians voluntarily depart their practice with updates from previous studies that account for more recent stressors in delivery systems including EHR adoption and the COVID-19 pandemic.
Despite the relatively low turnover rate of approximately 5% per year in the practice network being studied, the findings presented here offer an opportunity for a learning health system approach32 to understand and mitigate physician departures. Furthermore, the findings offer a more comprehensive array of themes that may be contributing to troubling national trends in burnout that may be intervenable before departure.10,11
Successful interventions that aim to address factors identified in this analysis could help retain physicians in practice. Themes within the domain of local practice culture present opportunities for practice leaders to increase their visibility and presence in the clinical environment, increase opportunities for physician recognition, development, and advancement, distribute responsibility across team members, and ensure adequate staffing across disciplines and roles. The EHR can also be optimized, better training and technical support can be offered, inbox burden can be distributed to other team members, and scribes can offload documentation burden. Themes in the business of medicine domain have implications for policy makers to consider alternative care or payment models that deemphasize metrics and documentation burden.
Future research on physician turnover should work to quantify which factors identified in this study have the greatest influence on actual turnover. Doing so could help identify and retain physicians at high risk for departure. In this capacity, quantitative analysis in the same cohort presented here suggests nonlinear interactions exist between physician tenure, EHR use patterns, and departure.33 Future research should also prioritize factors that are more modifiable and, therefore, amenable to intervention. For example, personal considerations may weigh heavily on an individual physician’s decision to depart but may not be something that practice leaders can address. Although frequency of themes should not be used to determine theme importance, it warrants mentioning that workplace design and resources to support wellness were not mentioned frequently by participants. This could indicate that practice leaders seeking to retain their physician workforce should prioritize leadership visibility, staffing, and advancement opportunities over “wellness programs” and aesthetic office design.
This study is subject to several limitations regarding its approach, generalizability, and potential for bias. As with all qualitative research, the number of times that a theme arises does not indicate that theme’s relative importance. For example, although EHR use was the most frequently cited theme as a contributor to departure, none of the participants listed the EHR as their primary reason for departure. Because the study was performed in a single practice network, it may not be generalizable. Although we reached thematic saturation, willingness to participate in this study could present participation bias with an inability to capture reasons for departure among nonparticipants. Participants had little racial and ethnic diversity, suggesting that our findings are likely subject to representative bias. Physicians from underrepresented racial and ethnic groups may depart their practice for reasons not identified in this study.
Conclusions
Physician turnover is influenced by factors at the societal, local, and individual levels. As COVID-19 transitions from pandemic to endemic, all industries and professions are facing the effects of the Great Resignation. Given the disruption physician turnover causes to patients, physicians, and the practices they leave, understanding factors that contribute to physician turnover is a critical first step to retaining the physician workforce at a local level.


Notes
This article was externally peer reviewed.
Funding: This work was supported by an American Medical Association (AMA) Practice Transformation Initiative (contract No 16118). Dr. Melnick reports receiving grants from the National Institute on Drug Abuse and Agency for Healthcare Research and Quality outside the submitted work.
Conflict of interest: The authors have no conflicts of interest to disclose.
To see this article online, please go to: http://jabfm.org/content/36/6/1050.full.
- Received for publication February 15, 2023.
- Revision received March 21, 2023.
- Revision received May 24, 2023.
- Accepted for publication June 12, 2023.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.