
Abstract
Background: With increasing prevalence of opioid use disorders (OUDs) there is an urgent need for OUD trained front line primary care providers (PCPs) who can help improve patient adherence to addiction treatment. Unfortunately, most physicians have had limited training for treating patients with addiction, leaving clinicians under prepared. To address this need, we created a Medication-Assisted Treatment (MAT) training program specifically designed for PCPs.
Intervention: A 4-hour PCP focused buprenorphine office-based implementation training was designed to supplement the 8-hour SAMHSA DATA 2000 waiver training. The intent of the supplemental training is to increase PCP likelihood of implementing MAT through practical evidenced-based implementation, addressing barriers reported by waivered PCPs.
Methods: We developed and validated a new pre- and postsurvey instrument that assesses changes in participants knowledge, skills, and attitudes. Data were entered into REDCap, and composite scales were created and analyzed to determine pre–post differences.
Results: A total of 183 participants completed pre–post evaluations. Pre–post comparisons indicated substantial improvement in learner levels of confidence in implementing MAT care processes and in their interactions with MAT patients (df = 4, F = 203.518, P < .001). Participants described themselves as more comfortable identifying patients who would benefit from MAT (t = 15.04, P < .001), more competent in implementing MAT (t = 21.27, P < .001) and more willing (t = 15.56, P < .001) to implement MAT after training.
Conclusion: Evidence suggests that a new MAT training program that supplements the SAMHSA waiver training increases confidence and willingness to implement MAT among PCPs. Efforts to replicate this success to allow for further generalization and policy recommendations are warranted.
Introduction
According to the US Center for Disease Control, 91,799 drug overdose deaths occurred in the United States in 2020. The age-adjusted rate of overdose deaths increased by 31% from 2019 to 2020 (21.6 to 28.3 per 100,000)1 The age-adjusted rate of deaths involving synthetic opioids, excluding methadone, increased 1040% from 2013 to 2019.2 The availability and potency of synthetic drugs, frequently combined with other substances, has resulted in a public epidemic characterized by overdose and death.
The epidemic is widespread geographically and spans all generations. According to the US Surgeon General, only 54.9% of those aged 12 and older with heroin use disorder received treatment for illicit drug use at a specialty treatment facility. Only 28.6% of those aged 12 and older with an OUD in the past year received treatment for illicit drug use at a specialty treatment facility.3 Tong and colleagues found that only 22% of Americans who are using heroin or are misusing prescription painkillers can access treatment.4 To tackle this problem, the primary care (PC) workforce needs to be involved in treating people with OUD.4 Patients requesting care from their primary care provider (PCP) often present with a chief complaint of physical illness, however, data suggest that there is frequently an underlying mental health or substance use issue triggering the visit. PCPs can sustain trusting relationships with patients that are supportive to patients with addictions, including OUD. 2,5⇓–7
The only feasible means of reaching and treating all patients with addiction is to make addiction screening, intervention, and treatment available in primary care, which motivated the US Health Resources and Services Administration and other federal agencies to aggressively launch training grants and incentive programs targeting PCPs with prescribing privileges. However, there are several barriers, perceived and tangible, to implementation. In an editorial on adding medication-assisted treatment of patients with OUD, Dr. Richard Hill, reflecting a prevailing opinion among family physicians, “cautioned that primary care physicians should be wary of taking on yet another complex patient population.”8 Despite an increasing number of clinicians who are waivered to prescribe buprenorphine, only 3.6% of family medicine physicians in the nation have this certification.5 According to the National Institute on Drug Abuse (NIDA), in 2011, there was an estimated treatment gap of 19.3 million patients with addiction in need of medical treatment with those in need.9 Therefore PCPs play an essential role in treating people with substance use disorder.
Building PCP engagement in combatting OUD requires more than just teaching how to use the medicine (buprenorphine) and helping them secure the permission to prescribe it (applying for the X-waiver). In this article, we will discuss the process for developing an intervention that builds a sense of urgency to change and demonstrates feasibility and prosperity for PCPs.
Background
In 2016, Northeast Ohio Medical University (NEOMED), in partnership with MetroHealth in Cleveland, received a 5-year grant from the US Health Resources and Services Administration (HRSA) to implement a Primary Care Training and Enhancement (PCTE) project. With these funds MetroHealth and NEOMED developed Primary Care Transformation Fellowships, with a desire to achieve the Quadruple Aim in medical education.10 Unexpectedly, during the grant period in both 2016 and 2017, Ohio ranked second in the United States for drug overdose mortality.5 As a result of the national opioid crisis, HRSA provided supplemental PCTE funding to NEOMED and MetroHealth to provide Substance Abuse and Mental Health Services Administration (SAMHSA)-sponsored Medication-Assisted Treatment (MAT) training for Primary Care Transformation Fellowship participants to address the opioid crisis. It quickly became clear to the NEOMED and MetroHealth program administrators that the SAMHSA sponsored MAT certification training, although excellent for teaching OUD treatment, was not enough to ensure PCPs confidence and expertise in implementing MAT in their practices. From 2017 until 2018, NEOMED and MetroHealth examined barriers to MAT implementation in PC and developed a 4-hour supplemental program to the SAMHSA MAT certification training. This program sought to address the barriers to program implementation and improve PCPs confidence and capability to implement MAT in primary care practices.
Methods
Study Design
This was a multi-site, 4 phase, educational program evaluation in which (1) a supplemental MAT educational program was developed, (2) a new survey measurement tool was developed and tested to assess the goals of the program, (3) the new program was implemented, and (4) the program was evaluated using the new measurement tool. The evaluation study was conducted after review and approval by MetroHealth and NEOMED Institutional Review Boards. NEOMED and MetroHealth seek to improve access to quality opioid and other substance abuse disorder treatment and prevention by increasing the number of clinicians trained to deliver these services, including interdisciplinary primary care providers (PCPs: physicians, physician assistants [PAs], nurse practitioners [NPs]) and residents). Goals of this supplemental program included: successfully identifying substance use disorders, offering patient support during MAT, and administering MAT to help patients achieve a better quality of life. In the end, clinicians will understand how their care teams may influence reduction in opiate harm across patient groups and in broader communities.
Participants
In this project, 203 participants were initially recruited from 11 partner health systems affiliated with the medical school, 2 area federally qualified health centers, and 2 nearby universities with physician assistant and advanced practice nursing training programs, respectively. Senior faculty at these organizations were already collaborating with the medical school on the HRSA-sponsored Primary Care Transformation Fellowship, and they were encouraged to share the training opportunity with other faculty, alumni, and colleagues. We were also able to leverage 3 regional professional conferences that took place nearby and were allowed to share the information with PCPs in attendance. Supplemental grant funds enabled us to pay practicing clinicians up to $1000 for time in training, as well as CME credit at no cost to them. Trainees (resident physicians) were not permitted to receive compensation, per federal sponsor grant restrictions. Participation was voluntary, and all participants at the NEOMED trainings responded individually to program announcements. Clinicians and resident physicians at the hospital trainings had training time built into their schedule.
From February 2018 to June 2019, we offered 10 total training sessions (occurring at 7 Northeast Ohio sites) that were attended. Participants included physician clinical faculty, resident physicians, physician assistants and nurse practitioners from NEOMED, MetroHealth, and partner hospitals, universities, and Federally Qualified Health Centers (FQHCs). Those who completed the training and had a license to prescribe controlled substances were eligible to apply for the DATA 2000 waiver to administer MAT. Of the training participants, 37 did not yet have a DEA number. Learners who did not complete pretest evaluations (n = 2) or posttest evaluations (n = 13) were excluded from our evaluation analysis; the total response rate for the evaluation survey was 92.6%.
Educational Intervention
HRSA funds were used for both faculty and resident training in OUD diagnosis, prevention, and treatment, emphasizing MAT. Training focused on prevention, screening and assessing patients for OUD, treating patients with OUD, including managing the disease in the context of other health conditions, connecting patients to appropriate community services, identifying patients at high risk of overdose, and emergency treatment of patients who have overdosed. Under the direction of a lead trainer, an addiction psychiatrist certified by the American Academy of Addiction Psychiatry (AAAP), training included the latest clinical guidelines, such as the Centers for Disease Control and Prevention (CDC) guidelines for prescribing opioids for chronic pain5 and the Providers Clinical Support System (PCSS) tools for patient engagement and clinician support. We incorporated resources available to trainees through governmental resources such as SAMHSA and the Bureau of Primary Health Care.
Training Schedule
PCPs in year 1 completed the 8-hour training on a Saturday on NEOMED’s campus. The first 4 hours was spent on the live portion of the AAAP Half-and-Half Course, and the second 4 hours was spent on the PCP Supplemental Training described in detail in the next section and Appendix 1. Each clinician was given 30 days from the original training date to complete the remaining 4 hours of the DATA 2000 Waiver Training online.
In year 2, 7 family medicine program directors who completed the Saturday program asked for their faculty and resident physicians to be trained. We agreed and hosted the program at 6 hospital locations (2 nearby hospitals in 1 health system trained together) in Northeast Ohio. The program content and delivery were consistent with the NEOMED-based program. Faculty and residents covering the practice when colleagues were in training had either already taken the course or had the option to attend the education session at another hospital, or at NEOMED. To ensure that this training meets the needs of PCPs, NEOMED and MetroHealth developed and β-tested a new evaluation tool (Appendix 2) to assess changes in knowledge, skills, and attitudes as a result of the training, as well as PCP intent to implement MAT into primary care education and practice. Analyses provide a regional view of success for Northeast Ohio.
To sustain the activities after the funding period ended, program participants received the SAMHSA Treatment Improvement Protocol 63: Medications for Opiate Use Disorder reference to help implement MAT at their sites and to complement what faculty and residents learn during MAT training and certification.11 MAT experts are available for ongoing program consultation, clinical consultation, and training to participants while they incorporate the content in their practices.
Supplement to AAAP Training
The supplemental training was designed and delivered by subject matter experts in (1) primary care implementation, (2) addiction medicine, and (3) motivational interviewing (see Appendix 1) to address perceived barriers to primary care implementation. We conducted an evaluation of the supplemental training, understanding that all who completed the evaluation would have completed a minimum of 4 hours of DATA 2000 X waiver training in advance of the intervention. Participants submitted the pretest in advance of the lunch break, following the first 4 hours of waiver training and before the supplemental training, and the posttest at the end of the training day with their compensation paperwork (see Appendix 2).
Supplemental Training Module 1: Office-Based Treatment with Buprenorphine (1 Hour)
During the first hour, a primary care physician and champion of MAT provided practical advice on choosing appropriate patients, following state regulations, and managing office workflows related to MAT. She also provided information about the (1) Centers for Medicare and Medicaid Services Merit-based Incentive Payment System (MIPS) measures related to Opioid Use Disorder (OUD), (2) safety and effectiveness of OUD medications, and (3) adherence to OUD treatment as a measure of quality of care in the clinical practice setting. Importantly, she also provided a personal narrative illustrating how adding MAT to her practice increased patient satisfaction and her own joy in practicing medicine. Finally, she personally invited each participant to visit her office and observe MAT implementation in real time.
Supplemental Training Module 2: Philosophy of Care and Addiction as a Brain Disease (1 Hour)
During the second hour, an addiction medicine specialist spoke about treating addiction as a chronic relapsing brain disease and led a group discussion about the implications of different philosophies of care (“abstinence-based” vs “harm reduction” approaches) in the delivery of MAT. The concept of addiction as a chronic disease was introduced along with a discussion of how philosophies of care (“abstinence-based” vs “harm reduction”) impacted the implementation and delivery of MAT. The training reviewed 5 explanatory models of addiction, including moral, spiritual, psychological, behavioral, and medical. The medical model of addiction emphasizes dopamine dysregulation in brain reward pathways leading to symptoms such as drug craving, tolerance, withdrawal, loss of control over substance use, and impaired judgment.12 Relapse to drug use is not considered a “treatment failure,” but rather an expected part of having a chronic condition.13 Just as an individual with diabetes may experience fluctuations in blood sugar levels based on imperfect adherence to medication and lifestyle changes, an individual with addiction may return to old behaviors when triggered by physiologic or environmental cues.
An addiction treatment program’s philosophy of care can significantly impact how MAT is implemented and delivered. Treatment philosophy of care can be conceptualized on a continuum ranging from “abstinence-based” on 1 end to “harm reduction” on the other end. In a strictly “abstinence-based” program, patients receive medications contingent on attendance in group treatment, individual counseling, and mutual help meetings. If a patient were to relapse, consequences might include taper and discontinuation of medication or discharge from the program. In contrast, a purely “harm reduction” program would seek to individualize psychosocial treatment based on patient preference, and medication would not be withheld based on adherence patterns to group or individual treatment. A patient with “unexpected urine drug screen results” would receive additional support and increased intensity of treatment services rather than discontinuation of medication or discharge from the program.
Supplemental Training Module 3: Motivational Interviewing (2 Hours)
The third and fourth hours of supplemental training were delivered by a professor with PhD expertise in addiction treatment and motivational interviewing (MI). This speaker emphasized how MI principles and strategies could be used to engage patients in their own care and how clinicians could manage difficult situations such as unexpected drug screen results and opioid use relapses. Training incorporated an introduction to motivational interviewing (MI) in an office-based opioid treatment setting (OBOT). MI is an evidence-based, collaborative, person centered, guiding conversation style to strengthen a person’s own motivation to change.14 Based on the third edition of Motivational Interviewing: Helping People Change, the introductory 2-hour training covered the underlying “spirit,” core skills and strategies of MI.15 The training involved OBOT specific examples of how MI skills and strategies may enhance patient outcomes. Participants engaged in learning through a blend of observation, written materials, experiential exercises, and practice opportunities. For example, after watching a live MI demonstration with a typical OBOT scenario, participants were invited to practice MI skills in dyads using “real-plays” from their own experiences with behavior change.
There is extensive evidence of efficacy for MI from controlled trials in substance use disorders and specifically for OUDs.16–23 In addition, Kim and Kalira argued that MI should be used throughout the shared decision-making process about MAT by establishing the foundation of an empowering and collaborative patient-clinician relationship, resolving ambivalence, bolstering patient actions, and promoting adherence to the treatment contract.24
Measures
Several researchers have developed instruments to evaluate clinician’s beliefs and attitudes about MAT.25 However, a review of the literature identified no instruments for evaluating clinicians’ attitudes about delivering specific aspects of buprenorphine treatment for OUDs. Prescriber attitudes toward delivering buprenorphine treatment for OUDs are likely to interact with both individual clinician differences (eg, confidence discussing medication effects and side effects with patients) and contextual factors (eg, organizational support). Our development of items and our approach to evaluation was informed primarily by social cognitive theory.25 A core component of this theoretical approach is the maxim that learning occurs in social contexts wherein the interaction between persons, their behaviors and the environment must be directly addressed. Self-efficacy and outcome expectancies are core elements of educational and health research, which have been demonstrated. Our measures were authored and designed to go beyond traditional approaches which focus on knowledge and achievement and focus on cognitively appraised barriers and self-efficacy.26 If the supplemental training can increase self-efficacy for integrating MAT into clinical practice among practitioners, practitioners will be more likely to implement MAT in their clinics. As a result, pre- and post- versions of MAT self-assessment scales were developed to evaluate prescribers’ individual- and contextual-level attitudes toward delivering MAT both before and on completion of MAT training, respectively.
In Step 1, study leadership developed a list of candidates to serve as experts in developing the evaluation tool. From a regional group of more than 20 candidates, an expert panel was selected and thus composed of a group of 2 physicians, an expert in psychometrics, an expert in postgraduate education and 2 persons experienced in substance use care delivery. In a series of meetings, the panel generated an initial set of concepts to be measured, authored a first draft of an item bank, examined the face validity of items and reconvened to conduct initial revisions after cognitive interviewing of a small sample of local participants. Panel review of face validity was structured: panel members received copies of an initial list proposed pre- and postinstruments and were asked to classify items as essential or irrelevant and to generate any other items that they considered to be necessary to explore MAT attitudes.
The panel reached a consensus on the items to be used in the instrument through successive rankings. The statements were then combined into pre and postinstruments with 3 distinct, 4-point Likert scales: (1 = not at all important; 4 = highly important); (1 = not at all confident; 4 = highly confident); and (1 = strongly disagree; 4 = strongly agree). The instrument included items that assess prescribers’ attitudes toward the importance of engaging in specific MAT practices and their confidence in engaging in these practices because importance and confidence are theorized to predict people’s motivation to engage in behavior change, such as deciding to deliver MAT to patients.27 The pre–post instruments share the same 26 items, though the postinstrument has an additional 11 items, which assess the specific impact of an educational intervention on attitude change. Our approach to pre–post assessment was informed by the retrospective approach described by McLeod et al27 and implemented in other upskilling, faculty development and postgraduate educational initiatives in health care settings.26–31
The initial MAT Self-Assessment item pool was administered to a population of PCP prescribers from Northeast Ohio enrolled in MAT training sessions hosted by NEOMED and MetroHealth. Participants’ responses to the instruments were analyzed.
Statistical Analysis
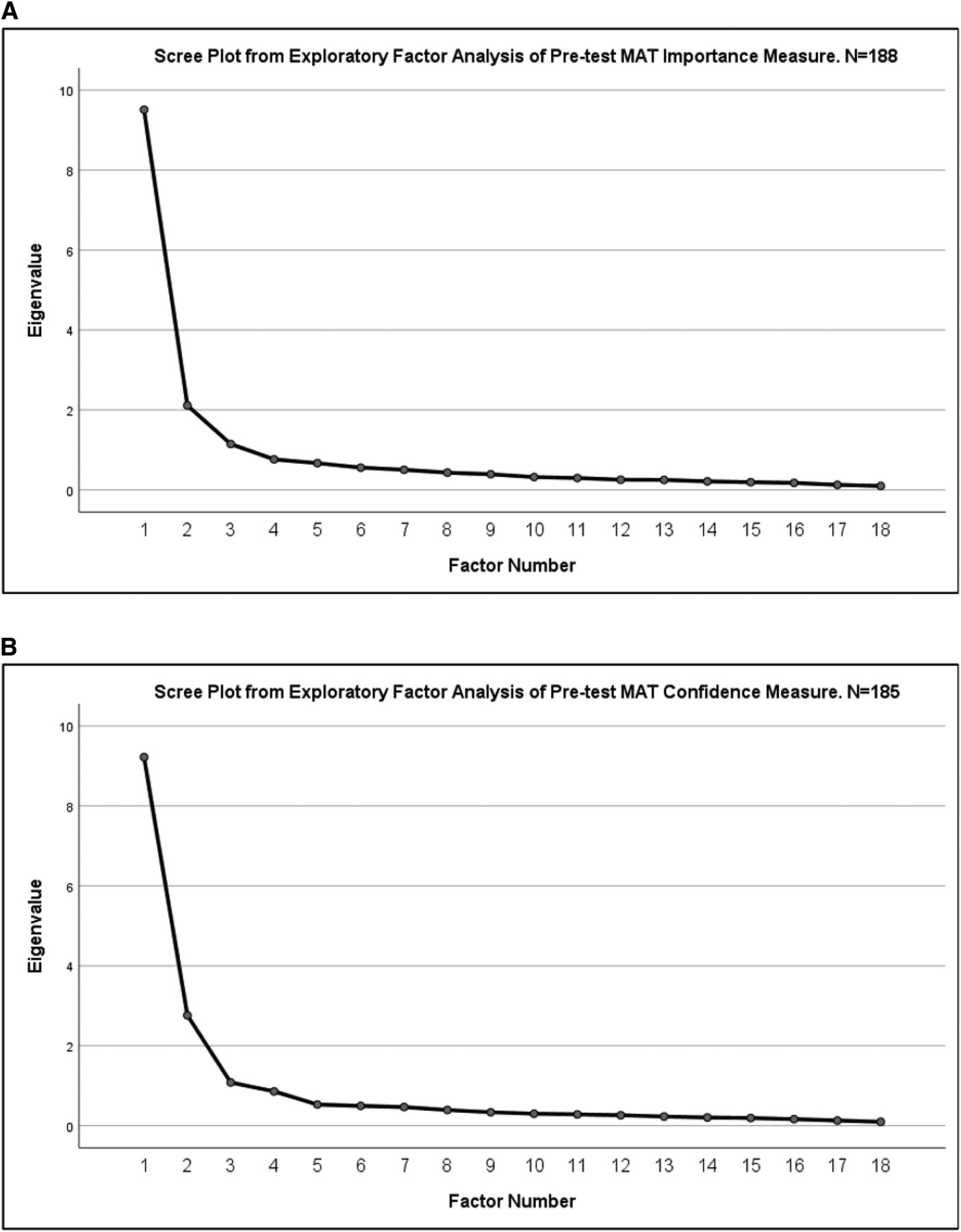
Data were initially subjected to detailed descriptive review and checking of statistical assumptions. Missing data were handled using listwise deletion. Due to our development of a new measure, the new survey tool was examined in 3 successive steps: (1) exploratory factor analysis (EFA), (2) reliability analysis, and (3) pre–post hypothesis testing. Data analyses were conducted using SPSS v.26 and AMOS v.2632,33 EFA analyses were conducted on the pretest data only. We utilized maximum likelihood estimation with promax rotation for solutions with between 1 and 4 factors on the 18 importance and 18 confidence items. Factor loadings were examined and items with primary factor loadings <0.40 and/or secondary loadings >0.30 were removed. Scree plots and eigenvalues were utilized to determine the number of factors.
We examined the hypotheses that training participants demonstrated an increase in self-ratings of importance and confidence in the 2 general competencies established by the EFA, CFA, and reliability analysis: MAT care process and patient interaction. We further assessed the extent that participants had changes in their level of 4 additional measures: Comfort in recognizing opioid misuse, comfort in identifying patients suitable for MAT, self-rated competence in implementing MAT and willingness to implement MAT. We estimated mean scores, 95% confidence intervals, and used a multivariate analysis of variance to test the hypothesis that composite scale scores improved between the pre and post assessments.
Results
Initial Validation of the MAT Self-Assessment Scale
Results of the exploratory factor analysis supported a 2-factor solution across both the importance and confidence sets of indicators. Scree plots are shown in Appendix Figures 1A and 1B. These results indicated that the 2-factor solution fit the data best and reflected a measurement structure that we described as care process and patient interaction factors. Six items had low primary loadings or high secondary loadings and were dropped from the analysis. Final estimates of EFA factor loadings of the resulting 2 scales of MAT Care Process and MAT Patient Interaction are shown in Table 1. Results of reliability analysis are presented in Table 2. All scales were found to be reliable, with Cronbach’s α >0.90.
Exploratory Factor Analysis Loadings for Medication-Assisted Treatment (MAT) Importance and Confidence Items
Reliability Analysis for Pre- and Post- MAT Training Evaluation Items (Cronbach’s α)
Effectiveness of Supplemental MAT Training
Pre–post analysis confirmed our hypothesis that participants would experience improvements in comfort in recognizing opioid misuse, comfort in identifying patients suitable for MAT, self-rated competence in implementing MAT, and willingness to implement MAT. The distributions of pre–post responses to these self-ratings are shown in Figure 2.

Pre–post comparison of willingness, comfort, and confidence with medication-assisted treatment (MAT).
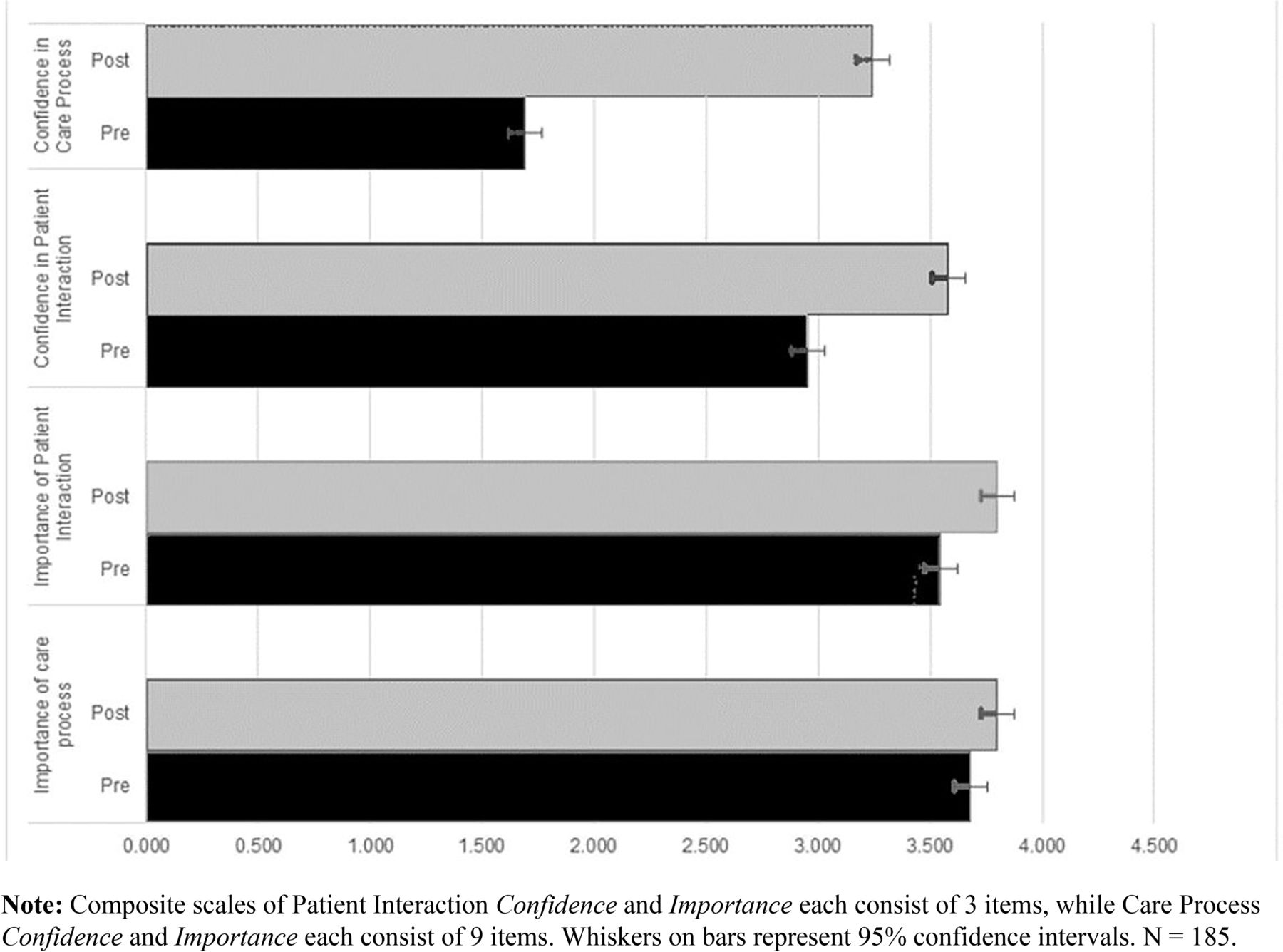
Pre–post comparison of importance and confidence items, care process and patient interactions.
Pre–post results for the newly created 4 composite scales (Importance of and Confidence in MAT Care Process and MAT Patient Interaction) are visualized in the clustered horizontal bar chart in Figure 2. Results indicate a large magnitude of increase in confidence in MAT care process, a small increase in confidence in patient interaction, and small increases in perceptions of importance of patient interaction and importance of care process. Multivariate analysis of variance results indicated that the within subject pre–post differences were statistically significant (Wilks λ = 0.180, df = 4, F = 203.518, P < .001). As expected, those areas with the lowest pretest scores had the largest magnitude of improvement.
Discussion
In this study, we demonstrated how to implement medication-assisted treatment of OUD into primary care practice. We (1) recruited PCPs to participate in training for MAT, (2) increased comfort and confidence in prescribing MAT and incorporating MAT into primary care practices, and (3) incorporated MAT education into 5 primary care residency training programs. Enhanced recruitment to MAT training programs was achieved by removing the pressure to apply for the X waiver, reimbursing PCP clinicians and medical educators for their time, and providing 12 hours of free continuing medical education credits. PCPs received critical MAT information and fulfilled qualifications to apply for the X waiver but were not required to do so to receive compensation for participating. In addition, the program included supplemental training on practice implementation of MAT for OUD delivered by a primary care physician champion and a motivational interviewing expert. Program graduates helped to recruit other colleagues to participate: 5 residency program directors who attended our training invited NEOMED to train their residents in MAT, and the PA faculty from a partner university hosted a special MAT program for PA students during their final year of training.
We conducted a follow-up of survey of clinicians who took the training to-date in 2018 (partially through the study period presented here) to assess who had implemented MAT into primary care practice. At the time of survey (n = 65, response rate 80%) 57% of trainees had implemented MAT into practice and another 19% had plans to do so with supporting evidence such as a colleague registered for an upcoming training, a shadowing appointment scheduled for hands-on training with one of the MAT presenters, signing up for the Ohio OUD ECHO distance learning program for new prescribers, or a pending proposal within the health system. Reasons for not (or not yet) implementing MAT included uncertainty of future practice location (particularly for resident physicians), disinterest from colleagues or other care team members, or uncertainty about legal consequences associated with treating patients with addiction. Even those who did not choose to prescribe found value in the training for patient education and referral purposes.
Limitations
Although the results clearly demonstrate our program gives PCPs the knowledge (SAMHSA 8-hour training), sense of importance and confidence (4-hour supplemental training), there are several limitations to the study. Our program was delivered in a single region, Northeast Ohio, and thus results might not be generalizable to clinicians from other parts of the United States. However, we included learners from multiple institutions, with varied levels of clinical experience so we expect that other training efforts would yield similarly positive results. Because no prior measurement tool existed for this type of study, we developed new evaluation questions, and used them for evaluation in a single study population. Our study has a moderately large sample size for a training program, the new measures are reliable, and we have made these available for use in future trainings in other settings. A major limitation of our approach is that our work was grant funded. Due to timing and funding limitations, we were unable to incorporate a comparative design, whereby some trainees received only the core MAT training and others both the core training and our supplemental training. Such a design could improve inference about the effectiveness of our approach, and our measurement tool is available freely for other researchers. Although the background literature indicated that PCPs with the core training, alone, were unlikely to prescribe buprenorphine. To continue to meet the need for primary care MAT training, we will need to develop sustainable models for offering the training program, perhaps by including MAT training and OUD treatment competency as a standard component of graduate medical education in primary care and by developing continuing education policies that further promote MAT training.
Next Steps
The next phase of this project will assess the impact of a hands-on clinical experience in addition to MAT plus PC supplemental training. A handful of participants in the MAT trainings have voluntarily completed a clinical experience with the family medicine presenter to obtain hands-on knowledge and comfort with practice implementation. We learned from the presenter leading the clinical experience, and confirmed with participating clinicians, that all PCPs who rotated at her MAT clinic following the classroom-based training discussed above have incorporated MAT into their primary care practice. NEOMED includes this hands-on experience with the CME training at our campus-based MAT clinic. NEOMED has secured a local foundation grant to support this training for current practitioners, and a federal SAMHSA grant to add this hands-on training component for medical students as part of a 3-year longitudinal OUD curriculum transformation. Given the increase in OUD use, overdose and death rising during the COVID-19 pandemic,34 new federal rules emerged allowing prescribers to treat a limited number of patients with buprenorphine without obtaining prescribed training or DATA 2000 waiver. Unfortunately, nonwaivered PCPs expressed negative attitudes toward providing MAT and, without training or another intervention, may continue to be resistant to treating OUD.8 The new guidelines allow X waiver physicians without training to treat up to 30 patients and up to 100 patients once they complete the Comprehensive Addiction and Recovery Act (CARA, X waiver) training. Now that the rules have been relaxed, further studies are needed to determine if PCPs with waiver training are more likely to treat OUD compared with PCPs without training.
Appendices.

Scree plots from exploratory factor analyses of pre-test medication-assisted treatment (MAT) importance and confidence measures.
Appendix 1
Appendix 2



Notes
This article was externally peer reviewed.
Funding: This project was supported by the Health Resources and Services Administration of the US Department of Health and Human Services Grant T0B30006.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/36/2/251.full.
- Received for publication August 15, 2022.
- Revision received November 21, 2022.
- Accepted for publication December 5, 2022.




{kind=link}
{kind=link}
{kind=link}