
Abstract
Background: Primary care physicians encounter many patients who present with lumps and bumps on their fingers, hands, and wrists. Some benign lesions including ganglion cysts, epidermal inclusion cysts, and giant cell tumors of the tendon sheath that are benign and can be managed by primary care clinicians most of the time in an outpatient setting.
Methods: We conducted a narrative of review of literature on the clinical presentation, diagnosis, prognosis, and management of common types of lumps and bumps found on the fingers, hand, and wrist.
Conclusions: Based on the literature review and our clinical practice, we provide indications for referral to plastic surgeons or other specialists for these lesions.
- Dupuytren’s Contracture
- Epidermal Inclusion Cysts
- Fingers, Ganglion Cysts
- Giant Cell Tumors
- Hand
- Outpatients
- Plastic Surgery
- Primary Health Care
- Wrist
Introduction
Primary care physicians often encounter hand tumors. Tumors of the hand commonly present as palpable lumps, and differential diagnoses may vary across different areas of the hand. The most common types of lumps and bumps found in the hand include ganglion cysts, giant cell tumors of the tendon sheath, and epidermal inclusion cysts. In this article, we share the clinical presentation, workup, and prognosis of common lumps and bumps of the fingers, hand, and wrist and provide practical guidance for primary care doctors in forming decisions to treat or refer patients who present with these conditions to hand surgeons.
Ganglion Cyst
Background
Ganglion cysts, the most common mass found in the hand, are benign tumors appearing commonly on the dorsal wrist (70%).1 They present as fluid-filled, translucent sacs with rubber-like consistency attached to the nearby tendon sheath or joint capsule.2 Figure 1 shows images of a ganglion cyst overlying the ulnar wrist. Although a history of arthritis or trauma may be associated with ganglion cyst,3 the pathophysiology of ganglion cysts is unclear. Symptomatic cases may present with radiating joint pain, decreased range of motion in the affected joint, or paresthesias from adjacent compressed nerves.4,5 Women aged between 20 and 40 are commonly affected.6

Ganglion cyst overlying the ulnar wrist; (A) Dorsal view, (B) Oblique view.
Diagnosis
Ganglion cysts are diagnosed based on certain clinical features. Patients usually present with an enlarging mass or painless focal swelling below the skin of the dorsum of the wrist or volar aspect of the wrist, most commonly on the radial aspect. On palpation masses are firm and immobile. Patients will often describe noticing the mass for months-years but secondary to fluctuating course (enlarges then decreases in size) they did not seek care. Transillumination will demonstrate translucency of the sac and differentiate ganglion cysts from lipomas.2 Imaging is infrequently indicated to diagnose a ganglion cyst; however, X-rays are often utilized to better assess the architecture of the underlying joint.7 X-rays can be of benefit especially with history of trauma or distal interphalangeal joint (DIPJ) location with osteoarthritic changes. Ultrasound and/or Magnetic Resonance Imaging (MRI) may aid the diagnosis in unusual clinical presentations, such as continuing increase in mass, persistent pain, or atypical mass location.8 Ultrasound may further support the diagnosis of ganglion cyst whereas MRI may help rule out malignant lesions.8
Treatment
There are three key levels of treatment for wrist ganglion cysts: reassurance, aspiration, or surgery.7 Reassurance is the first-line treatment option.8 Prescribing analgesics or joint immobilization could help mediate the discomfort from ganglion cysts.8 Physicians may aspirate the mass, but the recurrence rate can be >50%.7 Aspiration is performed with an 18 to 23 gauge needle and syringe due to the viscosity of joint fluid found within the ganglion. Aspiration should be performed with caution to avoid injury to neurovascular structures near the ganglion cyst. In recurring or symptomatic ganglion cysts, physicians may refer patients to a hand surgeon. Surgical removal of the mass by a hand surgeon can address the associated symptoms with a lower recurrence rate (30%).3,9
Digital Mucous Cyst
Background
Ganglions of the DIPJ are termed mucous cysts. They seem in the area between the DIPJ and proximal nail bed on the dorsal side of digits, the mucous cyst seen in Figure 2 is situated over the dorsal DIPJ.11 Mucous cysts can be associated with nailplate grooving if located closer to the eponychial fold proximal to the nailplate. Most cases have an asymptomatic course,12 but decline in the range of motion, pain, and tenderness of the affected joint may arise.11,13 Patients may describe lancing the mass with a clear-bloody viscous fluid that egresses. Patients frequently describe a fluctuating course with mass enlarging and then decreasing in size. The mass may erupt through the skin. Women aged 50 to 70 are most commonly affected.14

Digital mucous cyst between the distal interphalangeal joint and proximal nail bed.
Diagnosis
Superficial mucous cysts can be diagnosed without imaging.15 Key diagnostic features include a transilluminating mass and clear, viscous content on aspiration. Aspiration can be difficult for smaller mucous cysts or those that have decompressed.16,17 Differential diagnoses of mucous cysts include ganglion cyst, glomus tumors, and osteoarthritis.18 Radiograph examination should be performed for suspected mucous cyst as osteoarthritis of the underlying joint with joint space narrowing, subchondral sclerosis, and osteophyte formation is traditionally seen.12
Treatment
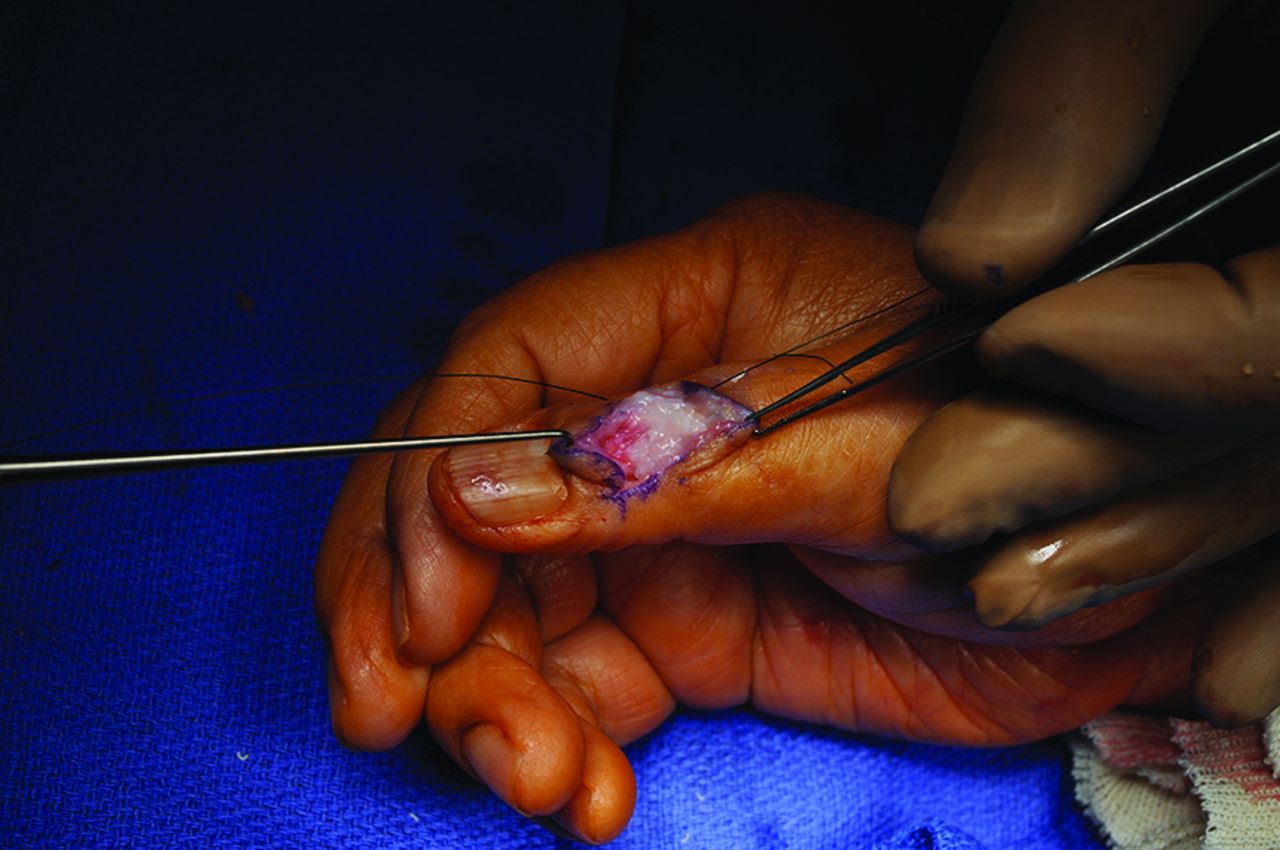
Observation is sufficient for asymptomatic cases.12 For symptomatic cases, surgical excision and removal of the underlying osteophytes is the most definitive treatment with a cure rate of 90%12,19 but joint stiffness and limited range of motion may arise.14,16 Patients may have persistent peri-incisional numbness. Figure 3 shows an intraoperative image of a digital mucous cyst excision the cyst is located on the ulnar side of the IP joint. Office-based treatment, such as puncture and expression of the cyst may achieve a cure rate of 70%.12,16 Steroid injection into the cyst after drainage can be performed but may have a recurrence rate of 40%.20

Intraoperative image of a mucous cyst excision procedure.
Referral
Because most cases of digital mucous cysts require no treatment or may be addressed in an office setting,12 referral may not be needed. However, referral to hand surgeons should be considered for patients whose diagnosis is uncertain, patients with significant symptoms, or those who request surgical removal.
Giant Cell Tendon Sheath Tumor
Background
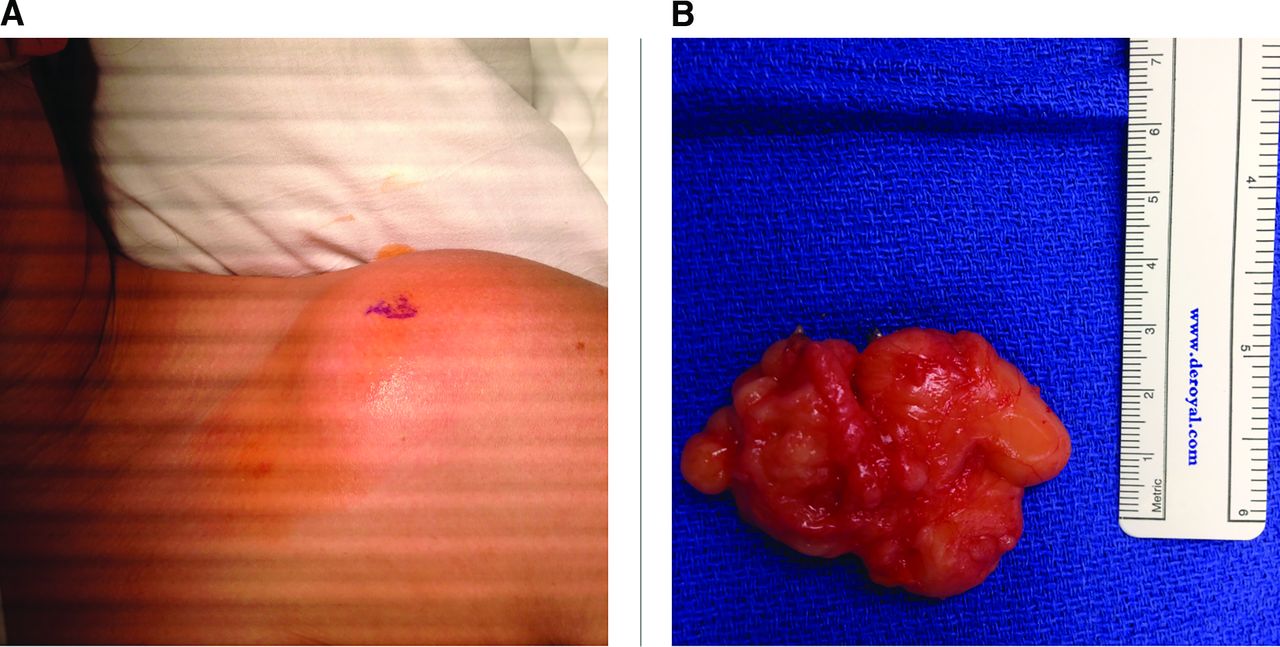
Giant cell tumor of the tendon sheath (GCTTS) is the second most common benign tumor in the hand.21,22 Whereas ganglion cysts are fluid-filled,8 GCTTSs present as solid, painless masses under the skin,23 frequently affecting women aged 30 to 50.24 Figure 4 shows a GCTTS located volar to the distal phalanx of the thumb. They seem tan-yellow intraoperatively and frequently extend to the tendon sheath and adjacent joints. Although these masses usually grow slowly, they frequently continue to enlarge unless excised. Although any joints of the hand can be affected by GCTTS, nodules most commonly seem on either dorsal or palmar side of the DIPJ.25 The etiology of GCTTS is still under discussion. Potential contributory factors include history of trauma, inflammation, neoplastic development, genetic aberrations, and metabolic syndrome.26–30

Giant cell tumor of the tendon sheath located in the distal phalanx of the thumb.
Diagnosis
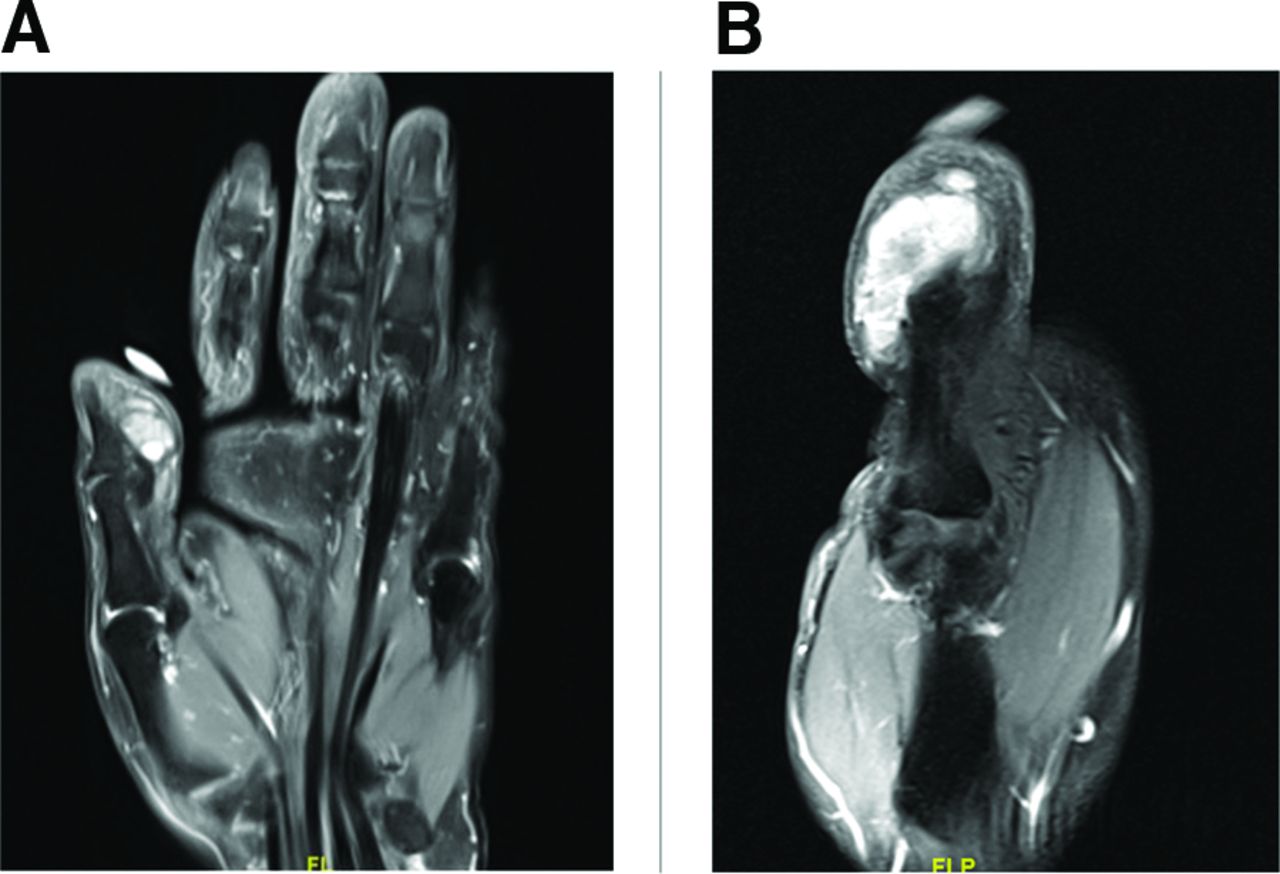
Imaging may assist in the diagnosis of GCTTS. On radiographs, GCTTS presents as a soft-tissue mass and may accompany pressure erosion or degenerative joint disease.25 Sonography and MRI are useful in characterizing the appearance of the soft tissue mass and may aid in the identification of satellite lesions.23 Figure 5 shows MRI images of a GCTTS volar to the distal phalanx of the thumb. Surgical pathology is used to confirm the diagnosis of GCTTS.31 Key histologic features include multinucleated giant cells, epithelioid histiocytes, mononuclear cells, xanthomatous cells, and hemosiderin deposits.31,32 Mitotic figures and apoptotic bodies may be present.31
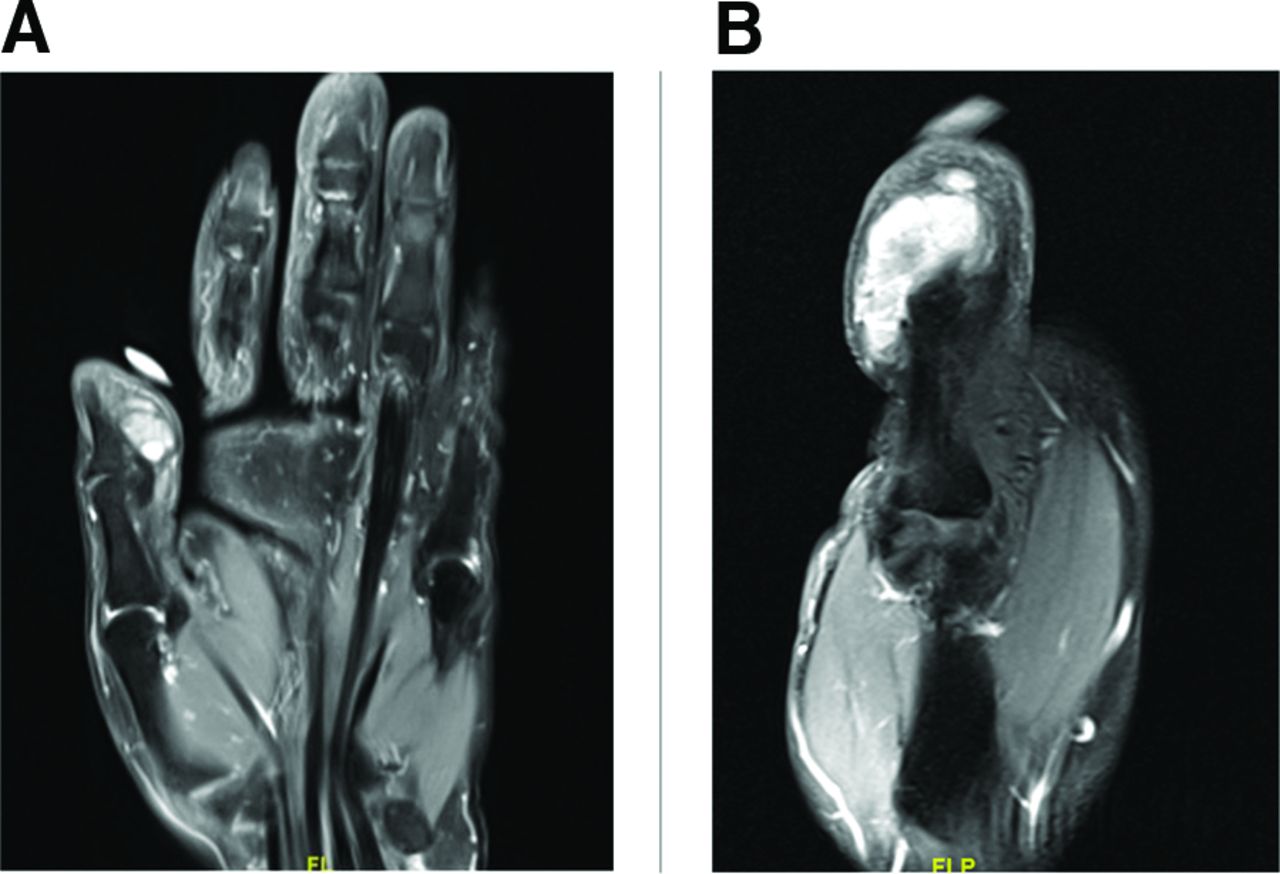
MRI images of a giant cell tumor of the tendon sheath located in the distal phalanx of the thumb.
Treatment
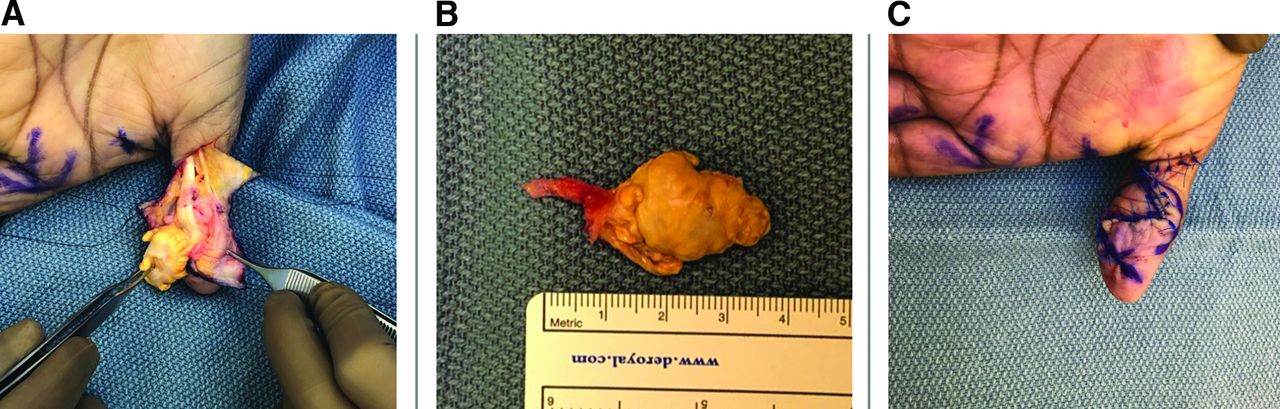
Complete local excision of the mass is recommended. Surgical excision can be difficult for locally invasive lesions. Patients may require radiation in select cases.25,33,34 Unfortunately, the recurrent rate of GCTTS is reported to about 15% on average32 (as high as 44%26). Figure 6 includes an intraoperative image of GCTTS excision (Figure 6A), excised mass (Figure 6B), and postoperative image of the skin closure (Figure 6C).

(A) Intraoperative image of a giant cell tumor of the tendon sheath located in the distal phalanx of the thumb (B) Excised mass; (C) Postoperative image of the thumb after the mass excision.
Referral
Referral to a hand surgeon should be considered for patients with suspected GCTTS.25 It is important for hand surgeons and primary care physicians to communicate the potential recurrence of GCTTS after surgery.
Epidermal Inclusion Cyst
Background
Epidermal inclusion cysts are slow-growing, keratin-filled cysts that may seem at any location under the skin including at the hand and finger.2 They are the most common cutaneous cyst35 and third most common soft-tissue tumor of the hand.3 Prior cutaneous trauma is associated with epidermal inclusion cysts.2,3 Men are more commonly affected than women.36 Although epidermal inclusion cysts can occur at any stage in life, they commonly occur in the third or fourth decades of life.37 Epidermal inclusion cysts are traditionally mobile and may present with a skin punctum over the mass.2 Although these cysts lack a neoplastic potential, they may continue to grow and be infected.2 Infected cysts may rupture but may resolve spontaneously.2
Diagnosis
The diagnosis of an epidermal inclusion cyst is made based on physical characteristics,35 including round subcutaneous mobile mass and central skin punctum.2,3 Among differential diagnoses, lipoma is one possible alternate for larger cysts.35 The central overlying skin punctum and firmness are helpful in differentiating epidermal inclusion cysts from lipomas.35 Patients may describe a history of squeezing the mass with a whitish thick material that egressed, potentially with a foul odor.
Treatment
Excision of the cyst and cyst wall is curative for epidermal inclusion cysts.2 However, treatment is only needed when requested by the patient as these are benign.35 Infected cysts may require antibiotics and incision and drainage. Inflamed or ruptured masses may recur sometimes.2,3,35 Intralesional injection of triamcinolone before excision may reduce inflammation.38 Primary care physicians may use the minimal excision technique described by Zuber, which does not require a total surgical excision or suture closure.39 Zuber’s technique involves the following steps: 1) Cleansing the overlying skin with povidone-iodine solution and anesthesia of the surrounding tissue with 2% lidocaine with epinephrine; 2) Stab incision to the center of the cyst and expressing the cystic content; a hemostat can be placed to keep the incision open; 3) After removing the cystic content, hemostat is used to pull the capsule out; 4) Application of antibiotic ointment and gauze over the procedure site; 5) Application of pressure by the patient for 2 hours after the procedure.39 Patients may request excision secondary to discomfort, history of infection, recurrence, or concern about appearance.
Referral
As most epidermal inclusion cysts do not require treatment, reassurance is a key treatment option. Different treatment options (ie, Zuber’s technique by the primary care physician vs referral to hand surgeon) should be considered for patients considering excision of the mass. Patients requesting hand surgery referral should be referred to a hand surgeon.
Lipoma
Background
Lipomas are benign tumors of adipocytes and the most common soft tissue tumor of the body.35 Lipomas commonly affect patients aged between 50 and 70.40 In the upper extremity, structures like the median nerve in the carpal tunnel and the ulnar nerve in Guyon’s canal may be compressed when lipomas grow large, leading to carpal tunnel syndrome or ulnar neuropathy.2,41 Subcutaneous lipomas are mobile, rubbery, and well-defined on palpation.2,35 In contrast, subfascial lipomas are often less mobile.2,35 Unlike ganglion cysts, lipomas are solid masses without translucency.2 In most cases, lipomas grow slowly over several years until the patients notice the mass or experience discomfort (ie, pain) from compression.2
Diagnosis
Key diagnostic features of lipomas include mobility, nontranslucency, softness and rubber-like texture.2,35 Figure 7 shows a lipoma overlying the left shoulder (Figure 7A) and the excised mass (Figure 7B). Differential diagnoses of lipomas include epidermal inclusion cyst, abscess, ganglion cyst, giant cell tendon sheath tumor, vascular malformation, and rarely liposarcoma.35 Epidermal inclusion cysts often have a central punctum of the overlying skin.2,3,35 Unlike lipomas, abscesses often are erythematous and painful and develop acutely.35 Liposarcomas often grow rapidly, are associated with pain, and are associated with larger size. Imaging such as ultrasound or MRI is helpful to delineate liposarcoma and diagnosis can be made with biopsy.42 Ultrasonography is helpful in differentiating lipomas from other benign conditions as well35,43,44 with a high sensitivity (86.9%) and specificity (96.0%) for superficial lipomas.44 However, the sensitivity of ultrasound in detecting deeper lipomas is lower.45

(A) Lipoma of the left shoulder; (B) Excised lipoma.
Treatment
Complete surgical excision is the mainstay treatment and has a low recurrence rate.2,41 Treatment is recommended for patients who experience functional or cosmetic impairment in the affected hand or those with concerning signs such as large size, rapid growth, and pain.2,35
Referral
Hand surgery referral for surgical excision should be considered for patients experiencing impaired hand function, are concerned about the appearance, or have rapid growth or other concerning signs/symptoms.
Dupuytren’s Disease
Background
Dupuytren’s contractures are secondary to palmar fibromatosis leading to contractures, most often of the ulnar digits but can affect any digit commonly at the metacarpophalangeal joints (MCPJs) and proximal interphalangeal joints (PIPJs).46 Prevalence of Dupuytren’s disease is higher among men aged 50 or older.47 70% of cases initially present to primary care physicians.48 The early phase of this condition presents with a small, firm, and painless nodule (Dupuytren’s nodule) on the palmar side of the hand most often over the ring metacarpal.46,49,50 Figure 8 shows a Dupuytren’s nodule proximal to the fifth digit (Figure 8A). In the later phase, starting from the location of nodules, the underlying palmar aponeurosis becomes thicker and fibrotic forming cords, curling the affected fingers into a flexed position,51 and may negatively affect daily activities and diminish quality of life.46,52 Figure 8B shows severe fibromatosis of the fourth and fifth digits in a patient with Dupuytren’s disease.

(A) Dupuytren’s nodule proximal to the fifth digit; (B) Dupuytren’s contracture at the fourth and fifth digits.
Diagnosis
Key diagnostic features include palmar nodules and palmar cords associated with digital cords.46,49 Differential diagnoses of Dupuytren’s contracture include flexor tenosynovitis and flexor tendonitis. Time of disease progression may vary, ranging from months to multiple years.46 As the disease may progress abruptly into the digital contracture phase, monitoring the progress of the disease with physical examination including the sites of nodules and worsening contractures, if present, of the affected joints is important.53 A positive Hueston Table Top Test demonstrated by patient’s inability to lay the affected hand flat prone on a flat surface is useful to stage the progression of Dupuytren’s contracture.53,54
Treatment
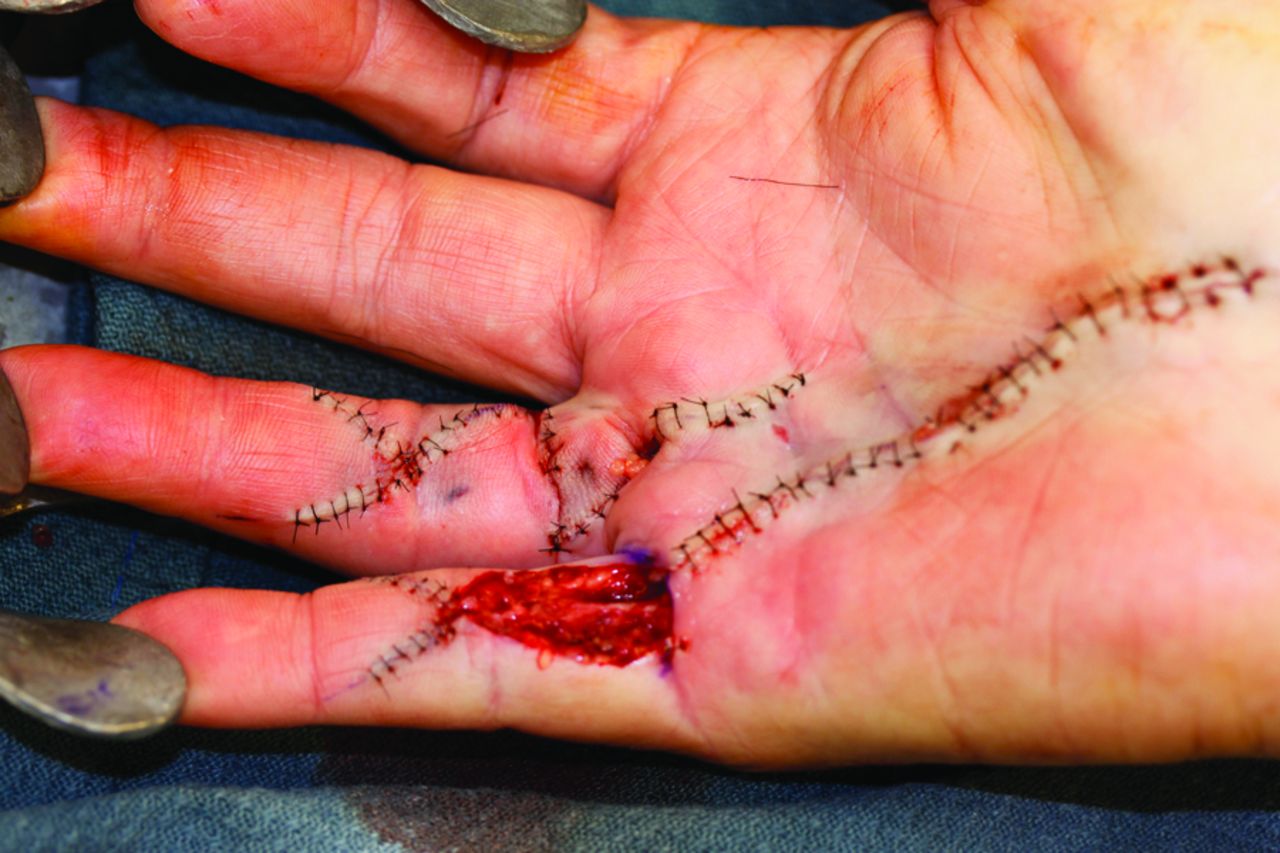
Patients without finger contractures require no treatment.46 A surgical release of the contracted joint is the mainstay of treating Dupuytren’s disease.46,50 Figure 9 is an intraoperative image of after surgical release of Dupuytren’s disease in the fourth and fifth digits with subsequent open wound of the fifth digit. Nonoperative treatment (ie, collagenase injections) can be considered if insurance authorization can be obtained. Collagenase clostridium histolyticum injections were reported to increase the range of motion in affected joints by reducing joint contractures in patients with Dupuytren’s disease.55 Collagenase injections are most helpful in patients with MCPJ contractures but can improve PIPJ contractures as well. As disease progression determines the timing of referral to hand surgery, regular follow-up for physical examination by primary care physicians is important.53

Intraoperative image of Dupuytren’s contracture release procedure.
Referral
Referral to a hand surgeon should be considered for patients with suspected Dupuytren’s disease if there is worsening hand contracture or compromised hand function in performing daily activities.53
Glomus Tumor
Background
Glomus tumors are benign tumors of the glomus body,56 a structure in the cutis that regulates blood flow, blood pressure, and temperature.57,58 The subungual region (under the nailbed) of the distal phalanx is the most common sites.59 Patients with glomus tumors may experience stabbing pain, tenderness and cold intolerance of the affected fingers.56 There are 2 subtypes of glomus tumors, solitary and multiple.60 Whereas solitary glomus tumors are more common and cause pain at the site of the mass in the digit, multiple glomus tumors are often painless, affect other parts of the body, and are associated with neurofibromatosis type 1.60 Although the etiology of glomus tumors is unclear, this condition is associated with aging, trauma, and family history.60 Women aged 20 to 40 are commonly affected.56
Diagnosis
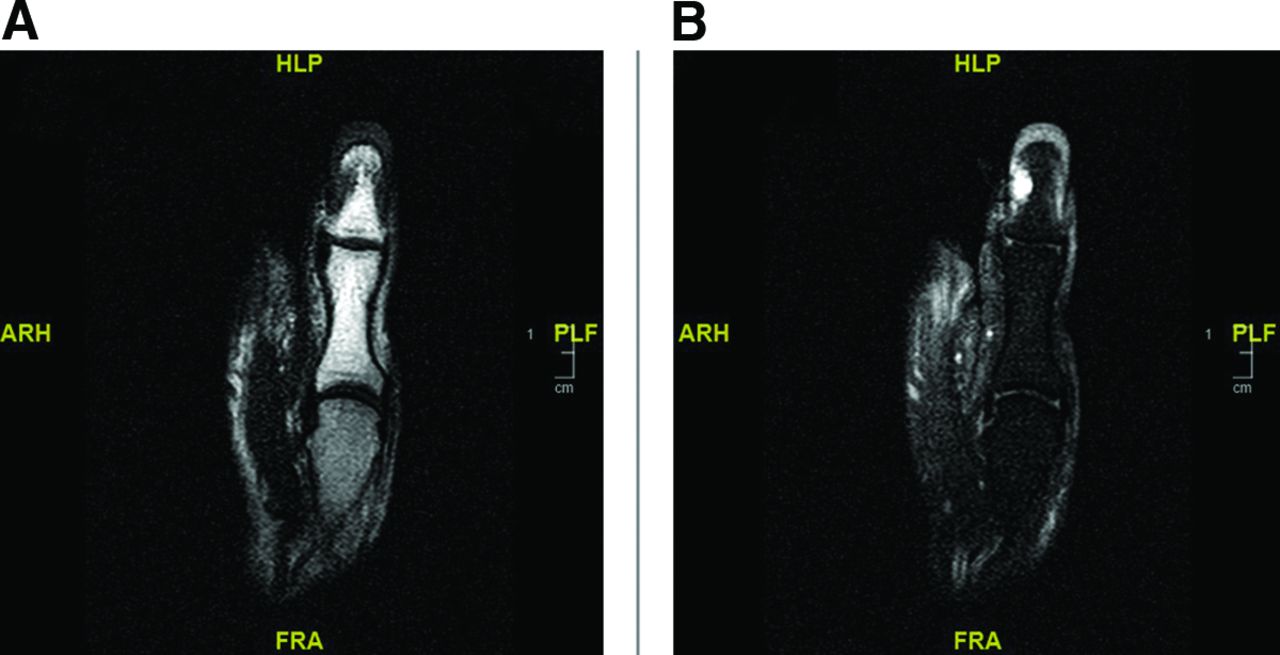
Diagnosing glomus tumors remains challenging as several other painful tumors may present similarly. Differential diagnoses of glomus tumor include hemangioma, neuroma, and leiomyoma.60 Key physical examinations for this condition include the Love’s pin test, Hildreth’s test, and cold-sensitivity test.60 The Love’s pin test (100% sensitive and specific)58 is positive when pressing the overlying skin with a pin head elicits exquisite pain.61 The Hildreth’s test (92% sensitive; 91% specific) is performed by introducing brief ischemia in the affected limb using a tourniquet; it is positive if there is reduction in pain with tourniquet inflated.62,63 The cold-sensitivity test (100% specific and sensitive)64 is positive if extreme pain is elicited with placing the affected digit into cold water.61 Highly suspected glomus tumors based on patient history and physical examination can be confirmed with MRI, ultrasonography, and histopathology.56,64 Figure 10 shows a T1-weighted MRI (Figure 10A) and a T1-weighted fat saturation MRI (Figure 10B) of a glomus tumor of the thumb. When the above exams are negative, other differential diagnoses (eg, neuroma, leiomyoma, hemangioma, epidermal inclusion cyst, foreign body, and gout) should be considered.56,60

(A) T1-weighted MRI image of a glomus tumor of the thumb; (B) T1-weighted fat saturation MRI image of the mass.
Treatment
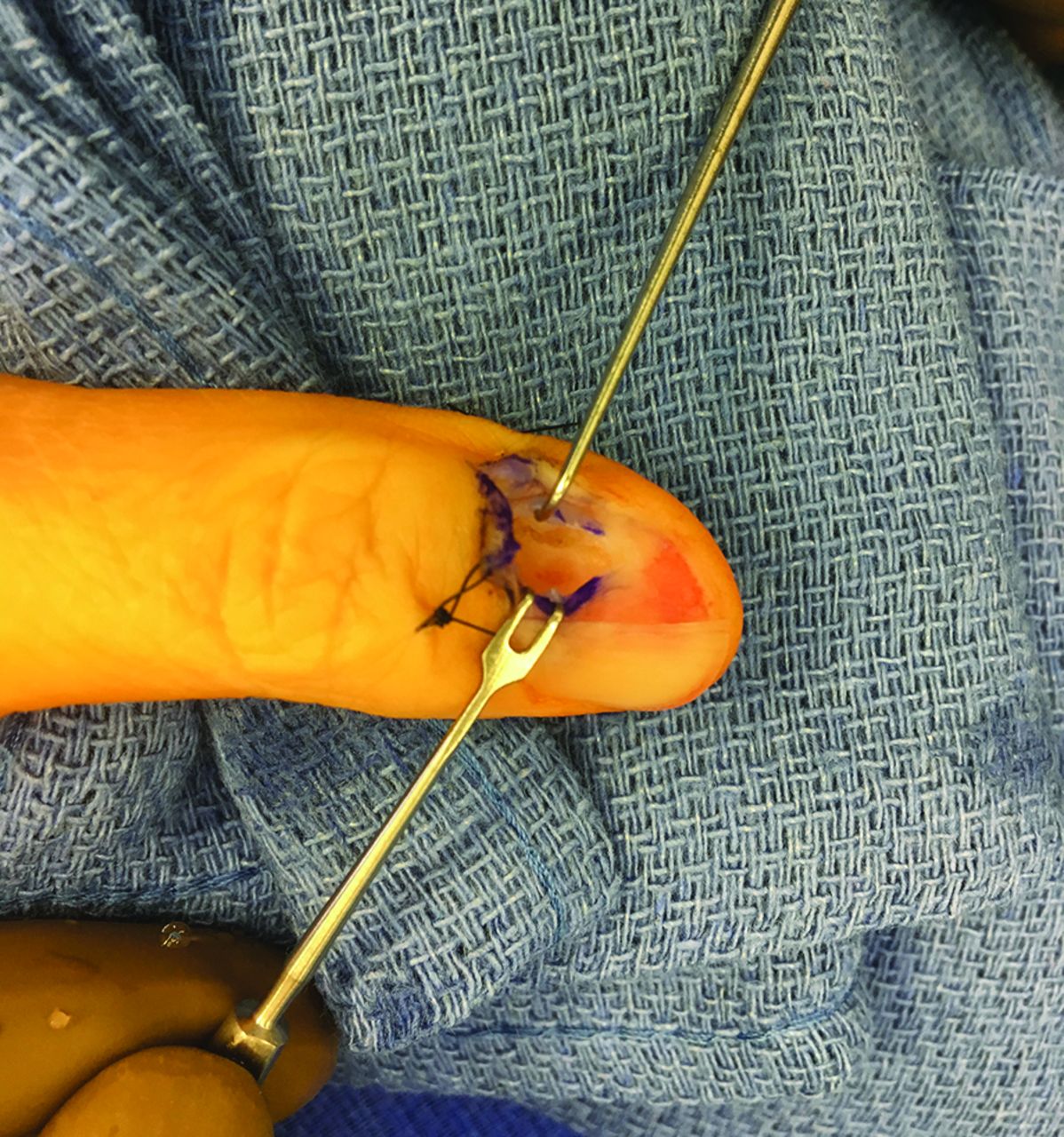
The standard of treatment for glomus tumors is complete surgical excision of the mass.64 Figure 11 shows an intraoperative image of glomus tumor excision. This often leads to permanent relief of the patient’s symptoms.56 Thus, primary care physicians’ role in making diagnosis and referring to hand surgery services is crucial.

Intraoperative image of excision of a glomus tumor of the thumb.
Referral
Once the diagnosis of glomus tumor is made, hand surgery referral for complete excision of the mass should be considered.64
Conclusion
Patients with lumps and bumps of the fingers, hand, and wrist frequently present initially to primary care physicians. Although most masses are benign and do not require treatment, malignant lesions need to be addressed immediately to prevent further complications of the disease.
Notes
This article was externally peer reviewed.
Funding: No funding was received for this work.
Conflict of interest: The authors report no conflicts of interest.
To see this article online, please go to: http://jabfm.org/content/35/6/1194.full.
- Received for publication January 26, 2022.
- Revision received February 20, 2022.
- Revision received May 24, 2022.
- Accepted for publication June 16, 2022.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}