
Abstract
Introduction: Increased screening efforts and the development of effective antiviral treatments have led to marked improvement in Hepatitis C (HCV) patient outcomes. However, many people in the US are believed to have undiagnosed HCV. Successful screening strategies and access to a coordinated system of care are critical for HCV affected adults. The objective of this study was to evaluate a primary care HCV screening education intervention that took place 2018 to 2019 to improve primary care training and management of patients after the implementation of the electronic medical record (EMR) screening alert.
Methods: Using 15 primary care practices located in vicinity of neighborhoods at-risk for higher rates of HCV infections, a stepped wedge randomized control study design was utilized to deliver an educational screening intervention. The education intervention was implemented sequentially with 5 practices being presented to every 3 months. Number of patients within the Baby Boomer cohort (birth years 1945–1965) were collected 3 months before the first practice receiving the intervention to 3 months after the last practice receiving the education intervention. The main outcome collected was the HCV screening. Generalized linear mixed models were used to test the hypothesis of improved screening rates after intervention implementation.
Results: There were a total of 85,697 patients within the Baby Boomer cohort seen at the 15 practices. Practices receiving the intervention had patients who were more likely to be screened for HCV (β = 0.259, P < .001; Odds Ratio [OR] [95%CI] 1.296 [1.098-1.529]).
In terms of demographics, results showed that females are less likely to be screened than males (β = −0.141, P < .001; OR [95%CI] 0.868[0.813 to 0.927]), Baby Boomer patients aged less than 65 were more likely to be screened than Baby Boomer patients aged 65 and older (β = 0.293, P < .001; OR [95%CI] 1.340[1.251 to 1.436]).
Discussion: This study looked at screening rates before and after an educational intervention which happened subsequent to the activation of an EMR alert. Whereas HCV EMR alerts showed an increase in HCV screenings before the education intervention, the addition of the education showed a modest increase in HCV screening rates for Baby Boomer patients.
- Early Medical Intervention
- Electronic Medical Record
- Hepatitis C
- Preventive Health Care
- Primary Health Care
- Screening Intervention
Introduction
Hepatitis C virus (HCV) infection is a disease that negatively impacts quality of life and results in premature mortality if left untreated. An estimated 4.1 million persons living in the United States are HCV antibody-positive and 2.4 million persons are HCV positive with active viral replication (1% prevalence among adults). Of those people with chronic HCV, 75% are unaware that they are infected.1⇓–3 Half of cases can be attributed to intravenous drug use. The rest of the cases result from sexual contact, birth mother to child, tattoos, intranasal drug use from shared paraphernalia, contaminated blood or transplants, and medical procedures.4⇓–6 Persons born between 1945 and 1965 in the “Baby Boomer” generation were likely infected between 1960 and 1980 and account for the majority of all chronic HCV infections in adults. The Baby Boomer generation is of interest because they represent more than 50% of newly identified cases in the past 10 years.7⇓–9 HCV patients experienced a 5 to 20% increased risk for liver cirrhosis due to delayed treatment, putting patients at high risk for additional complications such as hepatocellular carcinoma (HCC).10 In 2019, more than 14,000 people had HCV as an underlying cause of death.11 When this study was conducted, the Centers for Disease Control and Prevention (CDC) recommended all patients born between 1945 and 1965 be screened once for HCV. As of March 2020, the CDC began recommending a one-time HCV test for all adults age 18 to 79 to prevent HCV from spreading.12
The development of effective antiviral treatments along with increased screening efforts have led to improvements in HCV patient outcomes.10 Observational studies demonstrate a 40% reduction in HCC and liver failure in patients who achieve virologic cure along with reduction in mortality rates.13⇓⇓–16
Successful screening strategies and access to a coordinated system of care are critical for HCV affected adults.17,18 In May 2016, our large health care system implemented a one-time electronic medical record (EMR) alert for HCV screening for all patients born 1945–1965 who have no record of HCV antibody testing which resulted in a 17% absolute increase in screenings. A previous study also showing a 20% absolute increase in HCV screening when both HCV screening education and EMR alert activation took place at select practices took place during 2016. 19
The objective of this study was to evaluate a primary care HCV screening education intervention using a stepped wedge randomized control trial design that took place from 2018 to 2019 to improve primary care training and management of patients by augmenting clinician and staff behavior after the implementation of the EMR screening alert. This study looked at screening rates before and after an education intervention which happened subsequent to the activation of the EMR alert. We hypothesized that HCV screenings would increase after the education intervention was rolled out at 15 primary care practices.20 This stepped wedge design provides a more rigorous evaluation than a simple before and after intervention study which is scientifically flawed by confounding over time and does not include patients in a comparable control condition. The stepped wedge design eventually included all practices so therefore prevents contamination and disappointment effects in practices not randomized to the intervention parallel randomized parallel designs. 21,20
Setting
The study was conducted at Atrium Health, a large, vertically integrated health care system, based in Charlotte, North Carolina with > 200 primary care offices and more than 12 million patient encounters per year.
Methods
The Institutional Review Board deemed this project as quality improvement because all patients born between 1945 and 1965 were receiving the screening alert and the project did not include research development, testing and evaluation designed to develop generalizable knowledge. Previous research identified 15 primary care practices located in vicinity of neighborhoods at-risk for higher rates of HCV infections.22 The research team, consisting of researchers, primary care providers, hepatologists, and physician assistants who were experienced in managing and treating HCV, worked together to develop an education intervention. An education presentation was developed using existing information from a previous study in a PowerPoint format with a prerecorded voice-over. Education content consisted of who to screen, what to do with positive results, and when and how to refer HCV patients. The education also included specific information around the needs for newly diagnosed HCV patients such as the referral process, treatment, side effects of treatment, potential interactions with current prescriptions, required labs, and guidance on how to prepare patients for treatment visits with specialists. In addition, algorithms providing decision support were developed to guide primary care providers with patients whose lab test returned with a positive HCV. Both the Infectious Disease department and the Center for Liver Disease and Transplantation within our health care system provided content for the intervention input and patient care for HCV positive patients. The information provided to participating departments followed the guidelines for the referral process within our health care system and treatment guidelines based on the medication options at the time of the study.
The intervention was rolled out as a 1 hour lunch time meeting at the practice. A PowerPoint presentation with the prerecorded voiceover was presented at the lunchtime meeting by a nonclinical research team member, and then questions about the presentation were answered and/or followed up by the appropriate clinical department. If a practice declined to participate with an in-person lunch time meeting, the PowerPoint was emailed to the practice manager to be distributed to the providers to view when convenient. Because this education was not required, there was no attestation for providers to view the presentation.
Study Design
The study utilized a stepped wedge randomized control trial design (Figure 1). Each practice was randomly assigned to 3 groups and the education intervention was rolled out to 5 practices sequentially in 3-month intervals with the first 3 months used as a baseline. Practices were assigned randomly to wedges using a cluster randomization function in R. The evaluation consisted of data collection of patients within the Baby Boomer cohort across 4 time periods, (baseline and the 3 intervention rollout time periods) from July 1, 2018 to June 30, 2019. The education intervention was fully implemented by the end of the study, when all 15 practices receiving the education intervention, 5 in the first time period, 5 in the second time period, and 5 in the third time period.

Study design for 15 practices into 3 wedges.
The stepped wedge design was utilized to implement the intervention in a “phased, randomized roll-out,” where white cells indicate control time periods and gray cells indicate intervention time periods. Stepped wedge studies provide a more rigorous evaluation than a simple before/after study by: 1) allowing the research team and clinical teams to roll out the intervention in a timely, systematic manner, (2) increasing statistical power due to within and between cluster comparisons, (3) increasing clinical participation and leadership buy-in because all practices will eventually “flip” to the intervention, and (4) removing the confounding effects associated with time.20
Data Collection
Patient data without a previous HCV screening was collected from our enterprise data warehouse aligning within each time period. Within each of the 15 practices, only 1 visit per person per time period without a previous HCV screening was used for the denominator. If the patient received an HCV screening during that time period, the patient was excluded from future time periods. Patients who were already screened in the past were excluded from data collection as the EMR alert would not be activated for those patients.
Analysis
Generalized linear mixed models with a logit link were used to test the hypothesis of improved screening rates after intervention implementation controlling for random effects of practice location. The unit of analysis was any visit within the time frame where a patient was eligible for HCV screening (born between 1945 and 1965, no previous HCV diagnosis, no previous screening). The outcome of interest was HCV screening. The primary variable of interest was the education intervention (yes/no). To prevent misclassification bias, we coded the patient data based on the date of the intervention provided to each practice. All patients before the presentation date were coded as control and patients after the presentation date as intervention. Patient level factors associated with the likelihood of screening were also explored such as gender, race, age at the date of screening, and ethnicity.
Preliminary sample size analysis predicted we would need at least 300 eligible patients per period per practice to detect a 10% absolute improvement in screening rates assuming the current screening rate is 20% in the Baby Boomer population.23
Results
Table 1 shows the stepped wedge population by each wedge and time period. Rollout occurred at all 15 practices with 2 of the practices in time period 1, 4 in time period 2, and 2 in time period 3 that received an in-person presentation with the presentation emailed to the remaining 7 practices.
Stepped Wedge Study Design and Number of Patients Eligible for Hepatitis C virus (HCV) Screening
Patient Characteristics
A total of 85 697 patient visits were included in our analyses (Table 2). This exceeded the overall number of patients originally proposed to be included in the model. Patient demographics were reflective of the population born between 1945 and 1965. Patient age demographic were divided into patients aged less than 65 and patients aged 65 and older. Both the preintervention and postintervention had higher proportions of female patients. The racial diversity of all the patients in the control condition vs the intervention condition were 71% to 74% for white, 23% to 21% for African American, 3% to 3% for Hispanic/Latino, and 3.8% to 3.6% for other race.
Descriptive Statistics: Patient Population
Screening Results
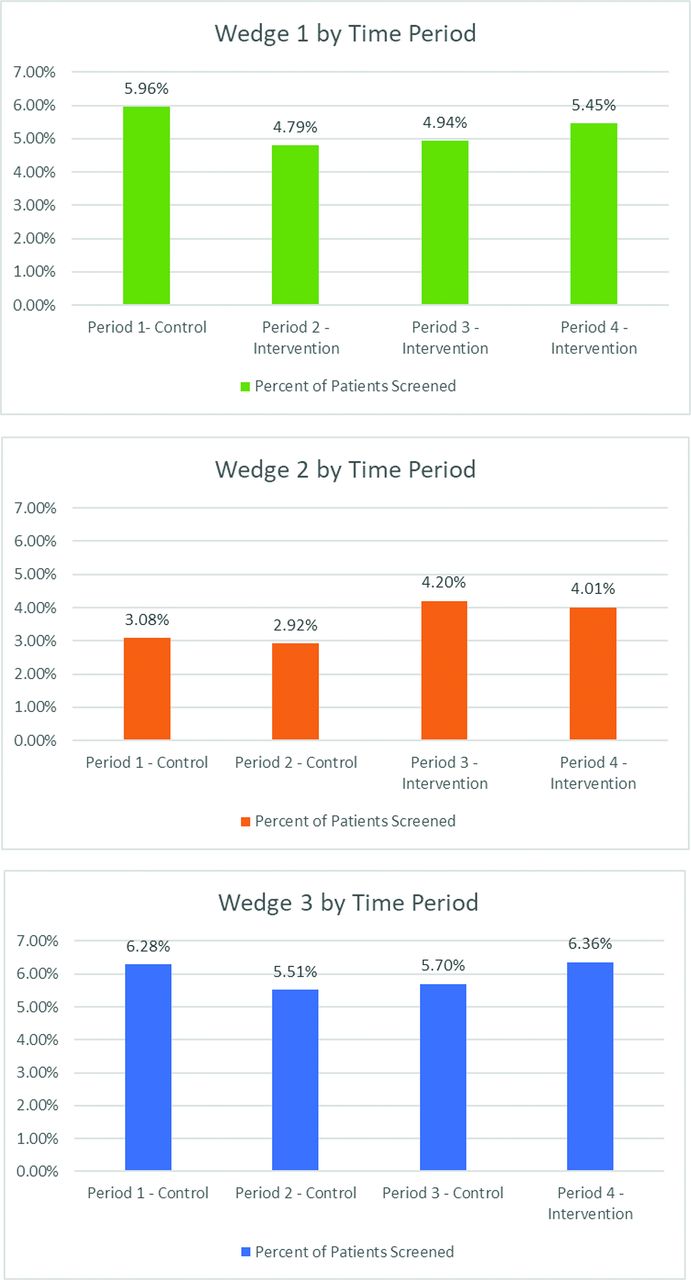
Figure 2 shows the screening rates at the 5 practices in each wedge and time period. Control periods were before the HCV education intervention and intervention periods are after the rollout of the HCV education intervention at the practice.

Incidence rate of patients screened for Hepatitis C virus (HCV) for each time period without any previous record of HCV screening. Each wedge consists of 5 practices and each time period consist of 3 months.
Results show patients born between 1945 and 1965 were more likely to be screened for HCV after their practice received the education intervention based on the interaction with an in-person presentation variable. (Table 3) (β = 0.259, P < .001; Odds Ratio [OR] [95%CI] 1.296 [1.098-1.529]).
Generalized Linear Mixed Model Results
In terms of demographics, results showed that females are less likely to be screened than males β =−0.141, P < .001; OR [95%CI] 0.868[0.813 to 0.927]), Baby Boomer patients aged less than 65 were more likely to be screened than Baby Boomer patients aged 65 and older (β = 0.293, P < .001; OR [95%CI] 1.340[1.251 to 1.436]).
Discussion
The education intervention presented at the 15 practices, highlighting the screening need for HCV for the Baby Boomer generation, resulted in a significant increase in screening rates between the control time periods and the intervention time periods. Although the increase was statistically significant in aggregate with an absolute change of 0.3% (from 4.4% for the control time periods to 4.7% (P < .001) for the intervention time periods), the absolute change observed did not meet the proposed absolute increase of 10% that would be clinically meaningful for the number of patients receiving the HCV screening. The number of screenings collected for this study far exceeded the requirement based on the power originally proposed. It is important to note that the practices evaluated here had previously experienced a 17% absolute increase in 2016 based on a health care system-wide EMR Baby Boomer HCV alert activation without an education intervention, that suggested that the 2016 alert activation successfully led to screening of a majority of eligible Baby Boomers before the start of this study. A previous study also showed a 20% absolute increase in HCV screening when both HCV screening education and EMR alert activation took place at select practices during 2016. 19 Similarly, in support of the effectiveness of combined HCV alert activation and education, a study conducted in 2016 at the University of Kansas Health System achieved a 15% absolute increase in patients screened for HCV after HCV alert activation.24 This absolute change increased to 25% when an education intervention was added shortly after.
Here, results indicated that younger Baby Boomers more likely to be screened that older Baby Boomers. There are a variety of reasons why this might have happened and further implementation evaluation research would need to be conducted to determine why this difference occurred.
Similarly, the results indicated that females were less likely to be screened than males. There are a variety of reasons why this might have happened and further implementation evaluation research would need to be conducted to determine why this difference occurred.
The results indicate that practices with in-person presentations had higher screening rates than those who did not opt for the in-person presentation. Further research incorporating implementation evaluation would provide additional explanation around those differences. Barriers to screening, practice engagement, and other workflow issues could be evaluated to determine why these practices had difference screening rates.
The results indicate that Time Period 2 was different from the other time periods. There are a variety of reasons why this might have happened and further implementation evaluation research would need to be conducted to determine why this difference occurred.
These results and those from other studies suggest that a standalone EMR alert with additional education is effective at increasing screening rates for HCV. The education standalone intervention implemented in our health care system was likely less effective because of the previous impact of the Baby Boomer EMR alert activation.
Future Research
Because the United States Prevention Task Force is now recommending screening for all adults aged 18 to 79, future research should include the 18 to 79 age range as the variable in the logistic regression model.25 To distinguish the difference in age groups, subgroups could be analyzed such as 18 to 34, 35 to 49, and 50 to 79 capturing the nuances of each age-group and their current and past behaviors.
Limitations
Because we did not track who viewed the education presentation, we do not know exactly how many physicians received the education intervention.
Because practices were not stratified based on size, clinically relevant demographic characteristics such as race, ethnicity and gender are not balanced in control and intervention conditions which may result in biased conclusions.
This study looked at screening rates before and after an education intervention which happened subsequent to the activation of the EMR alert. Significant patient populations in these practices were already screened before the education intervention which reduced the ability to measure the effect of the education intervention.
This study data were obtained from one health care system and therefore cannot be generalized to the entire population who do not seek services within our health care system.
Conclusions
This study evaluated screening rates before and after an education intervention which happened subsequent to the activation of the EMR alert. Whereas HCV EMR alerts showed an increase in HCV screenings before the education intervention, the addition of the education showed a modest additional increase in HCV screenings rates for Baby Boomer patients.
Notes
This article was externally peer reviewed.
Funding: This study, IN-US-337-4324, is supported by Gilead, Sciences, Inc.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/35/5/990.full.
- Received for publication December 16, 2021.
- Revision received May 20, 2022.
- Accepted for publication May 26, 2022.




{kind=link}
{kind=link}