
Article Figures & Data
Figures
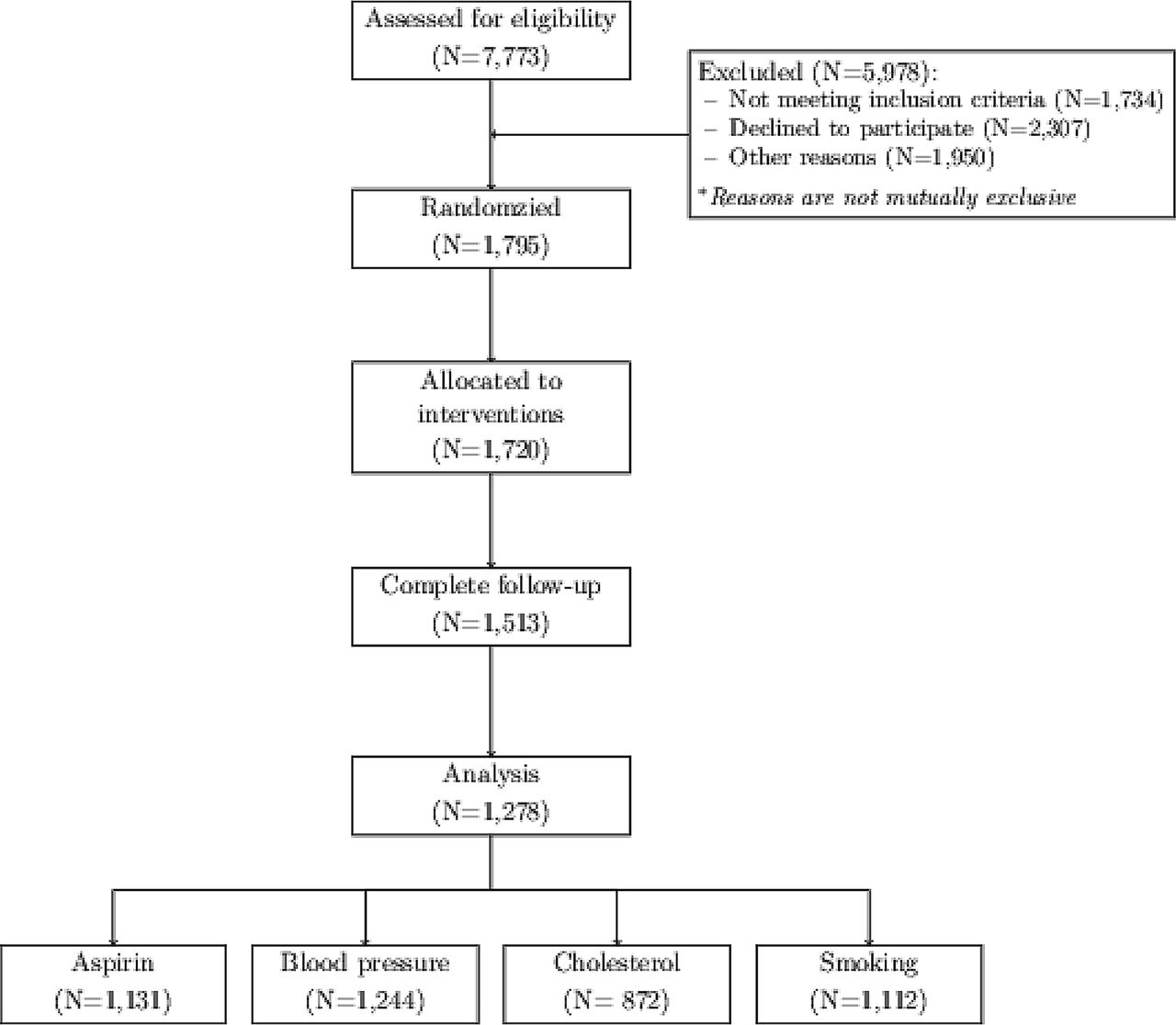
- Figure 1.
EvidenceNOW consort diagram.
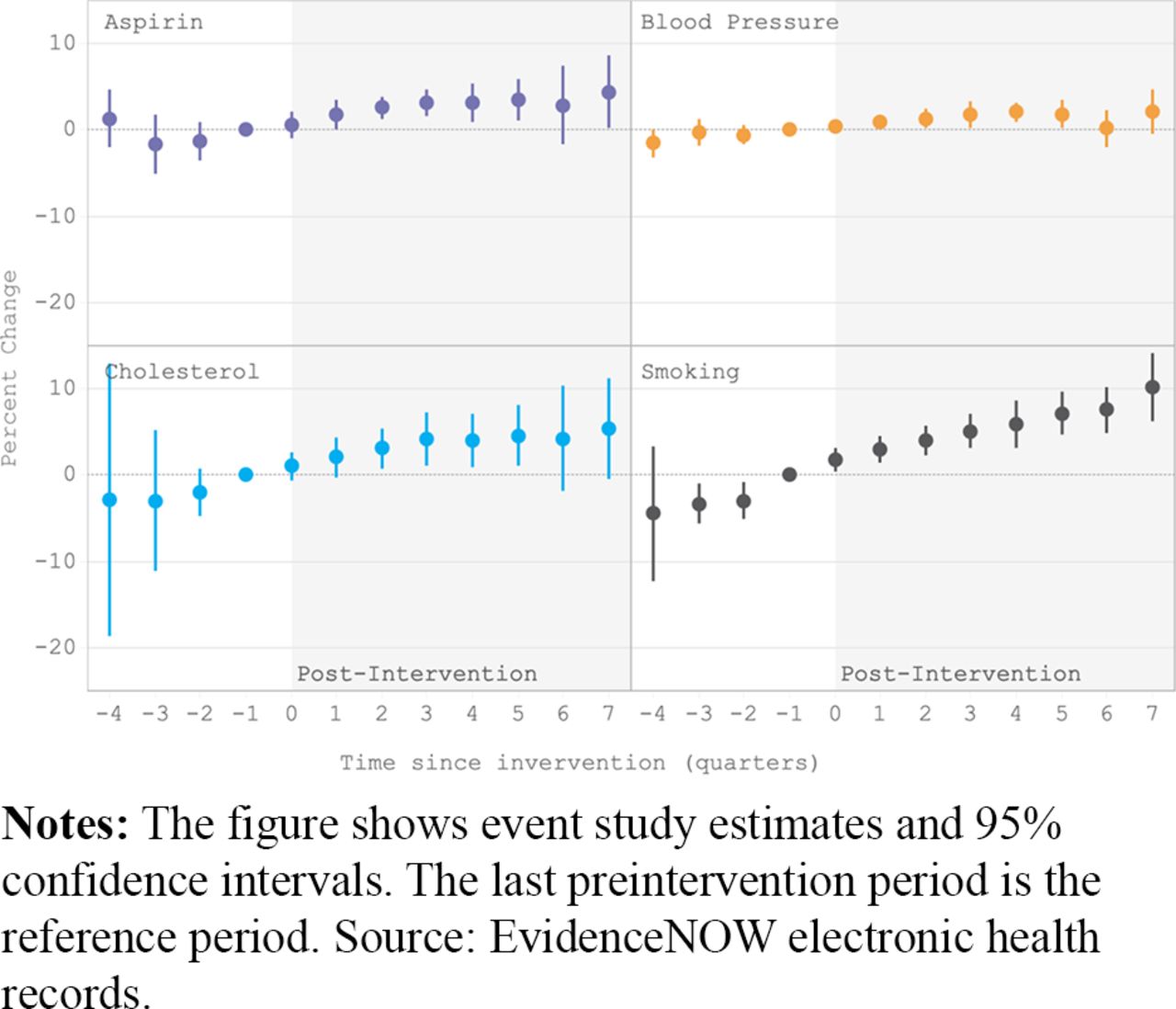
- Figure 2.
Event study estimates.

Tables
Aspirin Blood Pressure Cholesterol Smoking Denominator Patients 18 years and older with at least one face to face visit who (i) had an active diagnosis of ischemic vascular disease at any time during the current measurement period; (ii) were discharged alive for acute myocardial infarction, coronary artery bypass graft or percutaneous coronary interventions in the 12 months before the measurement period Patients 18 years and older and 85 years or younger with at least one face to face visit and active diagnosis of essential hypertension at any time before the first date of month 7 of the measurement period and who did not (i) have an active diagnosis of pregnancy at any time during the measurement period; or (ii) have evidence of end stage renal disease, dialysis, or renal transplant before or during the measurement period Patients 21 and older with at least one face to face visit who have (i) an active diagnosis of clinical atherosclerotic cardiovascular disease during the current measurement period or any time period; (ii) LDL-C result >= 190 mg/dL at any time during or before the measurement period; (iii) aged 40 to 75 years at the beginning of the measurement period with an active diagnosis of diabetes with the highest LDL-C result of 70 to 189 mg/dL during the current measurement period or two years before the beginning of the measurement period; and who (i) did not have adverse effect, allergy or intolerance to statin medication therapy; (ii) did not have an active diagnosis of pregnancy or breastfeeding; (iii) did not receive palliative care; (iv) did not have an active liver disease or hepatic disease of insufficiency; (v) did not have end stage renal disease; or (vi) did not have a most recent LDL-C results < 70 mg/dL for patients with a diabetes diagnosis who are not currently receiving statin medication therapy Patients 18 years and older as of the first day of the measurement period with at least two visits during the measurement period Numerator Number of patients who have documentation of use of aspirin or another antithrombotic during the measurement period Number of patients whose blood pressure at the most recent visit is adequately controlled (systolic blood pressure < 140 mmgHg and diastolic blood pressure < 90 mm Hg) during the measurement period Number of patients with a statin medication current on the medication list or prescribed a statin medication during the measurement period Number of patients who were screened for tobacco use at least once within 24 months and who received tobacco cessation intervention if identified as a tobacco user. Measurement period (EvidenceNOW practices) Data quarter and preceding three quarters Data quarter and preceding three quarters Data quarter and preceding three quarters Data quarter and preceding three quarters Notes: Measure specifications are based on CMS164v4 (aspirin prescription when appropriate), CMS165v4 (blood pressure control), CMS347v1 (cholesterol management) and CMS138v4 (smoking cessation support counseling).
Practice and patient characteristic EvidenceNOW Practices DARTNet Practices Practice size Solo 22.7 2 to 5 clinicians 46.7 6 to 10 clinicians 14.0 11 to 15 clinicians 10.6 Missing 5.9 Practice ownership Clinician 42.1 46.0 Hospital/health system/HMO 22.7 46.0 FQHCs 19.6 3.0 Other 11.4 4.9 Missing 4.2 0.0 Practice location Rural area 12.8 Large town 10.8 Suburban 6.3 Core urban 59.5 Missing 10.6 Insurance status: Fraction of patients Uninsured 9.9 Medicaid 23.0 Medicare 22.9 Dually eligible 7.1 Commercially insured 34.5 Other insurance 2.7 Race/ethnicity: Fraction of patients classified as White 59.8 49.1 Black 15.6 6.0 Unknown race 7.8 0.0 Hispanic 19.1 6.7 Unknown ethnicity 9.3 0.0 Practice participated in demonstration program No 53.7 Yes 19.7 Missing 26.6 Practice has MUA HER No 44.5 Yes 18.4 Missing 37.1 Notes: Numbers in the table are percentage values for practice characteristics and mean percentage values for patient characteristics. The sample includes all practices with at least one valid ABCS outcome measure during the study period (n = 1278 for EvidenceNOW practices; n = 613 for DARTNet practices). Practice location is based on the rural-urban commuting areas using 2010 Census data. Numbers for insurance status and race/ethnicity are average percentage values. They do not sum to 100 percent because practices were not required to report estimates that did so. Dual eligible insurance status includes patients receiving both Medicaid and Medicare. Demonstration programs include State Innovation Models Initiative, Comprehensive Primary Care Initiative, Transforming Clinical Practice Initiative–Support and Alignment Network, Community Health Worker training program, Blue Cross/Blue Shield patient-centered medical home program, Association of State and Territorial Health Officials’ Million Hearts State Learning Collaborative, Million Hearts: Cardiovascular Disease Risk Reduction Model, and any other program identified by the practice. HMO: Health Management Organization; FQHC: Federally Qualified Health Center; EHR: electronic health records; MUA: Meaningful Use. Sources: EvidenceNOW practice survey; DARTNet practice data.
Approach Aspirin Blood Pressure Cholesterol Smoking Event study Baseline level, % (SD) 64.9 (23.5) 63.6 (15.0) 61.5 (19.4) 62.0 (30.7) Change estimate 3.39 1.59 4.43 7.33 95% CI 0.61, 6.17 0.12, 3.06 0.33, 8.53 4.70, 9.96 P value 0.0167 0.0337 0.0342 0.0000 Pre-intervention trend test estimate (P value) 0.58 (0.37) 0.41 (0.19) 1.46 (0.27) 2.03 (0.002) Difference-in-differences, DARTNet comparison (all states) Baseline level, % (SD) (EvidenceNOW) 65.1 (23.2) 63.1 (15.2) 62.5 (19.2) 64.9 (30.2) Baseline level, % (SD) (DARTNet) 29.6 (20.3) 64.7 (20.4) 39.4 (19.2) 12.6 (9.1) Change estimate 3.75 2.76 3.87 8.32 95% CI −0.56, 8.06 −0.06, 5.58 −3.44, 11.18 2.89, 13.75 P value 0.0875 0.0556 0.2990 0.0027 Parallel trend test estimate (P value) 0.65 (0.50) 0.49 (0.46) 1.49 (0.26) 1.49 (0.35) Difference-in-differences, DARTNet comparison (EvidenceNOW states) Baseline level, % (SD) (EvidenceNOW) 64.9 (23.6) 62.9 (15.3) 62.0 (19.0) 61.4 (30.5) Baseline level, % (SD) (DARTNet) 31.0 (19.6) 63.6 (16.9) 40.9 (21.4) 15.9 (10.7) Change estimate 4.88 2.87 3.81 11.54 95% CI −3.33, 13.09 0.07, 5.67 −6.46, 14.08 3.56, 19.52 P value 0.2444 0.0447 0.4680 0.0046 Parallel-trends test estimate (P value) −0.54 (0.46) −0.55 (0.74) 0.53 (0.72) 2.67 (0.28) Abbreviations: SD, standard deviation; CI, confidence interval.
Notes: For the event study, baseline levels correspond to the last quarter before intervention begin (fourth quarter of 2015 for the first cohort to fourth quarter of 2016 for the fifth cohort). Estimates of the effect of interventions correspond to average estimates of the fifth to eighth post-intervention quarters. Pre-intervention trend estimates are based on the fourth to second pre-intervention period. For the difference-in-difference analysis, baseline levels correspond to the fourth quarter of 2015. Estimates of the effect of the intervention correspond to average estimates of the interaction term between an indicator for EvidenceNOW practices and 2017 quarters. Parallel-trends tests are based on the first and second quarter of 2016.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.