
Abstract
Context: Coordination between oncology and primary care practices in cancer survivorship is lacking.
Objective: To identify cancer care coordination perceptions, knowledge, and practices in a sample of Oklahoma oncology care providers (ONCs) and primary care providers (PCPs) regarding post-treatment care of adult cancer survivors.
Design: Cross-sectional, statewide survey by mail/web link in 2014/5.
Setting: PCPs identified through a primary care research network, primary care organization membership lists; ONCs identified through www.Healthgrades.com.
Participants: Contacts who were clinically active and seeing cancer patients were eligible. The final sample size included 101 ONCs and 58 PCPs who reported actively seeing cancer patients.
Measures: Responses to predominately Likert scale or ranked-order questions derived from the Survey of Physician Attitudes Regarding the Care of Cancer Survivors.
Analyses: Chi square and t tests were performed to test bivariate associations between provider type and survey measures.
Results: Statistically significant differences (P < .05) between ONC and PCP perceptions were observed for several questions on communication between the 2 provider types, ONC perceptions of PCP ability to address survivorship care, and responsibilities for post-treatment care.
Conclusions: Highly discrepant perspectives between ONCs and PCPs regarding communications and responsibilities for survivorship care may lead to adverse health outcomes. Interventions aimed at improving care coordination for cancer survivors should define each provider group's responsibilities in survivorship care, and create structures and processes that foster clear channels of communication between ONC and PCP practices.
- Cancer
- Cancer Survivors
- Cross-Sectional Studies
- Delivery of Health Care
- Oklahoma
- Primary Health Care
- Quality Improvement
- Survivorship
Introduction
The need to improve health care delivery for those who have completed cancer treatment is accelerating. Roughly 17 million individuals in the United Sates (US) have been diagnosed with cancer, but this figure will rise to over more than 22 million individuals by 2030.1 Cancer survivorship care, which typically focuses on the period of time after the completion of active cancer treatment, encompasses a range of complex health challenges. These include managing other chronic conditions (eg, heart disease, diabetes), monitoring for recurrent or new cancers, and addressing late effects of cancer treatment (eg, neuropathy, cardiomyopathy).2,3 High-quality survivorship care also helps patients address challenging psychosocial issues caused by cancer and its treatment. Changes in relationships, employment status, and health insurance coverage can lead to increases in financial distress, anxiety and depression.4⇓–6 Despite the growing need for high-quality cancer survivorship care, many patients who have had cancer do not receive recommended follow-up services.2,7,8
The frequency of visits to oncology providers (ONCs) is associated positively with receipt of recommended follow-up testing for cancer survivors.7 However, the majority of cancer survivors do not see ONCs regularly.8 One study showed that by 5 years after the completion of treatment, visits to ONCs declined substantially, with only one third of cancer survivors continuing to seek care from their ONCs.9 In contrast, nearly three quarters of these individuals continued to seek care from their primary care providers (PCPs). For a variety of chronic conditions including cancer, suboptimal care coordination and poor communication between specialists and PCPs results in fragmented care, increased costs and potentially avoidable morbidity and mortality.10⇓–12 The quality of cancer survivorship care depends on how well ONCs and PCPs are able to coordinate clinical services and communicate with each other, and with their mutual patients.13,14
Carefully implemented care coordination interventions focusing on chronic conditions, such as diabetes, for which clinical management falls within the scope of primary care practice have been shown to improve health outcomes.15,16 Similarly, greater coordination of care between ONCs and PCPs improves the quality of and patient satisfaction with follow-up care.17⇓–19 Effective communication between specialists and PCPs is a fundamental aspect of these care coordination interventions. Yet, communication between ONCs and PCPs is poorly understood. Multiple models aiming to enhance ONC-PCP coordination and communication for survivorship care have been described, including primary care-based, shared-care and specialist-based models.20⇓–22 Despite this attention, evidence that systematic ONC-PCP care coordination and communication occurs regularly for cancer survivors is lacking.23,24 Even primary care practices that have achieved patient-centered medical home status lack processes for delivering and coordinating cancer survivorship care.23
Cancer survivorship programs that capitalize on the fact that most cancer survivors continue to be seen in primary care even as they gravitate away from oncology care need to be developed and evaluated. Research, however, remains limited on how ONCs and PCPs perceive their roles in delivering care to cancer survivors,25 how well they communicate with each other, and how the follow-up needs of cancer survivors should be integrated into primary care.26 As a first step in building and implementing an efficacious survivorship care program, our team sought to gain a better understanding of the perspectives of both ONCs and PCPs regarding survivorship care. We investigated these issues in Oklahoma, which among all the states has the fourth worst cancer mortality rate,27 and the third and fifth lowest supplies of specialist and primary care physicians, respectively.28 A statewide survey was conducted to gather ONC and PCP perspectives on their communications regarding survivorship care, and to explore ONC and PCP views on their roles in the management of survivorship care for patients.
Methods
Sample and Participants
We conducted a cross-sectional, statewide survey by mail/web link in 2014/5 of oncology care providers (ONCs) and primary care providers (PCPs) to examine the perspectives of these 2 groups on treating patients who have completed the active phase of cancer treatment (ie, cancer survivors). We sought to draw, insofar as possible, a representative sample of ONCs and PCPs in Oklahoma who treat cancer survivors. However, no definitive membership lists of ONCs or PCPs were available, so the sampling frame included identification of ONCs through www.Healthgrades.com, mailing lists from state oncology organizations, and mailing lists of other, predominately surgical, specialist organizations whose members often treat cancer patients (eg, urologists). For PCPs, the sample was drawn by sending initial surveys by mail to addresses documented on professional membership lists of state primary care organizations (eg, Oklahoma Academy of Family Physicians) and via the listserv of a statewide practice based research network. All contacts were invited to participate if they were ONCs or PCPS and clinically active in seeing patients who had cancer or had been treated for it. Because nurse practitioners, physician assistants and registered nurses ae often involved in cancer survivorship care, these individuals as well as physicians were allowed to respond. The sample of ONCs included medical oncologists, gynecological oncologists, surgical oncologists (including the disciplines of otolaryngology, thoracic surgery, gastrointestinal surgery, and urology), and radiation oncologists. Respondents had the option of returning surveys by postage prepaid mailing envelopes or by completing an online version of the instrument. The final sample included 58 PCPs and 101 ONCs who met these criteria. The study was approved by the University of Oklahoma Health Sciences Center Institutional Review Board.
Measures
Survey
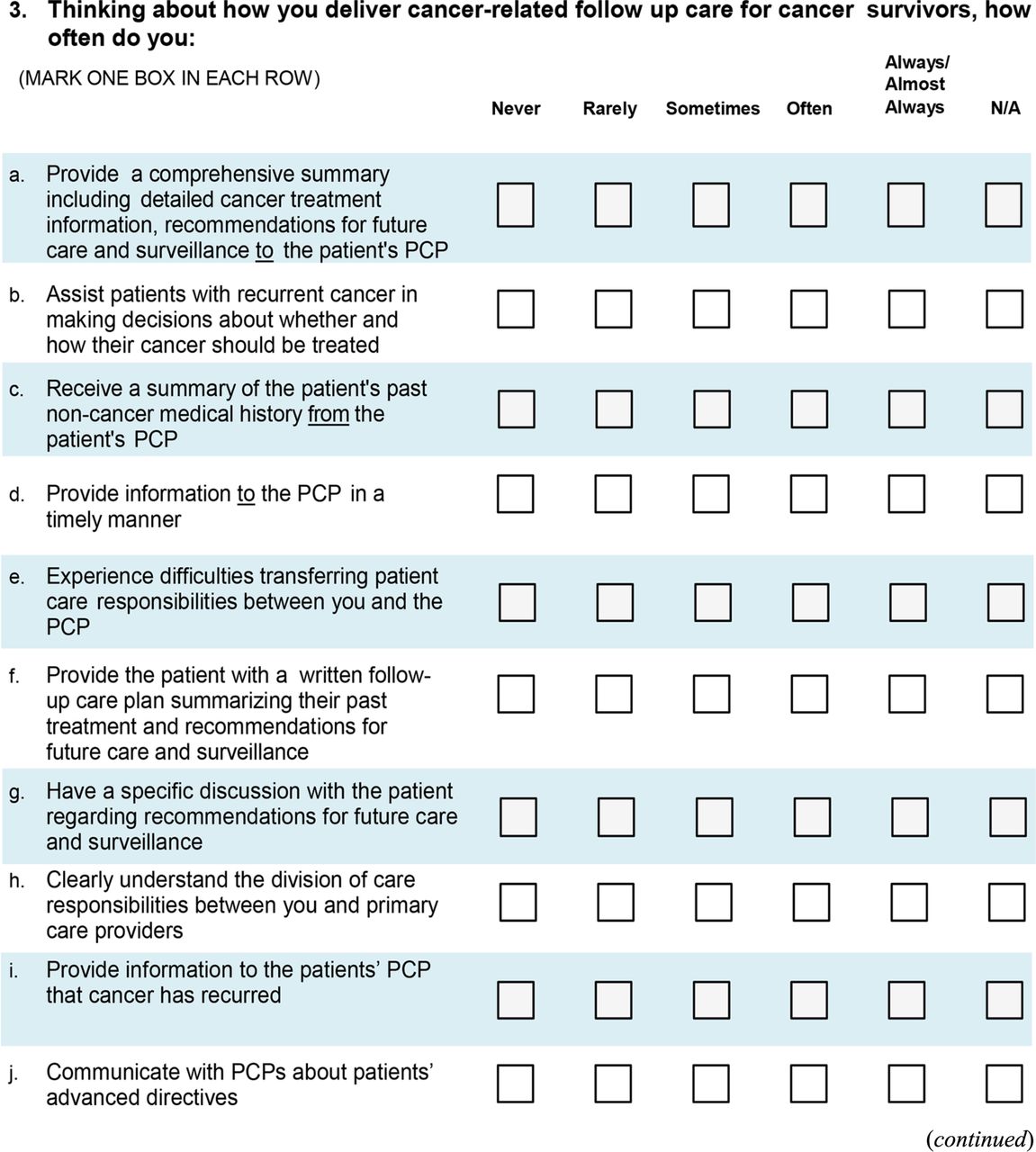
Participants were asked to respond to predominately Likert scale or ranked order questions derived from the National Cancer Institute/American Cancer Society Survey of Physician Attitudes Regarding the Care of Cancer Survivors (SPARCCS). The SPARCCS survey can be downloaded at http://healthservices.cancer.gov; detailed methods have been published elsewhere.29
SPARCCS was selected as the basis for the present PCP and ONC surveys because its questions permit comparisons by provider type of the perceived roles, knowledge, and practices of these 2 key provider groups with regard to follow-up cancer survivorship care, which involves surveillance for cancer progression or recurrence, identification of second cancers, and managing the medical and psychosocial late effects of cancer or its treatment. Online Appendices 1 (ONC) and 2 (PCP) present full surveys used in the current study.
Comparisons between ONCs and PCPs were made in the following thematic areas: 1) provider and practice characteristics (eg, years in practice, use of electronic data systems, practice-level capacity for change); 2) provision of cancer care coordination services (eg, communication between ONCs and PCPs regarding various aspects of patient care); 3) perceived confidence and skill of PCPs in providing cancer survivorship care (eg, skill in ordering appropriate cancer follow-up tests and detecting recurrences or late effects of cancer treatment); 4) preferred role in cancer survivorship care (frequency take responsibility for screening for other new cancer, detecting recurrences, etc.) and 5) preferred practice model for cancer survivor ship care (eg, care led by ONCs, PCPs, specialized survivorship clinics, or shared care).
Analyses
Frequency distributions were calculated for ONCs versus PCPs using the SAS software suite (v9.4; Cary, NC). Chi square testing with a 2-tailed P < .05 was performed to assess associations between provider type and survey measures. The small sample size limited the ability to adjust for potentially meaningful provider- or practice-level factors.
Results
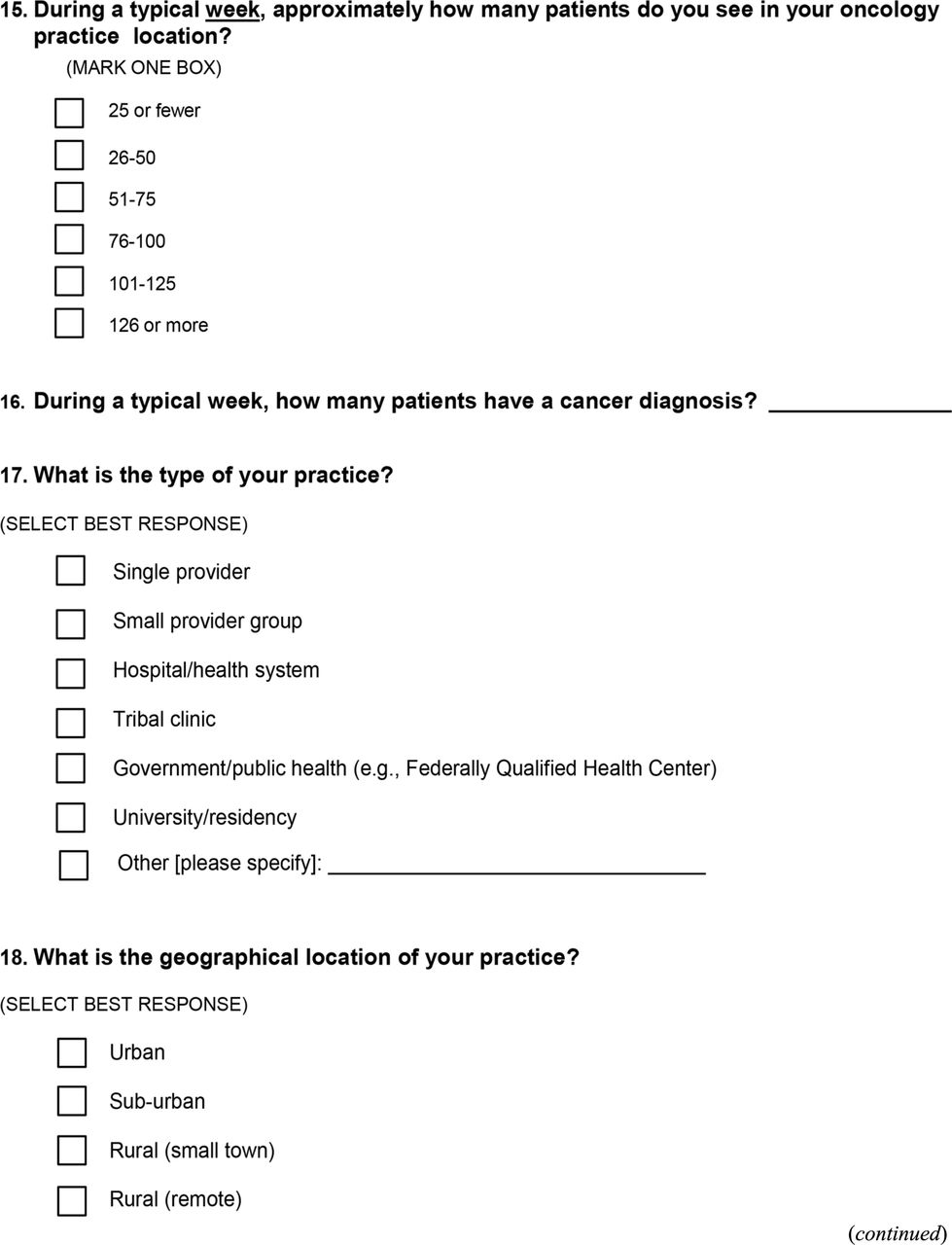
Regarding provider characteristics, PCPs were significantly more likely than ONCs to have spent more years in practice (P = .03) and worked in a rural location (P = .05) (Table 1). In addition, PCPs reported higher weekly patient volume (P = .03) than ONCs. Regarding practice characteristics, no statistically significant differences between ONCs and PCPs were observed for most measures, such as use of electronic billing systems or electronic health records. However, the difference between ONCs and PCPs in referral processes approached statistical significance, indicating that ONCs may be less likely than PCPs to have defined referral processes or dedicated personnel responsible for referrals (P = .06). In contrast, PCPs were significantly less likely than ONCs to report having defined care coordination processes or dedicated personnel responsible for care coordination (P = .04). The ONC-PCP difference in perceived practice change capacity was not statistically significant, with only about approximately 1 quarter of both ONCs and PCPs working in practices characterized as welcoming change.
Oncology Provider (ONC) and Primary Care Provider (PCP) Characteristics
Table 2 shows statistically significant ONC-PCP differences for several aspects of cancer care coordination. ONCs were more likely than PCPS to report they communicate routinely with other providers about who will follow the patient for cancer (P < .001) and who will handle cancer patients' other medical issues (P = .03). The proportion of ONCs who reported sending comprehensive cancer treatment summaries to PCPs was much higher than the proportion of PCPs reporting having received such summaries from ONCs (P < .001). In addition, a higher proportion of ONCs reported providing information to PCPs in a timely manner than PCPs reported receiving timely information from ONCs (P < .001). ONCs were more likely than PCPs to report they help patients with recurrent cancer make treatment decisions (P < .001) and have discussions with patients about future care and surveillance (P < .001). In addition, ONCs were much more likely than PCPs to report that they understand the division of care responsibilities between ONCs and PCPs (P < .001). The proportion of ONCs who reported sending information to PCPs that cancer had recurred was much higher than the proportion of PCPs who reported receiving information regarding recurrence (P < .001). Among ONCs, 27.1% indicated they “often, almost always, or always” provided patients with written follow-up care plans summarizing past treatments and recommendations for future care and surveillance (data not shown). Among PCPs, only 2.7% reported that they “often, almost always, or always” received an explicit follow-up care plan from the ONC with recommendations for future care and surveillance (data not shown).
Provision of Cancer Care Coordination Services by Oncology Providers (ONCs) and Primary Care Providers (PCPs)
Table 3 presents findings regarding confidence and perceived skill in the provision of cancer survivorship care among ONCs and PCPs. Compared with PCPs, ONCs reported higher confidence in ordering appropriate surveillance testing to detect recurrent cancer (P < .001) and detecting physical adverse effects of cancer or cancer treatment (P < .001). The ONC-PCP difference for confidence in addressing psychosocial outcomes of cancer or its treatment was nearly significant (P = .052), with ONCs reporting greater confidence in this realm. Table 2 also presents findings from the 3 survey questions on the perceived role of PCPs in survivorship care. Compared with PCPs, ONCs were much more likely to disagree with these statements, which included: PCPs have the skills needed to initiate appropriate screening or diagnostic work‐up (P < .001), PCPs should have primary responsibility for cancer‐related follow‐up (P = .02), and PCPs are better able than ONCs to provide psychosocial support (P < .001).
Confidence and Perceived Skill in the Provision of Cancer Survivorship Care by Oncology Providers (ONCs) and Primary Care Providers (PCPs)
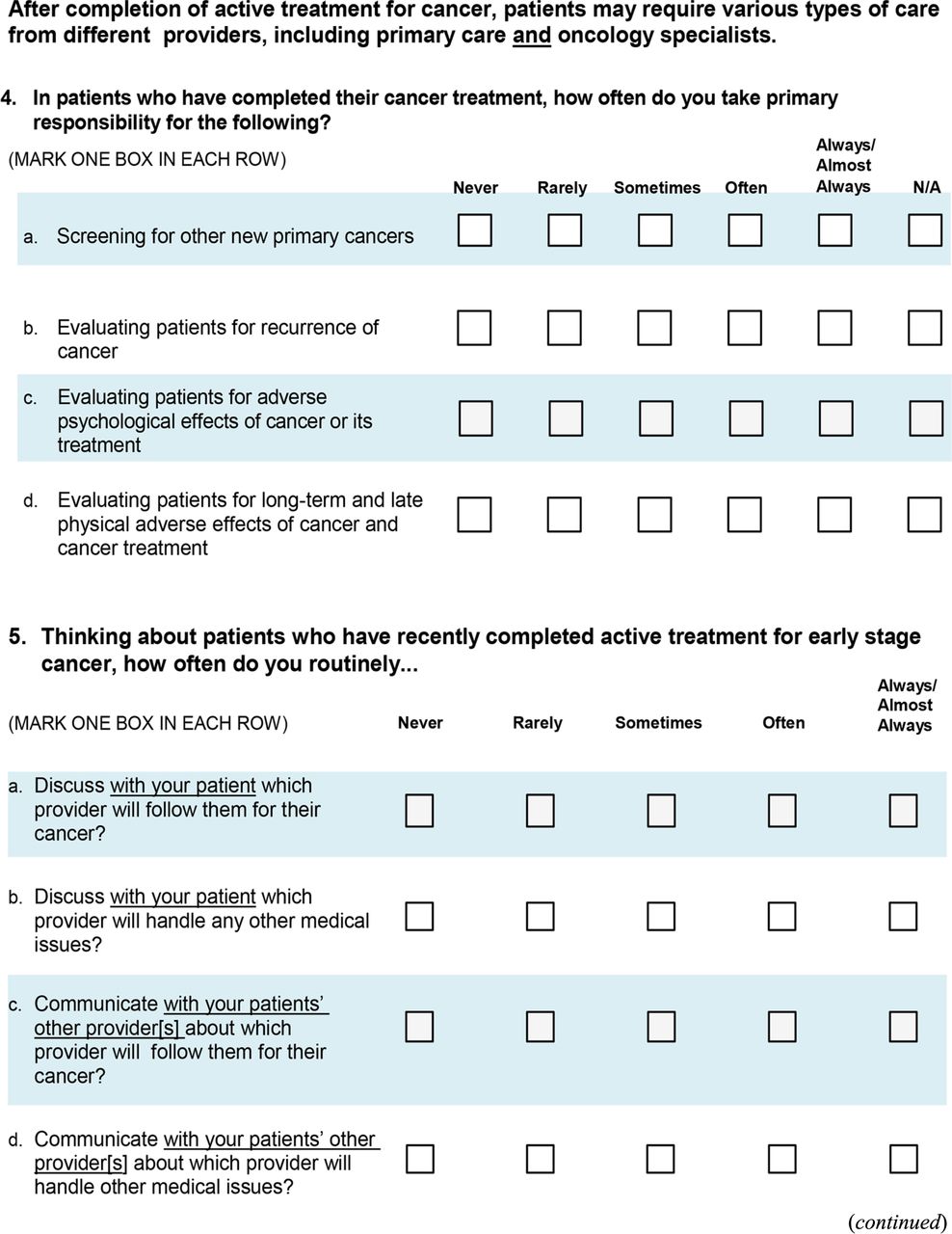
Table 4 shows that ONCs were less likely than PCPs to report that they screen patients for other new types of primary cancers (P < .001) and evaluate patients for adverse psychological effects of cancer or its treatment (P = .016). However, ONCs were more likely than PCPs to report that they evaluate patients for recurrence of cancer (P < .001) and for long-term and late physical adverse effects of cancer and cancer treatment (P < .001).
Oncology Provider (ONC) and Primary Care Provider (PCP) Perceived Role in Cancer Survivorship Care
Figure 1 shows the discrepancy between ONCs and PCPs on their ranking of 4 approaches to survivorship care for patients with early-stage cancer. The first choice among ONCs was an ONC-led survivorship care model, but this was the second choice among PCPs. In contrast the first choice among PCPs was an ONC-PCP shared care model, but this was the third choice of ONCs. The second choice of ONCs, specialized survivorship care clinics, was the fourth (last) choice among PCPs.

Preferred Approach to Survivorship Care for Patients with Early-Stage Cancer. Abbreviations: ONCs, oncology care providers; PCPs, primary care providers.
Discussion
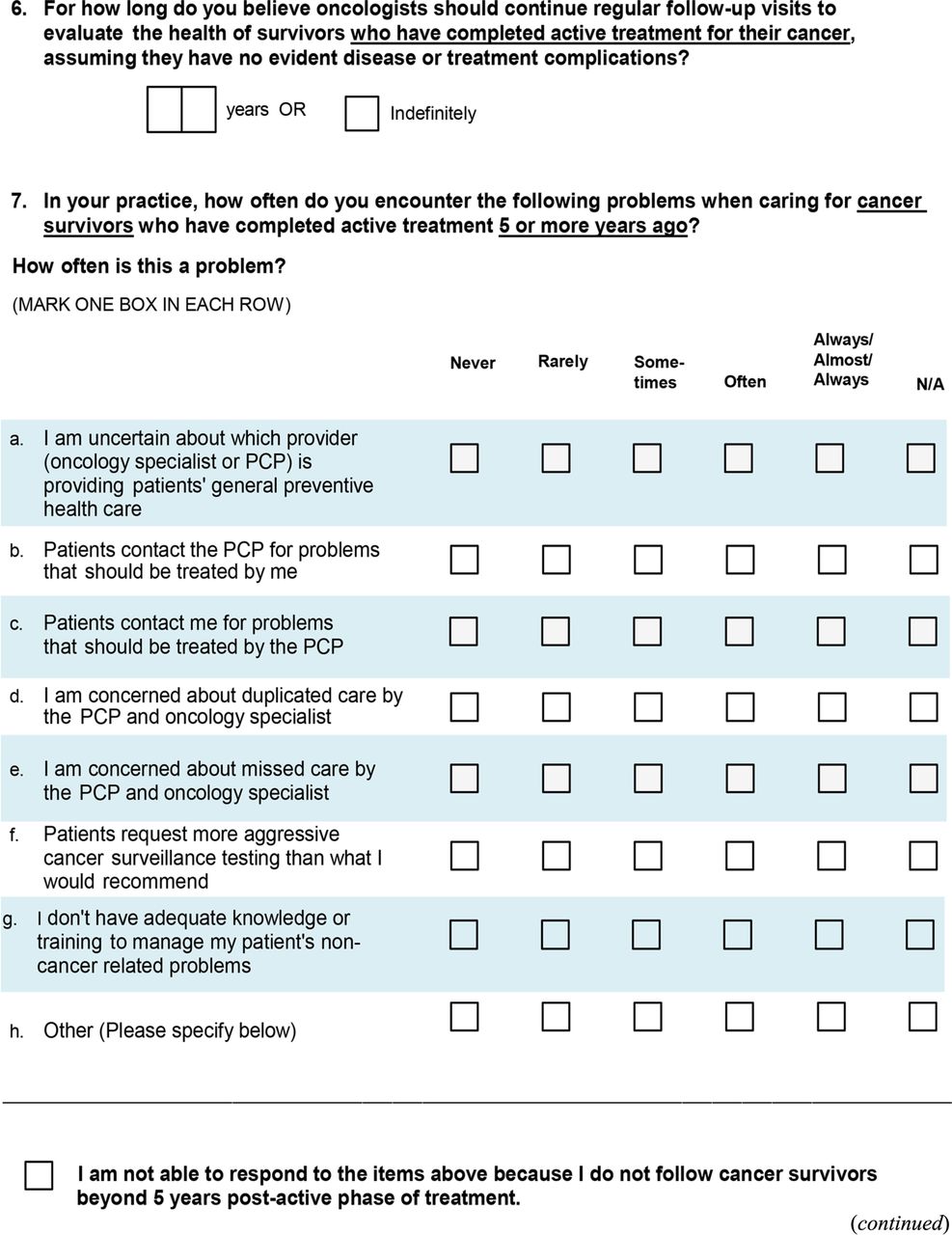
Our findings parallel other reports documenting poor communication and lack of care coordination between specialist physicians and PCPs.10,11,30⇓–32 We observed a discrepancy in which most ONCs reported that they provided information on survivorship care to PCPs, yet few PCPs reported receipt of this information. Furthermore, most ONCs felt that PCPs do not possess the skills to conduct follow-up cancer surveillance or provide psychosocial support for patients who have had cancer. In addition, most ONCs preferred that survivorship care be conducted by ONCs or by specialized survivorship care clinics, whereas PCPs tended to prefer a shared-care approach to survivorship care.
This lack of engagement between ONCs and PCPs is concerning given that the majority of cancer survivors do not see ONCs regularly,8,33 and visits to ONCs decline substantially by 5 years after the completion of cancer treatment.9 In contrast, most cancer survivors continue to visit their PCPs, and PCPs frequently address patient survivorship care needs.9,34 The deficits in ONC-PCP coordination observed by us and others29,35 can impede desirable outcomes by delaying follow-up testing and by missing opportunities to identify late effects of treatments.36⇓–38
The quality of cancer survivorship care hinges on how well ONCs and PCPs can bridge these differences. In recognition of the need to improve ONC-PCP coordination, the Institute of Medicine report, From Cancer Patient to Cancer Survivor: Lost in Transition highlighted coordination between ONCs and PCPs as 1 of 4 key components of survivorship care.2 Although this seminal report illuminated the issue of poor ONC-PCP care coordination, it provided little evidence-based guidance on how ONCs and PCPS could improve their interactions to optimize survivorship care delivery. One major barrier to achieving effective ONC-PCP care coordination is that ONCs and PCPs in the United States typically work within separate health care systems.39 Moreover, our findings reveal that only about approximately one quarter of ONCs and PCPs reported working in practices welcoming change. Given these organizational barriers, it is unsurprising that relatively little attention has been paid to developing and testing interventions to improve survivorship care, and that many of these attempts have faltered.
For example, standalone survivorship care plans (SCPs) have been developed to improve communication from ONCs,40,41 so have become a standard of care.42,43 Yet, SCPs alone have not been shown unequivocally to improve outcomes,44⇓–46 and many oncology practices nay not have the time or resources that are required to complete these forms. Modifying electronic health record (EHR) systems to improve ONC-PCP communication could also help, but can be difficult given the incompatibilities of EHR software products and the inability of health information exchanges that link EHRs to provide granular data on cancer survivorship.
Another key barrier to improving survivorship care coordination is that ONCs and PCPs disagree fundamentally on how care for cancer survivors should be delivered. In our study, ONCs favored oncologist-led clinics followed by specialized survivorship care clinics. In contrast, nearly half of PCPs favored a shared-care model in which PCPs and ONCs jointly manage survivorship. Specialized clinics were PCPs least favored option. A similar discordance between ONCs and PCPs in preferred survivorship care delivery models has been observed by others.35 In addition, many ONCs in our and other studies express skepticism that PCPs have the skills needed to initiate appropriate screening or diagnostic work‐up for cancer survivors.35,47 Given these differences, it is unsurprising that the quality of follow-up survivorship care has been shown to be suboptimal,48 and that many survivorship outcomes are overlooked by the health care system.8,49
Because ONCs and PCPs largely operate in separate spheres both in terms of how their clinics are organized and how they think about their roles in cancer survivorship care, we believe research is needed to develop and test interventions that can bridge these differences. Given that the growing number of cancer survivors will further strain ONC workforce supply and given that most cancer survivors stop seeing ONCs by 5 years post-treatment, we feel interventions to improve survivorship care coordination should not create new “carve out” services that would further compartmentalize the delivery of survivorship care. Instead, a major goal would be to help PCPs to know what to watch for and when to refer back to the cancer specialists.
One straightforward intervention that seems feasible would be to ensure that direct, structured personal communication between ONC and PCP practices occurs regularly. Ideally, this communication would be led by individuals with clinical judgment, such as nurse care coordinators, as many PCP practices already have nurses on staff who could take on this role. Such a point person could reach out periodically to counterparts at ONC practices to gather, organize and transmit clinically actionable information on survivorship care to PCPs. The point person could also contact patients to screen for psychological and financial distress and other patient concerns. One advantage is that activities nested within in primary care could be accomplished whether or not the oncology site regularly completes SCPs or provides specialized survivorship care services. A similar approach has been implemented and evaluated for rural preventive services.50 This mode of communication was nearly unanimously viewed as helpful by PCPs, which provides justification for developing and testing a similar approach for cancer survivorship care.
Another potential solution that has gained attention is to risk-stratify patients into survivorship care pathways based on the complexity of their ongoing needs and the types of providers their personalized pathway requires.51 This approach has been implemented successfully in England and Northern Ireland,52,53 which have single-payer systems. Implementation and evaluation of personalized, risk-stratified survivorship care across a variety of US health care settings merits attention, especially as value-based care gains traction. In particular, its application might be most feasible for early-stage, relatively common cancers having a good prognosis, as recent research shows promise in delivering survivorship care within the primary care setting to women with early-stage breast cancer.54 In addition, implementation and evaluation of interprofessional training in the use of a risk-stratified approach to cancer survivorship care is warranted, given that many primary care providers express a need to gain skills in this area.29,55⇓57,55,56,57
Our findings are subject to limitations. The survey was conducted in Oklahoma, which is a highly rural state with a disproportionate cancer burden and a low supply of ONCs and PCPs. Finding cost-effective solutions to cancer care coordination that can work in Oklahoma may not generalize to all geographic locations but may have important implications for locations with similar profiles. Because the small sample size precluded comparison of rural-urban differences in provider views about survivorship care needs, additional research would be needed to examine this issue. In addition, we lacked a definitive sampling frame for identifying ONCs and PCPs, although used a variety of sampling strategies to try to contact as many of these providers statewide as possible.
The sample included physicians, advanced practice nurses, and physician assistants. Experiences, perceptions and beliefs about cancer survivorship care could vary among these provider groups, but the small sample size limited our ability to explore this issue. It is possible that providers who have recently treated patients with cancer may have greater recall of whether information was communicated between oncology and primary care than their counterparts who have not recently seen these patients. In addition, oncology-primary care communications for patients who are critically ill may be recalled more vividly than for those who have milder illness. Moreover, instances in which communication between oncology and primary care was suboptimal may have a greater impact on recall than instances in which this information was communicated smoothly. Prospective data collection could help confirm or refute whether recall bias affects findings, but a prospective design was outside the scope of this small pilot study.
Although our sample size was small, our findings were strikingly similar to those reported by others.29,35 Because our survey was anonymous, ONC and PCP responses could not be linked. The data are now several years old, but the issue of the lack of coordination between oncology and primary care remains relevant.51 Finally, this report does not summarize companion qualitative research we are conducting (manuscript under review) that provides a richer understanding from ONCs, PCPs and patients on how to configure interventions to improve survivorship care. Importantly, this qualitative study will add patient perspectives on how and where they want to receive survivorship care.
Conclusion
ONCs and PCPs have widely divergent perspectives on cancer survivorship care, but both groups have vital roles in providing health care for patients who have been treated for cancer. We found that many PCPs indicated an interest in a shared-care approach to survivorship care. This is important because many patients stop seeing ONCs regularly for survivorship care and these numbers are likely to increase as the number of cancer survivors in the US grows. Effective interventions to improve ONC-PCP communications are needed, as are interventions to clarify provider roles in survivorship care. Poor patient outcomes that could be reversed through improved survivorship care will persist unless improvements in PCP-ONC care coordination are made.
Acknowledgments
Preliminary data from this study were presented at the 2015 North American Primary Care Research Group (NAPCRG) Annual Meeting; October 26, 2015; Cancun, Mexico.
Appendix 1 - Oncology Survey









Appendix 2 - PCP Survey








Notes
This article was externally peer reviewed.
Funding: This project was partially supported by grants (P30CA225520 and U54GM104938) from the National Institutes of Health.
Conflict of interest: No potential conflicts of interest are reported by any of the authors.
To see this article online, please go to: http://jabfm.org/content/35/2/329.full.
- Received for publication July 12, 2021.
- Revision received October 30, 2021.
- Accepted for publication November 3, 2021.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}