
Abstract
Background: Social determinants of health (SDOH) influence health outcomes. Food insecurity (FI) is the most common need related to SDOH. Many primary care practices and health systems have begun to screen for FI and refer patients to resources. How this process is viewed by multiple stakeholders, including patients, health care workers, and staff at food assistance organizations (FAOs), will influence its impact.
Methods: In this mixed-methods study, we completed 42 interviews with individuals from the 3 stakeholder groups. We then conducted a survey with 126 respondents using questions developed from the qualitative results.
Results: All stakeholders recognized the impact FI has on health outcomes, but perspectives varied on the value of sharing information through referrals to FAOs and concerning receipt of services, including privacy concerns and that the process would require significant work and not necessarily improve FI.
Discussion: Stakeholders agree that FI impacts health but have differences in perceptions around screening and referral done in health care settings. Perspectives of multiple stakeholders need to be considered when designing these systems.
Conclusion: Successfully designing systems to address FI through referral to FAOs requires input of multiple stakeholders because perspectives on the value and work required for this process vary.
- Colorado
- Community Medicine
- Data Sharing
- Food Insecurity
- Primary Health Care
- Qualitative Research
- Referral
- Social Determinants of Health
- Surveys and Questionnaires
Background
In 2014, the Institute of Medicine recommended that health care settings begin to screen for and report on social determinants of health (SDOH)-related needs,1 leading to development of screening tools and increasing implementation of screening processes.2⇓⇓–5 However, even earlier, the American Academy of Pediatrics and others recommended screening for food insecurity (FI) in health care settings.6,7 FI is defined by the U.S. Department of Agriculture as “a household level economic and social condition of limited or uncertain access to adequate food.”8 FI is the most commonly identified need related to SDOH, affecting approximately 11% of the population in the United States in 2019 and up to 23% after the onset of the COVID-19 pandemic in March 2021.9,10
Patients identified as experiencing FI may benefit from being connected to resources, but several barriers exist, including time needed, lack of patient trust and comfort with the process, and the multiple points where referrals to food assistance organizations (FAOs) can fail (eg, lack of communication between the patient and FAO, ineligibility for services).11 In addition, closed-loop communication, where practices receive information about receipt of services, may help health care providers know that patient needs are being met. Effective systems for making referrals to FAOs allowing this kind of closed-loop communication with practices rarely exist or are in early stages of development.12⇓⇓–15
Each of these screening, referral, and closed-loop communication processes involve personal data sharing. In addition, attitudes toward data sharing and privacy differ across population groups.16⇓⇓–19 Although existing literature indicates high acceptability of data sharing among patients and caregivers for the purposes of addressing FI in urban and pediatric settings, less is known about perspectives in the context of adult primary care and in nonurban areas.20⇓–22 In addition, this type of data sharing depends on the comfort and participation of 3 primary stakeholder groups: patients, health care workers (HCWs), and FAO staff. Information on the perspectives of all 3 of these stakeholder groups is scarce, and yet the active involvement of each is essential for successful interventions to address FI in health care settings.23 In this article, we share findings regarding multistakeholder perspectives on data sharing for the purposes of FI screening and referral in primary care settings located in rural and smaller town locations.
Methods
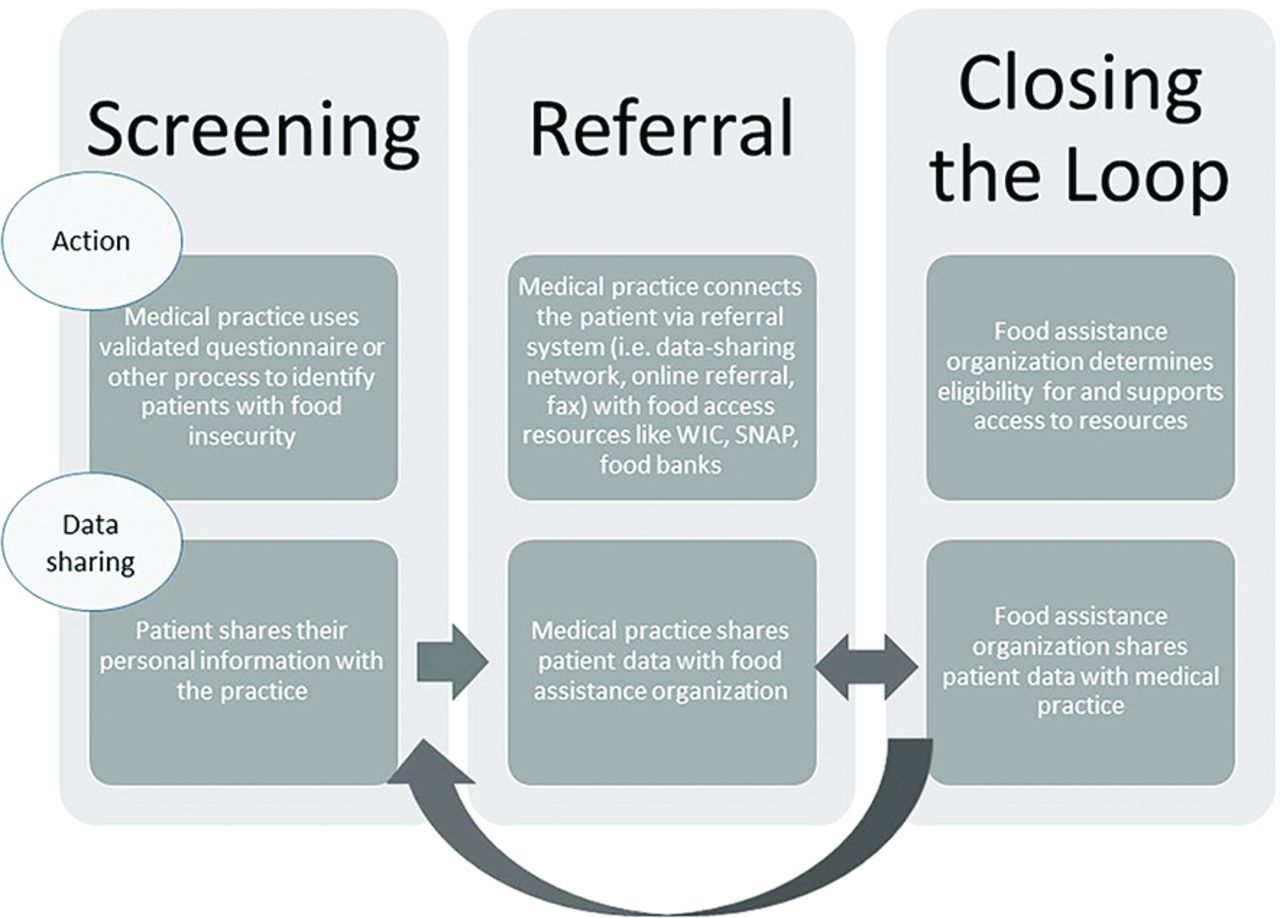
We used an exploratory sequential mixed-methods design, beginning with semistructured interviews, followed by a survey.24 Data collection took place between April 2019 and March 2020. The Colorado Multiple Institutional Review Board approved our protocol, and we used the Consolidated Criteria for Reporting Qualitative Research as a guide for reporting our results.25 We conceptualized the process of addressing FI in health care settings as having 3 distinct steps: screening to identify FI, referral to FAOs, and closing the loop. Figure 1 describes each step and the corresponding flow of data among the 3 key stakeholder groups: patients, HCWs and FAOs.

Steps and data flow for screening and referral. Abbreviations: WIC, Women, Infants, and Children; SNAP, Supplemental Nutrition Assistance Program.
This research took place in Mesa County, Colorado, which has 1 medium-sized city, Grand Junction, with a population of 63,500, and a total county population of 154,000,26 indicating that a majority of Mesa County residents live in small towns or rural areas. Eleven percent of Mesa County residents live in poverty, compared with 9.3% statewide,26 and 12.6% reported FI before the COVID-19 pandemic began.27 The Latinx community is the largest minority group, comprising 15% of the population.26
Qualitative Data Collection and Analysis
FI participants (ie, patients) were recruited by: (1) care managers (generally social workers or medical assistants with added experience and training) at 2 practices during scheduled visits or (2) the research team at community events. Prospective participants were asked screening questions to confirm lifetime experience of FI.6 We also recruited providers and care managers at 5 practices and staff at 12 FAOs.
Members of the research team (EB, AN, or MS, all non-Hispanic females with training in qualitative interviewing; MS with college-level training in Spanish) conducted interviews either in-person or by phone in English or Spanish, depending on the participant's preferred language. Research team members did not have existing relationships with any of the respondents. Informed consent was obtained before all interviews. We developed and used a separate semistructured interview guide for each stakeholder group. Questions were based on a list of constructs developed with the assistance of the project advisory group, a committee of individuals with professional or lived experience with FI. We pilot tested each guide with 2 people from the specific stakeholder group and revised it accordingly. Interviews lasted 30 minutes on average (range 15 to 65 minutes) and were audio recorded and professionally transcribed. Spanish-language interviews were transcribed in Spanish and then translated to English. Participants received a $25 gift card.
Rapid qualitative analysis techniques have been shown to result in similar theme development when compared with traditional qualitative thematic analysis, offer earlier return of findings, and are often combined with other analytic methods.28,29 These approaches work well for studies in which specific answers are sought for intervention development or refinement, such as with this study. We therefore analyzed interview data using a 2-step process consisting of a modified rapid analysis approach30,31 followed by coding to identify emergent themes. We first developed an interview summary template that captured respondents' comments regarding the 3 steps in screening and referral outlined previously. After each interview, the interviewer immediately completed the template. A second research team member then read each transcript and reviewed the summary to ensure accuracy. We then developed a matrix with columns depicting categories from the summary template and rows depicting individual respondents. The content from each individual summary was directly abstracted into this matrix, allowing the research team to review the summarized statements of all respondents for each category, and thereby to begin identifying themes and variation across respondents.
Following the rapid analysis, we developed a simple code list based on topics emerging as salient for further exploration. These included, eg, “experiences with screening and referral” and “perspectives on data-sharing.” Given that the coding was in larger conceptual chunks, coding across reviewers was highly consistent. As an additional measure, 2 researchers (AN and EB) coded independently and compared results for 2 transcripts and found high consistency of code use, thus not requiring further double-coding.32 AN and EB then coded all transcripts independently using ATLAS.ti software (version 8.0, Scientific Software Development GmbH, Berlin, Germany). Three study team members (AN, EB, and JH) then reviewed all coded segments and through an iterative process of group discussion identified key themes specific to each stakeholder type and each process step.
Quantitative Data Collection and Analysis
With input from our project advisory committee, we developed a survey examining emergent topics of interest following our qualitative analysis. Our purpose was to build from the interview data and gather confirming or disconfirming data from a larger sample of stakeholders. For example, our interview data suggested differences across stakeholder groups in perceptions of patient comfort with data sharing and helpfulness of data sharing. We therefore developed questions examining each of these domains (perceived patient comfort and perceived helpfulness) in relation to each of the 3 steps from our conceptual model (see Figure 1). After pilot testing, we administered the same survey to individuals from all 3 stakeholder groups, to allow for comparison of responses across groups.
Researchers (MS or EB) recruited patients to participate in the survey in the waiting rooms of 3 clinics, displaying recruitment signs and waiting for patients to approach. Prospective participants were screened to confirm lifetime experience of FI.6 After obtaining informed consent, surveys were completed in person in a private space. HCWs and FAO staff received e-mails requesting participation and completed surveys using the online survey platform REDcap. Participants received a $10 gift card. Survey data were descriptively analyzed by calculating response frequencies, disaggregated by stakeholder type.
Following data collection and analysis, member checking was done through 6 presentations of results and discussions with HCWs, FAO staff, academic experts on FI, and patients.
Results
We interviewed 42 individuals: 20 patients, 12 FAO staff members, and 10 HCWs (5 physicians, 5 care managers/staff who complete screenings for SDOH). We surveyed a total of 126 individuals: 50 patients (representing an 83% response rate), 37 FAO staff (representing a 63% response rate), and 39 HCWs (for the survey, only physicians and advanced practice providers were asked to respond, a 76% response rate). Providers represented 5 primary care practices (1 federally qualified health center, 1 residency program serving a low-income population, 1 large multisite private practice, and 2 small private practices). The 49 FAO staff represented 16 organizations (5 governmental, 11 community-based organizations). As providers and FAO staff who had participated in interviews also received an invitation to participate in the survey, there was some overlap in those groups but no overlap in the patient participants. Respondent demographic characteristics and responses to FI questions are shown in Table 1. Of note, patients had the most lifetime personal experience with FI, although a significant number of FAO staff had also personally experienced FI. HCWs were the least likely to have personal experience of FI.
Interview and Survey Participant Demographics
Qualitative themes and survey results: Table 2 presents our interview findings and Figure 2 presents our survey findings.
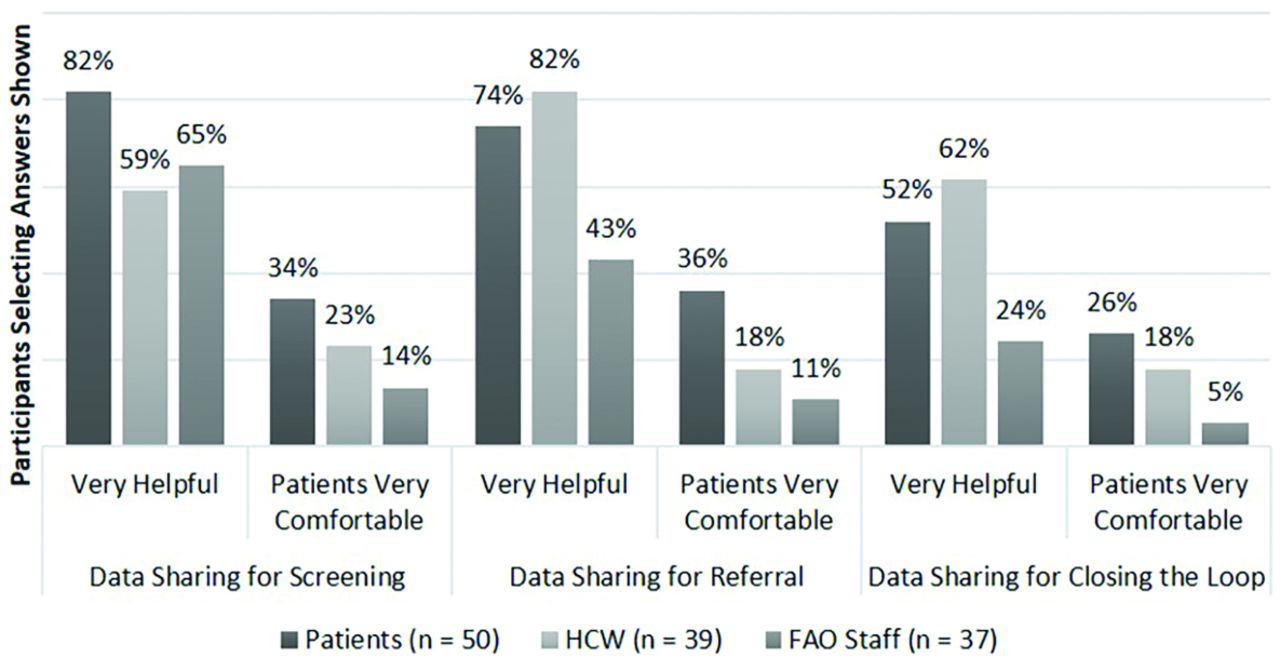
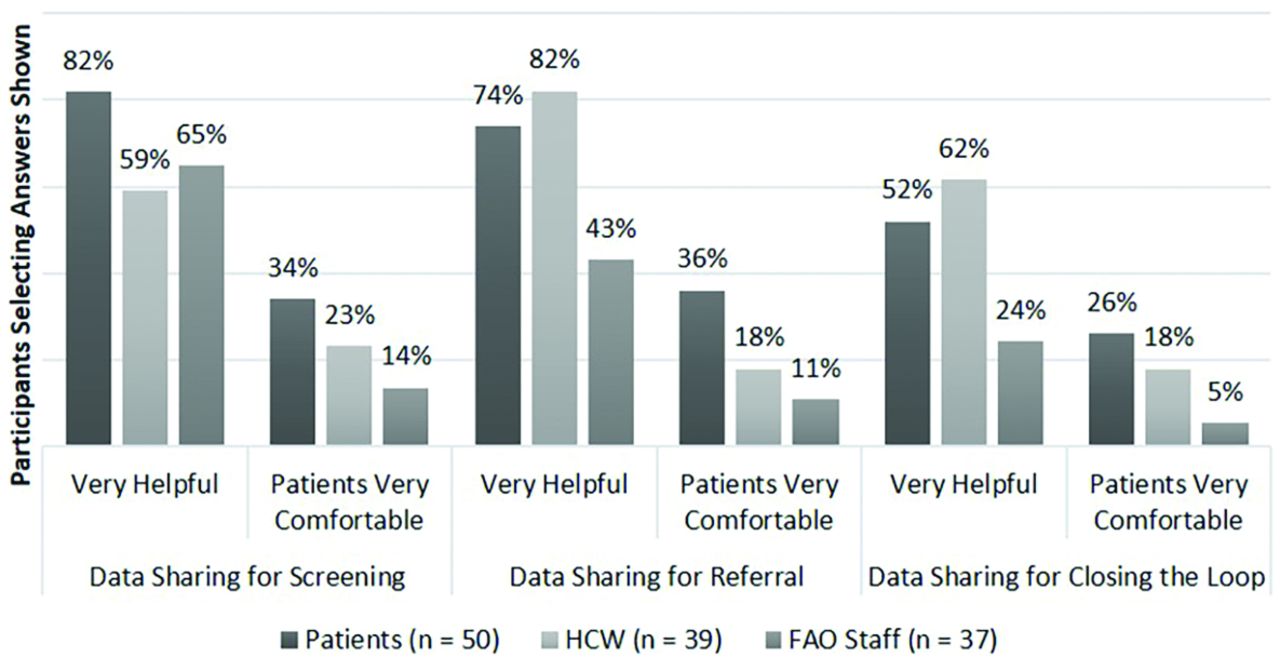
Survey responses across stakeholder groups. Abbreviations: HCWs, health care workers; FAO, food assistance organizations.
Themes, Perspectives across Stakeholder Groups, and Illustrative Quotations for Qualitative Findings on Screening, Referral, and Closing the Loop to Address Food Insecurity (FI) in Primary Care Practice
Screening
Qualitative Themes
Overall, respondents understood the connection between FI and health and believed that the data sharing involved in screening for FI was important and could give HCWs insight into patients' lives and health. Differences by stakeholder group are described below.
Patients
While respondents indicated surprise at the thought of being asked at an appointment whether they had enough food, they also indicated that they would be comfortable talking about FI. They thought knowing about FI would help their medical provider to better understand their health and ability to follow through on dietary recommendations. In contrast, a few indicated that they would not want to talk to their doctor about FI, due to wanting privacy or being concerned, eg, that Child Protective Services (CPS) would be notified if the family did not have enough food. Respondents generally felt that being asked about FI so clinic staff could suggest resources would be acceptable, but being asked for the sole purpose of data collection would not be.
HCWs
HCWs identified the value of screening for FI and indicated that screening all patients would generate helpful information but noted challenges related to staff time and logistics. Care managers in particular indicated that they thought screening questions were best asked in person and that results may not be reliable in the absence of a trusting relationship. Medical providers also expressed concern that the information gathered might not be used to actually assist patients experiencing FI.
FAO Staff
FAO staff also believed FI was related to health outcomes and that screening in health care settings could be valuable because providers could encourage people to pursue assistance. However, they were less convinced than the other 2 groups that patients would be comfortable sharing information about FI with their health care providers.
Survey Results
Eighty-two percent of patients answered that screening for FI in health care settings was “very helpful,” but only 34% thought people would be “very comfortable” discussing FI. Only 59% of HCWs answered that screening was very helpful, and 23% thought patients would be very comfortable. FAO staff seemed least favorable to this step, with 65% responding that this step would be very helpful but only 14% answering that patients would be very comfortable (see Figure 2).
Referring Patients to Resources
Qualitative Themes
Compared with screening, this step elicited more concerns from all groups, primarily around the work and logistics required to ensure effectiveness.
Patients
Patients were generally comfortable with information being shared with organizations, if the intent was connection with resources, but were emphatic that they would want to be asked permission before information was shared. Patients also reported that referral is only 1 step in accessing resources and that many other barriers exist, such as needs around transportation or inability to complete forms or take time off from work to access resources.
HCWs
Providers had privacy concerns related to the Health Insurance Portability and Accountability Act (HIPAA) about sharing patient information with FAOs. However, care managers generally said that they already shared patient contact information with programs like SNAP or WIC, indicating that some information sharing is already happening. Many reported that the work to refer is not compensated, and practices are already overwhelmed. Care managers mentioned that having improved mechanisms or formal systems for connecting patients with resources would help with logistics (eg, electronic referral systems).
FAO Staff
Collaboration with medical providers and strategies to help address FI were viewed as beneficial. However, FAO staff expressed concern that they would be unable to handle a large influx of referrals given grant funding, volunteer staffing, and space limitations. For programs like WIC and SNAP, the concern was the work required to process more applications, particularly if there were incomplete applications or people were not actually interested in or eligible for the services. Similar to patients, they identified other barriers that prohibit connecting people with food resources, including fear of consequences such as loss of potential citizenship due to the public charge ground of inadmissibility rule33 or CPS involvement.
Survey Results
In response to the question about helpfulness of data sharing for referrals, 72% of patients, 84% of HCWs, and only 43% of FAO staff thought this step was “very helpful”; 36% of patients thought people would be “very comfortable” (about the same as for comfort with screening), but only 11% of FAO staff and 18% of HCWs thought patients would be very comfortable with this step (see Figure 2).
Closing the Loop
Qualitative Themes
Perspectives differed more across groups for this step, with patients and FAO staff indicating greater privacy concerns and HCWs emphasizing its importance.
Patients
Most respondents said that they would be okay with this information sharing, but that they would want to be asked for permission. However, a few stated unequivocally that they would not want this information shared with their medical provider, as they felt receiving services was sensitive information. Respondents suggested that there could be shame around such information being shared due to the stigma around use of certain programs. Concerns about data security were also mentioned, specifically that data systems are vulnerable to hackers.
HCWs
This group was most adamant that this step is crucial for understanding patient circumstances. Care managers thought it would increase efficiency if they were able to easily receive information from FAOs regarding patients' receipt of services, noting that they often get no feedback after making a referral. They emphasized that the information would need to be easily obtainable, suggesting it automatically be put in patient charts through the electronic health record.
FAO Staff
Program staff were enthusiastic about greater collaboration with practices but emphasized that they were very protective of privacy. In general, they felt hesitant about data sharing, although some indicated that it would be acceptable if they had permission from the patient. Another concern was time required and cost to use a data-sharing system, especially for organizations that relied primarily on volunteers for staffing or limited budgets. Finally, several program staff indicated that data sharing was not something they could control and that any decisions about data sharing would happen at a higher leadership level.
Survey Results
Fifty-two percent of patients and 24% of FAO staff thought this final step in the process was “very helpful,” compared with 62% of HCWs. Regarding patient comfort, only 5% of FAO staff thought patients would be “very comfortable” with closing the loop, compared with 26% of patients and 18% of HCWs.
Discussion
Broadly, people from all stakeholder groups believed that FI was important to address in health care settings and that screening for FI and connecting patients with resources was valuable. However, there were differences in comfort with and perception of the importance of data sharing between medical practices and FAOs. FAO staff were the most concerned about client privacy related to information sharing. In addition, FAO staff are required to capture and report data for grants and federal or state programs using specific systems, which makes sharing additional data through different systems challenging. HCWs were unsure of how HIPAA regulations apply to sharing of SDOH-related information, an issue that is not entirely clear despite recent efforts to integrate screening and referral into practice.34,35 In addition, some patients had concerns with each step of the process, primarily related to privacy and the potential for shame or stigma around either experiencing FI or receiving services. These findings concur with and build on previous research documenting concerns among some patients related to privacy and stigma around FI and other SDOH needs.36⇓⇓–39 They add new insights from the perspective of FAO staff, whose views are often not considered when developing FI referral systems.40 They also provide insight into perspectives of people living in a rural and small-town setting.
These findings may have implications for the use of referral systems and how they are implemented. First, it was important to all stakeholders that the work required to screen, refer, and close the loop lead to reduction in FI. Burnout and information overload already exist in primary care such that some experts feel that adding another process like screening for SDOH needs is not feasible or worth the effort.41,42 Primary care providers and staff wanted to know they could do something with information on patients' FI, because screening itself is another task in an already taxed system. Similarly, FAO staff expressed concerns about their ability to participate in a referral system due to resource limitations and workload. For effective systems to be developed and adopted, this added workload should be addressed.43 In addition, as has been found elsewhere, patients reported that access to information or referral is not the only or primary barrier to accessing resources.44 This points to the need for multilevel structural and policy change, in addition to efforts to address FI within primary care settings.45
Second, we learned that personal relationships with clinic staff may make screening and referral more comfortable for patients, leading to more honest responses, but face-to-face screening is challenging for practices given time constraints. While the literature is mixed on whether people are more honest when responding to in-person questions compared with computer or article questionnaires,46⇓–48 there is strong evidence that patients are more comfortable discussing sensitive topics when there is a close relationship with staff.49,50 This has implications for workflow, as many practices currently use patient-completed article screening forms. Finally, this supports recommendations for approaching screening for SDOH from a team-based and patient centered approach.51
A limitation of this work is that these data represent conveniently sampled stakeholders in 1 area of western Colorado and may not represent the views of people in other geographic areas or contextual circumstances. In addition, the work was conducted both with patients who have experienced screening for FI and those who have not, so some of their responses may be more speculative than a description of their personal experience (ie, possible selection or recall bias).52
Conclusions
Our findings provide multiple stakeholder perspectives for health care settings that are currently implementing or seeking to implement screening and referral for needs related to SDOH. In particular, our findings provide new insights about sharing data about FI between primary care settings and FAOs. While all stakeholders see some benefit to these processes, concerns still exist and differ across stakeholder groups. FAO staff in particular have concerns about privacy, ability to share information, and whether people experiencing FI will truly benefit. Patients and FAO staff were generally more comfortable with screening and referral and less comfortable with closing the loop. In contrast, HCWs felt strongly that closing the loop is crucial, and if systems do not feed information back to practices, there is a potential that screening and referral could be jettisoned due to other pressing clinical tasks. Critical components of addressing FI in primary care settings include robust procedures for obtaining permission for data sharing at each step of the process, communicating with patients about reasons for data sharing, easing the administrative burden of data sharing for HCW and FAO staff, and reassuring FAO staff that data will be treated with confidentiality and respect.
Acknowledgments
We are grateful to all of our community partners in Mesa County, Colorado, who participated in this work, as well as to Elizabeth Staton for technical writing support.
Notes
This article was externally peer reviewed.
Funding: This research was supported by the Colorado Evaluation and Action Lab of the University of Denver. The opinions expressed are those of the authors and do not represent the views of the Colorado Lab or the University of Denver.
Conflict of interest: none.
To see this article online, please go to: http://jabfm.org/content/35/1/85.full.
- Received for publication March 2, 2021.
- Revision received August 24, 2021.
- Accepted for publication September 9, 2021.




{kind=link}
{kind=link}