
Article Figures & Data
Figures
- Figure 1.
Key Drivers of Implementation Domains and Supporting Activities for Plan, Do, Study, Act (PDSA) framework in Practice Facilitation. Abbreviations: BP, blood pressure; HTN, hypertension.
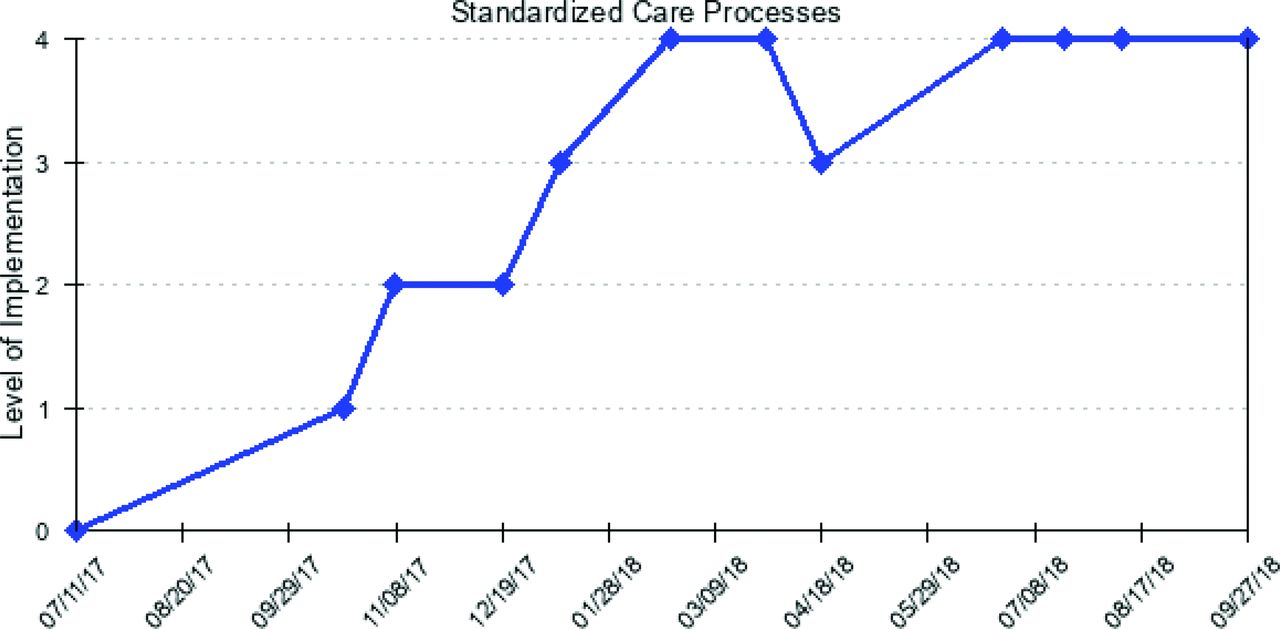
- Figure 2.
One Practice's Standardized Care Plan, Do, Study, Act Process using the Key Driver Implementation Scale.
- Figure 3.
Months of Active Practice Facilitation by Study Site, Facilitator, and Practice in the Southeastern Collaboration (SEC) to Improve Blood Pressure Control Trial. *PF 1a's practices were facilitated by PF 1b starting in study month 5; Pr = Practice; Site = University site in the SEC study. Abbreviation: PF, practice facilitation.
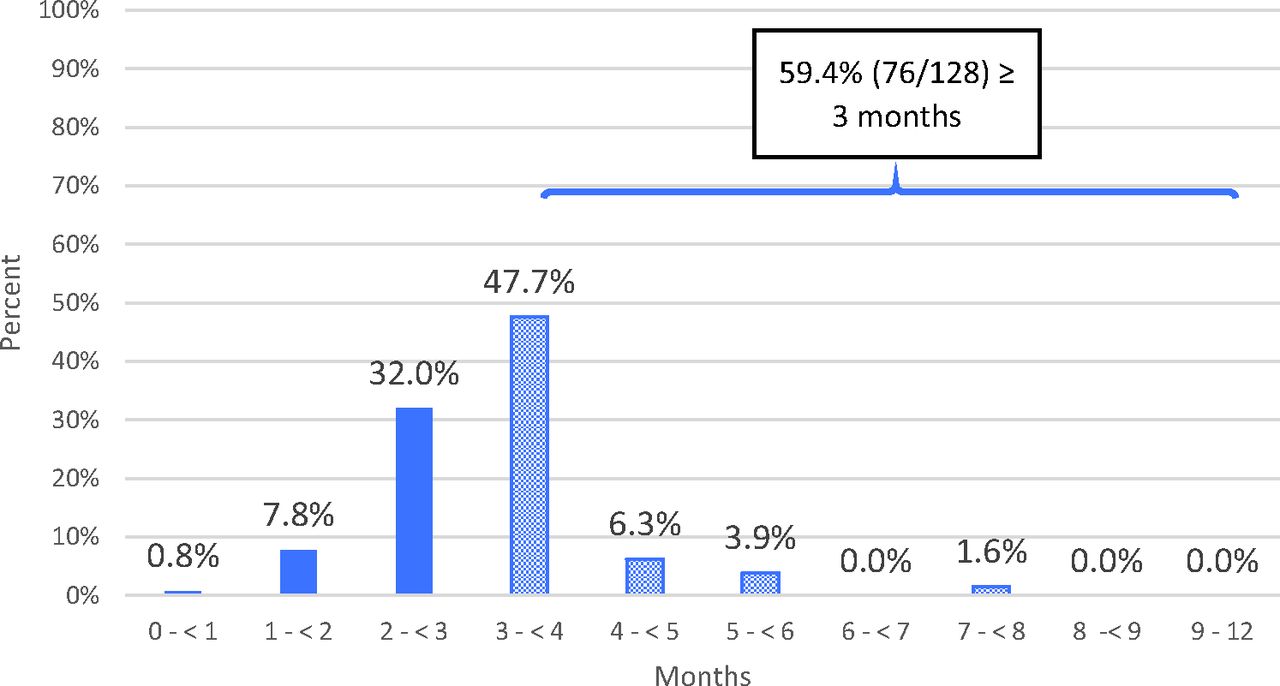
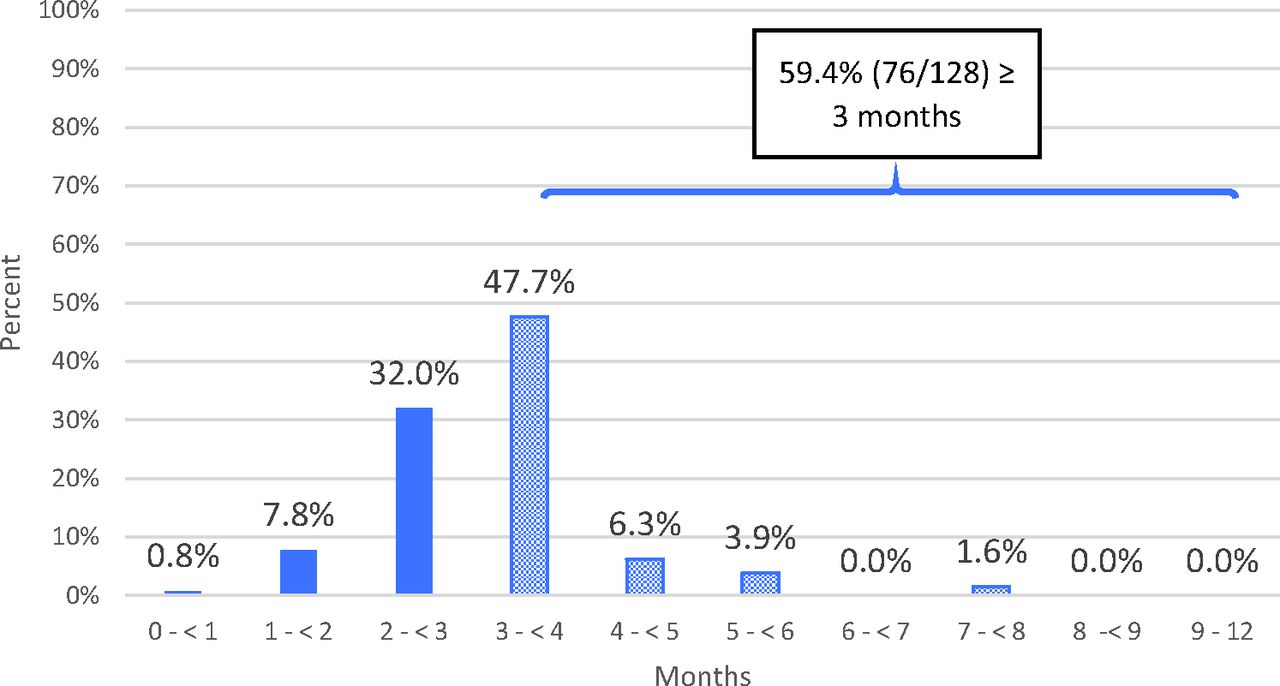
- Figure 4.
Percentage of Plan, Do, Study, Act (PDSA) cycles by months active in the overall sample (n = 128 PDSA cycles) in the Southeaster Collaboration to Improve Blood Pressure Control Trial.
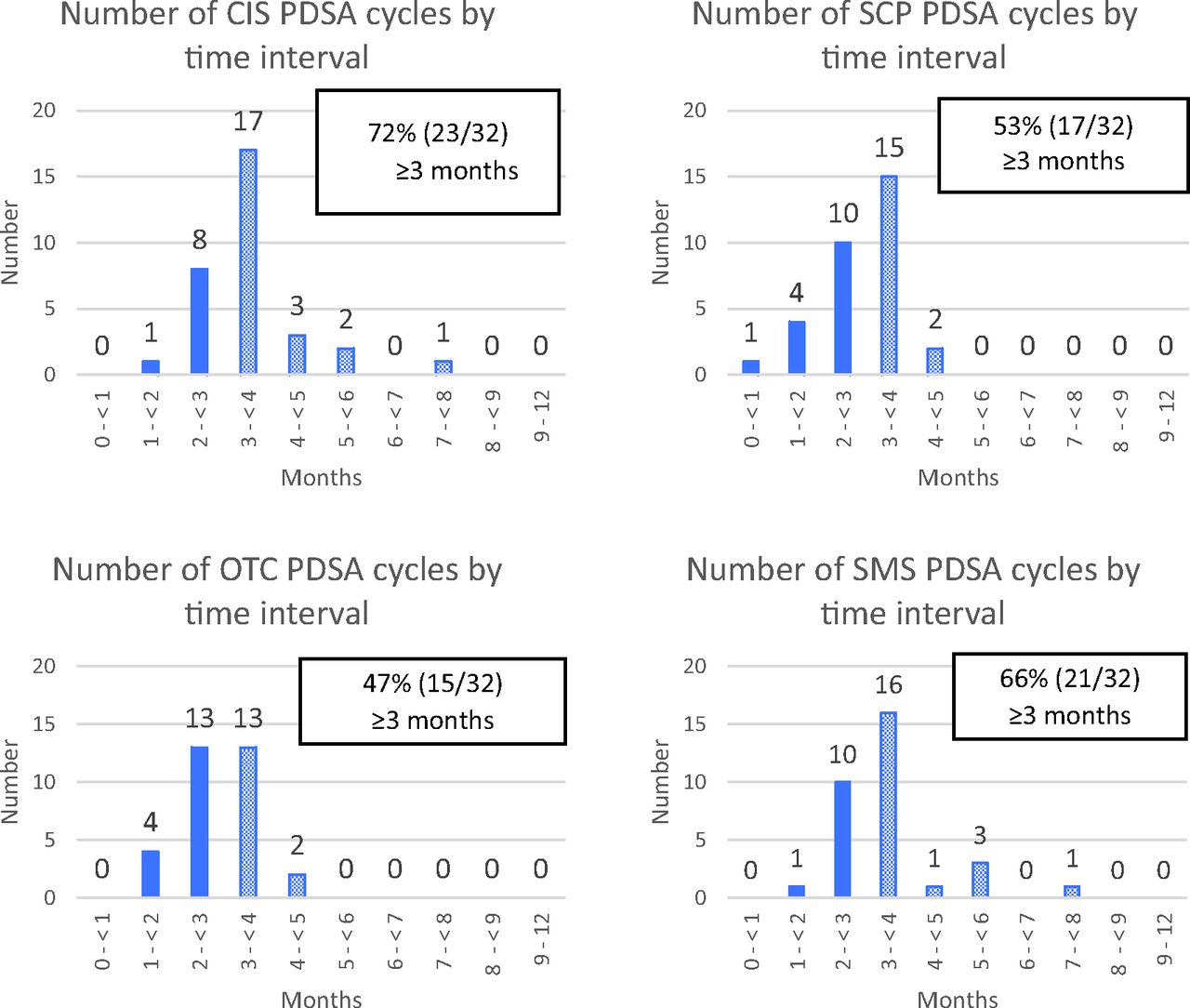
- Figure 5.
Plan, Do, Study, Act (PDSA) Cycles by Key Driver Domain in the Southeastern Collaboration to Improve Blood Pressure Control Trial. Abbreviations: CIS, Clinical Information Systems; SCP, Standard Care Processes; OTC, Optimized Team Care processes; SMS, Patient Self-Management Support.



Tables
Training Activity/Resource Details Practice Facilitator Certificate Program at Millard Fillmore College of the University at Buffalo of The State University of New York Building organizational capacity in change management
Building core competencies in using quality improvement methods (engaging practice teams in PDSAs, using data to drive change, doing workflow analysis, and using the Chronic Care Model23
40 hours of fieldwork with an experience practice facilitator mentor
Motivational Interviewing Training A half-day workshop on how to use motivational interviewing to encourage practice change, help patients with self-management support, and keep practices engaged in the research project
Twice monthly practice facilitation 1-hour long work group calls (Year 1 to 4) (Year 5 reduced to monthly) Videoconference calls to support PF work within the practice and to implement the study protocol, during which PFs shared and archived helpful resources
Specific training in health equity and how to guide practices to engage in PDSA activities that specifically focused on enhancing outcomes for African American patients
Practice Facilitation Implementation Guide designed around the Key Driver Framework Thirty-page “how to” study implementation guide for facilitators including ideas for PDSA activities to guide practices to select activities to implement, including those that focus on enhanced activities to better serve African American patients. The guide included background on the study, descriptions of the 4 Key Driver domains, and an inventory of potential QI activities nested within Key Driver domains
Other professional development activities Practice Facilitation professional development experiences and team presentations on early lessons and study findings
Attendance at The North American Primary Care Research Group's International Conferences on Practice Facilitation: November 2017, December 2018, and June 2019
PF, practice facilitation; PDSA, Plan, Do, Study, Act; QI, quality improvement.
- Table 2.
Key Driver Implementation Scale (Descriptions Have Been Shortened for Publication)
Clinical Information Systems (CIS). The practice… 0 currently does not review practice population data 1 trusts their BP data reports enough to consider implementing change activities 2 has access to reliable data on their patients with HTN 3 reviews BP data monthly, discusses how to make changes to improve processes to optimize BP control Standardized Care Processes (SCP). The practice… 0 no activity on following evidence-based protocols for HTN 1 has identified ≥ evidence-based protocol(s) for HTN, has begun customizing it for their practice 2 has no activity on following evidence-based protocols for hypertension 3 has established a workflow to implement ≥ 1 HTN protocol, and it has been tested it on a few patients 4 has implemented an evidence-based protocol for HTN, but not yet used with all patients 5 routinely fully implements ≥ 1 evidence-based protocol for HTN Optimized Team Care (OTC). The practice… 0 has no QI activities related to HTN 1 has occasional meetings/discussions about HTN QI, but no practice-wide understanding of QI 2 has a QI team that communicates regularly, plans tests, discusses results, knows project's focus/measures 3 QI team runs multiple tests simultaneously, communicates findings, and the entire office staff Self-Management Support (SMS). The practice… 0 currently has no activity on self-management support for patients with hypertension 1 staff understands the difference between patient education and self-management support 2 identifies HTN related SMS resources and incorporates the use of the resources into their workflow 3 develops tracking systems to monitor use of HTN-related SMS resources 4 care team collaborates with patients to sets, documents, and reviews HTN-related SMS goals 5 care team assess patients' confidence level related to managing their hypertension HTN, hypertension; QI, quality improvement.
- Table 3.
Characteristics of the 32 Study Practices Exposed to Practice Facilitation Services
Practice Characteristics Survey Items, [# Missing] n/Mean (%, SD, range)* Practice Size (mean, range) Number of full-time providers (MD/DO, NP, PA), 0 3.7 (0 to 21) Number of part-time providers (MD, DO, NP, PA), 0 0.9 (0 to 18) Number of other professionals (nurses, administrative/clinical support staff), 0 12.3 (2 to 53) Practice ownership type, [0 missing] (N, %) Private 11 (34.4%) Federally qualified health clinic or look-alike 15 (46.9%) Free Clinic 1 (3.1%) Part of a hospital/health system 5 (15.6%) Number of years practice has been in operation, 0 (N, range) 16 (1 to 42) Payer mix [0 missing], (% and range) Medicare 22% (0% to 60%) Medicaid 23% (0% to 50%) Dual Medicare/Medicaid 8.5% (0% to 30%) HMO, PPO, Commercial 21% (0% to 72%) Uninsured 24% (0% to 100%) Other 2% (0 %to 17%) Has received patient-centered medical home recognition, [1] (n, %) 10 (32%) Number of patient visits to providers per year, 0 (mean, range) 11,928 (1 to 100,000) Practice busyness34 (0 to 10, where 10 is most busy), 0, (mean ± SD) 7.5 ±1.7 % African American patients, 0, (mean, range) 57.5% (25% to 94%) % Hispanic/Latino patients, [4], (mean, range) 10% (0% to 60%) Number of practices with prior quality improvement project experience with chronic disease focus 0 (n, %) 27 (84%) SD, standard deviation; HMO, health maintenance organization; PPO, preferred provider organization.
↵* Data provided as absolute numbers or means and standard deviations (SD) for continuous variables and proportions as appropriate. Data rounded to tenths position.
- Table 4.
Examples of Most Engaging and Durable PDSAs (PDSAs) Activities by Key Driver Domain
Key Driver Example Activities Clinical Information Systems (CIS) Creating a practice level list and monthly reports of patients with HTN and uncontrolled HTN
Creating lists of hypertensive patients without recent visits or with uncontrolled HTN at their last visit for outreach
Standard Care Processes (SCP) Instructing practice staff on guideline-concordant blood pressure measurements, including use of sound reduction equipment to provide a calm environment for patients during BP assessments and use of posters throughout the clinics demonstrating proper technique and engaging in refresher sessions to maintain focus on proper measurement technique
Working with staff to document BP in EHRs such that the data would populate HTN reports
Standardizing staff behaviors to repeat BP measurements for patients with SBP and DBP values ≥ 140 and/or ≥ 90 mm Hg
Optimized Team Care processes (OTC) Holding group QI meetings with attendance where data review and improvement activities were devised
Creating HTN control educational videos for patients related to nutrition, lifestyle, and medication adherence
Weekly huddles to identify patients with uncontrolled BP and those requiring extra support; instituting processes for making follow-up phone calls to check on patient's engagement in their own care and reporting out of office BP measurements back to staff
Having all clinic staff wear different HTN control messages on their clothing such that a unique message is shared by each staff member who interacts with patients during visits.
Patient Self-Management Support (SMS) Patients' use of BP log cards to document out-of-office BPs and instructing clinical staff on how to address noted BP trends that may be related to stress, lack of medication adherence, etc.
Use of refrigerator magnets to remind patients to check their BPs, know their goal BPs, and engage in healthy lifestyle activities
Use of “kudos” cards given to patients at subsequent office visits when BP's were improved
Use of “Teach Back” methods with patients
Engaging in patient goal setting activities
Providing a raffle in clinic waiting rooms to receive a home BP monitor as a way to promote home monitoring and self-management
BP, blood pressure; EHR, electronic health record; HTN, hypertension; SBP, systolic blood pressure; DBP, diastolic blood pressure; QI, quality improvement.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}