
Abstract
Introduction: Genetic screenings can have a large impact on enabling personalized preventive care. However, this can be limited by the primary use of medical history-based screenings in determining care. The purpose of this study was to understand the impact of DNA10K, a population-based genetic screening program mediated by primary care physicians within an integrated health system to emphasize its contribution to preventive healthcare.
Methods: Construction of the patient experience as part of DNA10K shaped the context for PCP engagement within the program. A cross-sectional analysis of patient consents, orders, tests, and results of nearly 10,000 patients within the primary care specialties of family medicine, internal medicine or obstetrics/gynecology between April 1, 2019 and January 22, 2020 was conducted.
Results: Across all specialties, a median number of 7.5 cancer and cardiovascular disease variants per PCP was found. The average age of the study population was 49.6 years. Over 8% of these patients had at least one actionable genetic risk variant and almost 2% of patients had at least one CDC Tier 1 variant. The median numbers of patients per PCP with either hereditary breast and ovarian cancer, Lynch Syndrome, or Familial Hypercholesterolemia was 1 (Interquartile Range 0-2).
Discussion: The analysis of test results and the engagement of an integrated healthcare system in the implementation of a genetic screening program suggests that it can have a large impact on population health outcomes and minimal referral burden to PCPs if identified risks can lead to preventive care.
- Chronic Disease
- Cross-Sectional
- Studies
- Genetic Testing
- Genomics
- Integrated Health Care Systems
- Primary Care Physicians
- Primary Health Care
Introduction
Genetic testing for pathogenic variants that confer susceptibility for cancer and heart disease—the 2 most common causes of death in the United States (US)—has the potential to guide individualized disease prevention, treatment, and risk identification. Primary care physicians (PCPs) play a pivotal role in preventive services, such as applying family histories in identifying high genetic risk for disease. However, medical history-based screening can under-detect pathogenic cancer syndromes, such as hereditary breast and ovarian cancer (HBOC), Lynch syndrome, and familial hypercholesterolemia (FH),1⇓–3 3 conditions present in at least 1% of the US population considered by the Centers for Disease Control and Prevention (CDC) to be of high public health importance (CDC Tier 1 applications). The purpose of this study was to characterize the impact of PCP engagement in a population genetic screening program (DNA10K) by analyzing patient participation and test results.
Methods
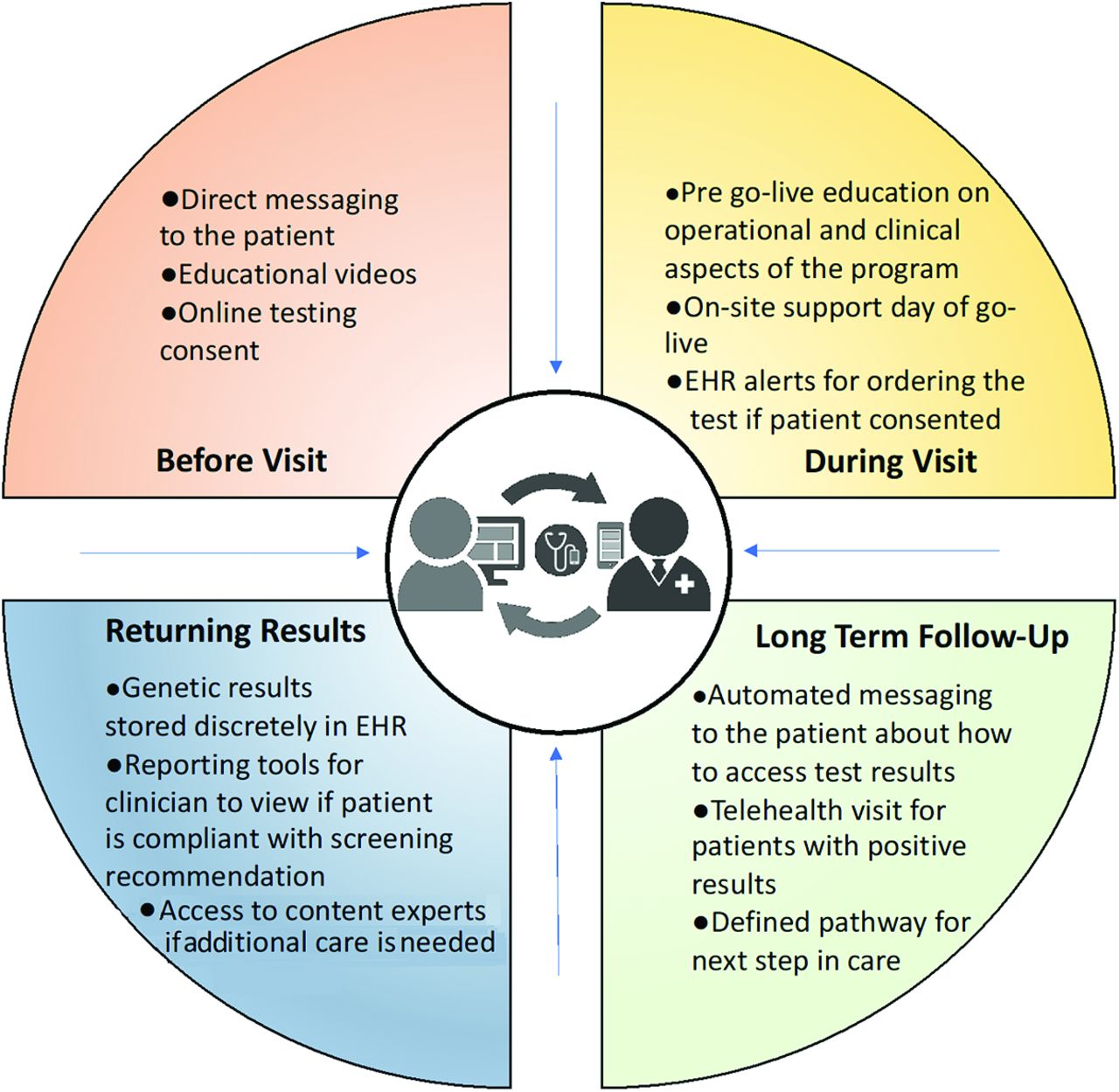
DNA10K was conducted within an integrated health care system to provide genomics-guided care to more than 10,000 patients by their PCPs (n = 116) in family medicine (FM), internal medicine (IM), and obstetrics/gynecology (OBGYN) across 14 clinical practice locations in northern Cook and Lake Counties, Illinois. The context of the DNA10K implementation is described in Figure 1.
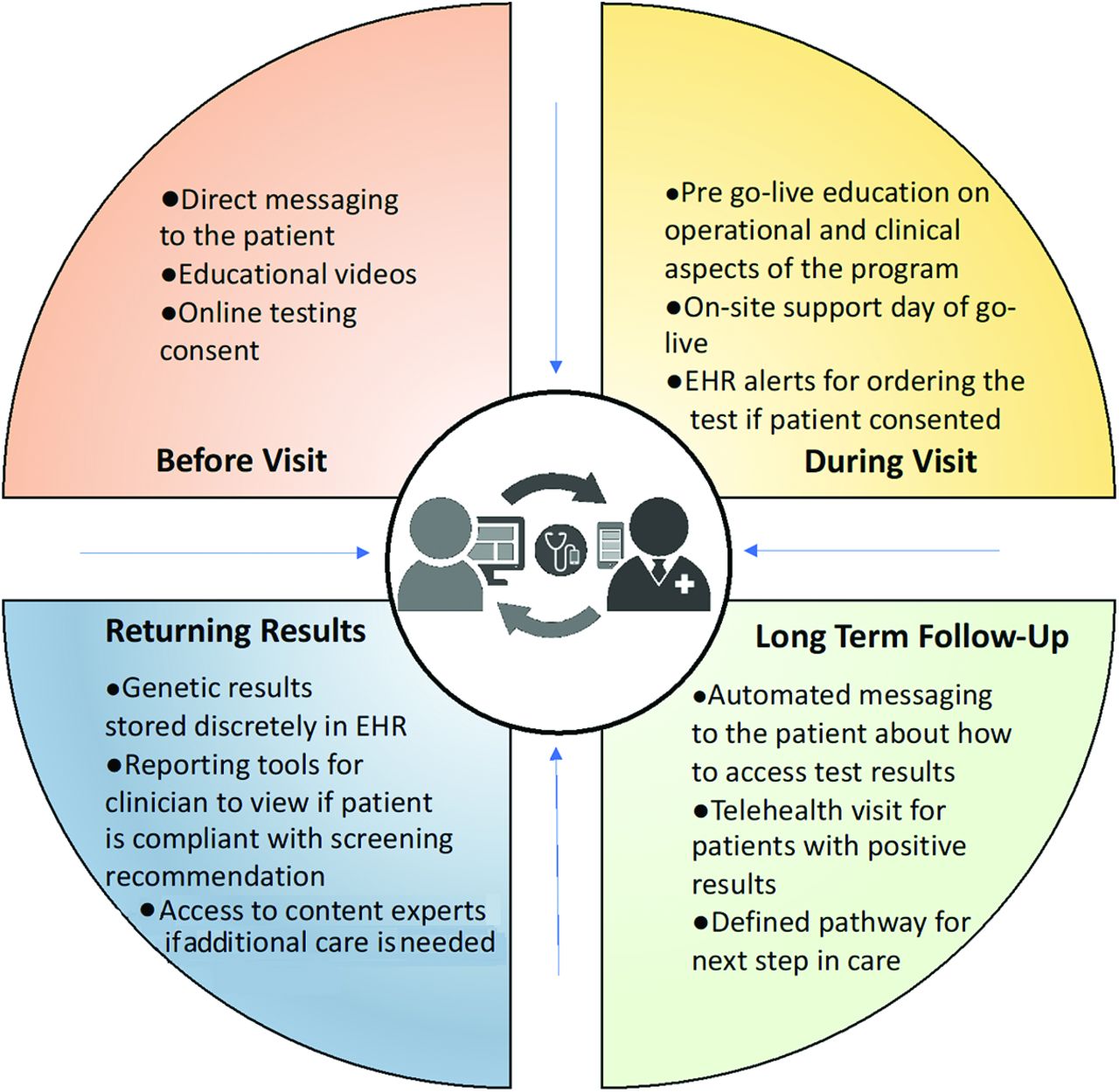
Context for Supporting PCP Engagement in Population Genetic Screening. Figure Legend: The NorthShore Center for Personalized Medicine DNA10K program consisted of multiple components. (a) patient educational video and consent via the NorthShore Connect (NSC) patient portal, (b) PCP electronic clinical decision support and electronic health record (EHR) order, (c) access to a NorthShore lab for phlebotomy, (d) Color Genomics, Inc. genetic testing using a 74 gene next-generation sequencing panel, (e) discrete reporting of results available in the EHR, (f) coordination of results with PCP health maintenance visits, (g) automated patient messaging about next steps, (h) access to genetic counseling, (i) return of results on the patient portal, and (j) clinical follow-up with PCP and specialists. The NorthShore Institutional Review Board approved this study as an exempt quality improvement evaluation. Abbreviations: PCP, primary care physician; EHR, electronic health record.
A cross-sectional analysis of consents, orders, tests, results, and actionable genetic variants of patients who were genotyped between April 1, 2019, and January 22, 2020, was conducted. Medians and interquartile (IQR) ranges of genetic test result frequencies per PCP are reported at the overall and specialty levels for cancer and cardiovascular pathogenic variants, Tier 1 pathogenic variants,1 non-Tier 1 pathogenic variants, and the percentage of actionable pharmacogenomic variants.4 Group differences for demographics and test results were examined using Kruskal-Wallis, ANOVA with posthoc Tukey's honestly significant difference (HSD) test, and Wilcoxon Rank Sum tests in Statistical Analysis System (SAS) version 9.4 (Cary, NC) with P < .05 being considered significant.
Results
Overall, 49,413 patients were contacted. Of those who consented (n = 14,063), 77.7% (n = 10,933) had an order placed by a PCP and 89.6% (n = 9,797) of these patients completed testing. Mean age of the participants was 49.6 years. An additional 442 patients completed testing ordered by medical geneticists and other specialists (DNA10K total n = 10,239). Table 1 presents stratified results by primary care specialty for DNA10K participants. A total of 813 (8.3%) patients had at least 1 actionable genetic risk variant (excluding pharmacogenomics), and 182 (1.9%) patients had at least 1 CDC Tier 1 variant. HBOC variants were present in 116 patients (1.2%), Lynch syndrome in 38 (0.39%) patients, and FH in 29 (0.3%) patients. More than 99% of patients (9599 of 9607) had at least 1 actionable pharmacogenomic variant. The median number of participants per PCP ranged from 62.5 (IQR, 33 to 120) for FM, 66 (IQR, 22.5 to 138) for IM, and 75 (IQR, 40 to 118.2) for OBGYN. Median numbers of patients per PCP with at least 1 CDC Tier 1 variant or at least 1 actionable cancer or cardiovascular disease variant is 1 (IQR, 0 to 2) and 5 (IQR, 1 to 10), respectively. No statistically significant differences were observed per specialty PCP for analyzed test results.
DNA10K Primary Care Physician-Mediated Genetic Screening Results*
Discussion
In this study, the engagement and implementation of a genetic screening program in an integrated health system enabled PCPs to identify cancer and cardiovascular disease variants in more than 8% of patients and at least 1 CDC Tier 1 variant in nearly 2% of patients. Limitations included the lack of detailed patient family histories, which restricted an evaluation of its sensitivity. In addition, there was not sufficient follow-up time to assess the effects of testing on downstream screenings (eg, mammography, colonoscopy, lipid testing, genetics referrals, and medical outcomes). However, results suggest PCP-guided population-based genetic screenings could complement routine family histories to identify high genetic risks for cancer and cardiovascular disease.
Acknowledgments
We wish to acknowledge the leadership of John Revis, MD, Janardan Khandekar, MD, and Justin Brueck, MHA at NorthShore University HealthSystem (Evanston, IL), NorthShore Health Information Technology and EPIC Ambulatory Team for information technology EMR integration work, Alicia Zhou, PhD at Color Genomics Inc. (Burlingame, CA) for support, and EPIC Systems™ (Verona, WI) for assistance with delivery of genomic services and EMR integration.
Notes
This article was externally peer reviewed.
Funding: The DNA10K initiative is funded by the Transformation through Innovation Fund at NorthShore University HealthSystem. Additional funding to Dr. David from the NorthShore Auxiliary Research Award and National Institute on Minority Health and Health Disparities grant no. U54MD010724.
Conflict of interest: Dr. David acts as a scientific advisor to Genalyte, Inc. (San Diego, CA). Dr. Zimmer is employed by and owns stock in Color Genomics, Inc. (Burlingame, CA). No other disclosures were reported.
To see this article online, please go to: http://jabfm.org/content/34/4/861.full.
- Received for publication July 23, 2020.
- Revision received July 24, 2020.
- Accepted for publication September 29, 2020.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Applying health equity implementation science frameworks to population genetic screening
- Diagnostic yield of genetic screening in a diverse, community-ascertained cohort
- The Contribution of Pharmacogenetic Drug Interactions to 90-Day Hospital Readmissions: Preliminary Results from a Real-World Healthcare System
- Family Medicine Research on Health Equity, Addiction, and Eating Breakfast--Just for Starters