
Abstract
Background: During the Coronavirus disease 2019 (COVID-19) pandemic, wearing facemasks became obligatory worldwide.
Objectives: The objective of this study was to evaluate the effects of facemasks on gas exchange.
Methods: Healthy adults were assessed at rest and during slow and brisk 5-minute walks, with and without masks. We monitored O2 saturation, end-tidal carbon dioxide (EtCO2), and heart and respiratory rates. Participants graded their subjective difficulty and completed individual sensations questionnaires.
Results: Twenty-one participants with a median age of 38 years (range, 29–57 years) were recruited. At rest, all vital signs remained normal, without and with masks. However, during slow and brisk walks, EtCO2 increased; the rise was significantly higher while wearing masks: slow walk, mean EtCO2 (mmHg) change +4.5 ± 2.4 versus +2.9 ± 2.3, P = .004; brisk walk EtCO2 change +8.4 ± 3.0 versus +6.2 ± 4.0, P = .009, with and without masks, respectively. Wearing masks was also associated with higher proportions of participant hypercarbia (EtCO2 range, 46–49 mmHg) compared with walking without masks, though this was only partially significant. Mean O2-saturation remained stable (98%) while walking without masks but decreased by 1.2 % ± 2.2 while walking briskly with a mask (P = .01). Mild desaturation (O2 range, 93% to 96%) was noted during brisk walks among 43% of participants with masks, compared with only 14% without masks (P = .08). Borg's scale significantly increased while walking with a mask, for both slow and brisk walks (P < .001). Sensations of difficulty breathing and shortness of breath were more common while walking with masks.
Conclusion: While important to prevent viral spread, wearing facemasks during brisk 5-minute walks might be associated with mild hypercarbia and desaturation. The clinical significance of these minor gas exchange abnormalities is unclear and should be further investigated.
Introduction
During the Coronavirus disease 2019 (COVID-19) pandemic, facemasks became ubiquitous worldwide to protect against viral spread.1⇓–3 Concurrently, warnings against mask potential harmful effects, including hypoxemia and hypercarbia, appeared. The World Health Organization stated4 that “people should not wear masks while exercising,” yet no real-life experimental supporting evidence was found. This study evaluated the effects of a standard surgical facemask on respiratory physiology in healthy individuals.
Methods
Healthy adult volunteers were recruited. Vital signs, oxygenation, and ventilation were monitored under 3 different conditions: (a) at rest, (b) during a slow walk (4 km/h), and (c) during a brisk walk (7 km/h), with the latter 2 on a standard treadmill at 0° inclination. Each segment lasted 5 minutes, and each was performed twice—in random order—once without, and once with, a standard disposable surgical facemask (Non-Woven 3-ply FaceMask, LeJian Protective Equipment, China). A 5-minute recovery period was allocated between segments. The room settings were 25°C with 48% humidity.
Using a Welch Allyn 300 Vital Signs Monitor, we documented heart rate and oxygen saturation continuously; carbon dioxide was measured end-tidally (EtCO2) using LifeSense II (Nonin Medical Inc., Minneapolis, USA) via nasal prongs. This device also measured respiratory rate. Values were registered at 0 minutes, 2 minutes, 4 minutes, 5 minutes, and at recovery end.
Normal CO2 was defined as 35–45 mmHg; Normal oxygen saturation was defined as ≥97%.5,6
Participants rated their subjective difficulty using Borg's Exertional Scale,7 an established numeric tool (range, 1 to 10), measuring the combined feeling of effort and exertion, breathlessness, and fatigue during physical work. Furthermore, participants graded their individual sensations, comparing the same activity, with versus without a mask, namely: difficulty breathing, shortness of breath, “choking” feeling, headache, dizziness, and weakness.
Data were analyzed using SPSS, version 25 (SPSS Inc; Armonk, NY). Results are presented as mean±standard deviation (SD) or median+range according to variable distribution. For comparison of parameters measured with versus without a mask, paired-samples t -test was used when normal distribution was assumed; otherwise, a Wilcoxon rank-sum test was used. A general linear model was used for repeated measurements analysis. Sample size was calculated using power analysis (α=0.05, 1-β=0.8). The study was approved by the organization's Institutional Research Board (RMC0325-20), and participants signed informed consent before entering the study.
Results
Twenty-one volunteers were recruited into the study. Of the 21 volunteers, 11 were female, with a median age of 38 years (range, 29–57 years), median body mass index of 24.5 (range, 20–33.6), and without underlying cardiopulmonary morbidity. During the rest, all vital signs were within normal limits among the participants, with and without a mask.
During the slow walk, respiratory and heart rates increased equally with and without a mask among the participants. A small yet statistically significant difference in EtCO2 increase was observed while wearing a mask (P = .004). Two examinees showed mild hypercarbia wearing a mask, while none without (P < .001) as shown in Table 1.
Changes in Parameter Values, Comparing Slow and Brisk Walks, With a Mask Versus Without a Mask
During the brisk 5-minute walk, we saw a statistically significant increase in EtCO2, more profoundly while wearing a mask: a mean change of 8.4 ± 3.0 mmHg versus 6.2 ± 4.0 mmHg (P = .009), from baseline of 33.5 ± 3.8 without mask, 33.9 ± 4.3 with mask, respectively (Figure 1). Three participants (14%) showed hypercarbia (EtCO2>45 mmHg; max, 48.5) while walking with a mask, compared with only 1 (5%) (EtCO2=46 mmHg) while walking without a mask (P = .60). Mean oxygen saturation remained stable while walking without a mask (98%) but decreased slightly, yet statistically significant, by 1.2% ± 2.2 while walking with a mask, from 97.9% ± 2.3 to 96.7 %± 1.9 (P = .01) (Figure 1). Nine participants (43%) demonstrated mild desaturation (O2 range, 93% to 96%) while walking with a mask, compared with only 3 (14%) who had mild desaturation (O2 range, 93% to 96%) while walking without a mask (P = .08). As anticipated for physical activity, heart and respiratory rates increased with and without a mask, similarly.
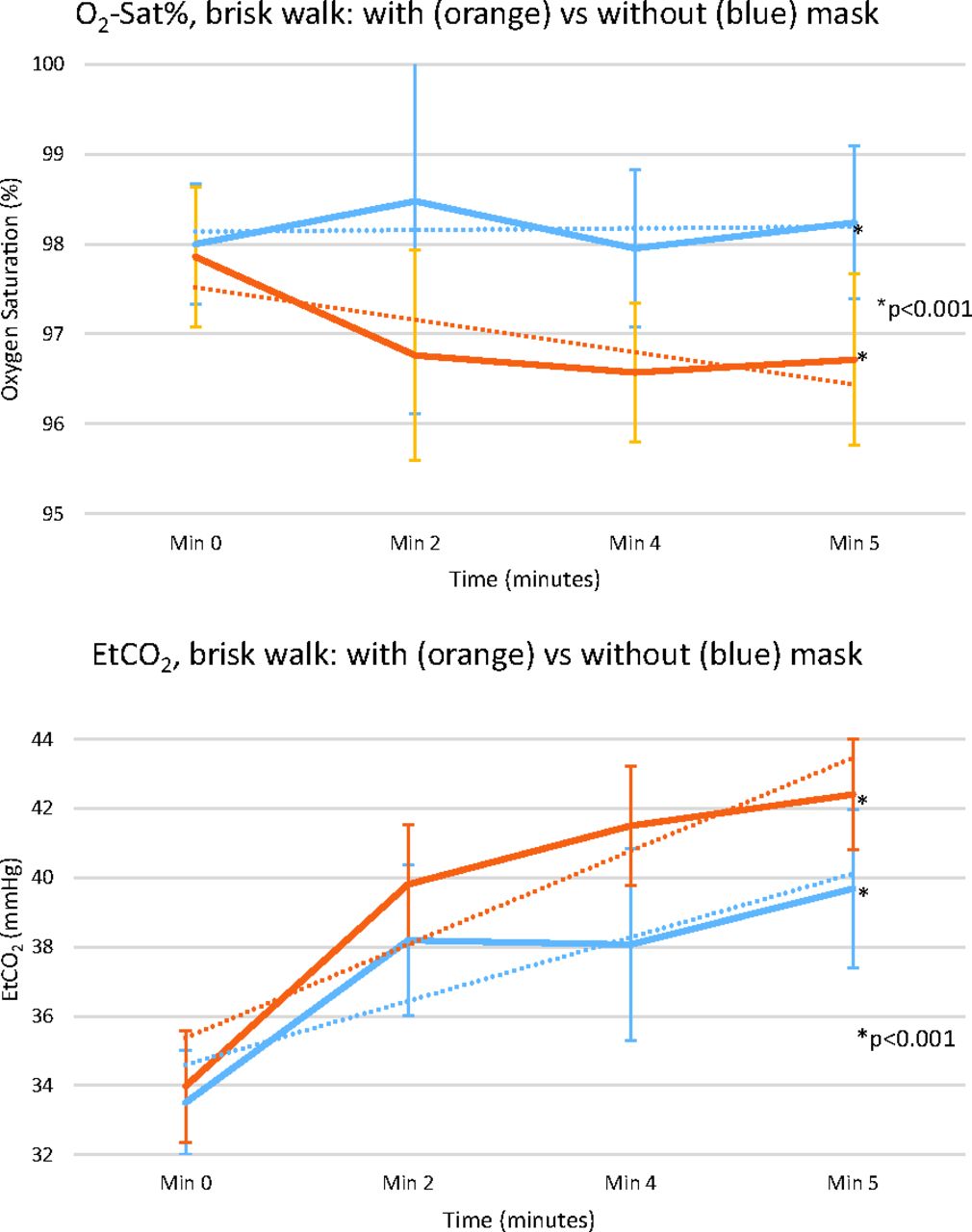
Mean O2-saturation (%) and EtCO2, during a brisk 5-minute walk, with a mask versus without a mask. Abbreviation: EtCO2, end-tidal carbon dioxide.
There was a statistically significant increase in the Borg Exertion Scale while walking with a mask for both slow and brisk walks (Table 1).
In the subjective perception questionnaire, participants described that walking briskly with a mask, compared with walking without a mask, caused “difficulty breathing” (86%), “shortness of breath” (33%), “choking” feeling (57%), and “dizziness” (19%); none of these were reported while walking without a mask.
Discussion
In this controlled trial, we demonstrated that wearing a facemask during a 5-minute walk has mild effects on respiratory parameters, causing EtCO2 to increase more profoundly than walking without a mask. In addition, oxygen saturation decreases while walking briskly with a facemask.
Most values remained within normal limits, but a subset of participants reached abnormal levels. The consequences and clinical significance of these minor gas exchange abnormalities are unclear, yet several participants reported shortness of breath and dizziness while walking briskly with a mask. The relationship between these phenomena has to be further investigated. Notably, our evaluation tested healthy volunteers and lasted only 5 minutes in an air-conditioned room.
EtCO2 probably increases due to rebreathing of expired air “trapped” in the chamber formed between the mouth and the mask. During exercise and the inevitable increase in respiratory rate coupled with increased CO2 production, there was a clearing of trapped air that was probably less effective, and perhaps even further dampened by mask warmth and humidity. This activity also increases resistance and overall work of breathing, contributing to subjective sensations of breathlessness, and increased Borg scale. A recent article by Fikenzer et al8 also demonstrated a marked negative impact of masks on exercise capacity.
These effects of breathing through a mask have not been thoroughly investigated. Kim et al9 evaluated volunteers walking calmly for 1 hour wearing an N95 mask. They observed an increase in transcutaneous CO2 (with most results remaining within normal limits), but no change in oxygen saturation. Person et al10 examined the effect of wearing a facemask on healthy individuals while performing a calm 6-Minute-Walk-Test. Distance walked, oxygen saturation, heart rate, and respiratory rate did not differ while wearing a mask. Samannan et al11 recently reported a minor influence of masks on gas exchange in healthy volunteers, and COPD patients, performing 6-minute walk tests. Rebmann et al12 evaluated nurses wearing facemasks and did not see any clinically relevant physiologic changes, although many subjective symptoms were reported.
Summary
Wearing masks is safe and important to prevent viral spread. That said, we demonstrated that wearing a surgical mask causes a mild, yet statistically significant, increase in EtCO2, as well as mild O2 desaturation, in healthy adults performing a brisk 5-minute walk in a comfortable setting.
While the abnormalities in our study may not be clinically significant, these statistically significant changes should encourage further evaluation of whether masks may cause additional gas exchange abnormalities during longer activity, especially in older people and those with comorbidities.
Acknowledgments
We thank the Gerner family who donated the Nonin LifeSense II EtCO2 monitor to the Pulmonary Institute at Schneider Children's Medical Center of Israel, in memory of their son Oz, who died of cystic fibrosis.
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/34/4/798.full.
- Received for publication October 24, 2020.
- Revision received February 24, 2021.
- Accepted for publication March 11, 2021.




{kind=link}